Le Infezioni in Medicina, n. 3, 279-283, 2025
doi: 10.53854/liim-3303-4
REVIEWS
Risk of autochthonous human schistosomiasis transmission in Italy
Andrea De Vito1, Agnese Colpani1, Giulia Moi1, Hélène Moné2, Gabriel Mouahid2,3, Daniela Fusco4, Valentina Marchese4, Giordano Madeddu1, Joachim Richter5,6
1Unit of Infectious Diseases, Department of Medicine, Surgery and Pharmacy, University of Sassari, Sassari, Italy;
2UMR 5244 IHPE Interactions Hôtes-Pathogènes-Environnements, Université de Montpellier, CNRS, IFREMER, Université de Perpignan, Perpignan, France;
3LMI Cons-Helm, UMR 261 MERIT, Institut de Recherche pour le Développement, Abomey Calavi, Benin;
4Implementation Research Group, Bernhard Nocht Institute for Tropical Medicine, Hamburg, Germany;
5Institute of International Health, Global Health Center, Charité Universitätsmedizin, Berlin, Germany;
6Swiss Tropical and Public Health Institute, Basel, Switzerland.
Article received 16 May 2025 and accepted 1 July 2025
Corresponding authors
Joachim Richter
E-mail: jockelri@gmail.com
Andrea De Vito
Email: andreadevitoaho@gmail.com
SummaRY
Introduction: Schistosoma (S.) haematobium is a widespread tropical helminthic zoonosis. Schistosomiasis was endemic in some foci in Southern Europe until the sixties of the last century. Autochthonous transmission of human schistosomiasis was first reported in the French island of Corsica in 2014, and the schistosome responsible for this emergence was also linked to partial hybridisation between S. haematobium and the bovine schistosome species S. bovis. Transmission has recently been retrospectively confirmed in southern Spain as well.
Risk of introduction of schistosomiasis to Italy: The distance between southern Corsica and northern Sardinia is 12 km. The freshwater snail Bulinus (B.) truncatus, one of the intermediate mollusc hosts of S. haematobium, is known to be endemic in some regions of southern Europe, including Corsica, Spain, and Portugal, where it transmits the zoonotic S. bovis. B. truncatus appears still to be endemic in Sardinia and possibly also in Sicily. Furthermore, schistosomiasis of ungulates caused by S. bovis, transmitted by the same vector snail, also appears to be endemic in Sardinia. Migrant populations and returnees to Italy have been found to be infested with schistosomes, and tourism to local freshwater bodies is increasing.
Discussion and conclusions: There is a considerable potential risk of autochthonous schistosomiasis being introduced to Italy. Therefore, surveillance has to be intensified to prevent the establishment of an autochthonous transmission cycle of human schistosomiasis in Italy. Systematic screening strategies for individuals who have been possibly exposed to endemic areas need to be established. Curative treatment of identified cases is mandatory. Praziquantel, the drug of choice, needs to be readily available throughout Italy.
Malacological surveillance of snail populations focusing on potential transmission sites is recommended. A one-health approach is recommended to verify the actual epidemiological situation of autochthonous S. bovis infestation and, thereby, to investigate the risk of establishing a zoonotic reservoir. Clinicians should be aware that, in some circumstances, schistosomiasis may occur in individuals who have never travelled to known endemic areas before.
Keywords: schistosomiasis, Schistosoma haematobium, urinary schistosomiasis, genital schistosomiasis, Schistosoma bovis, Bulinus truncatus, Planorbarius metidjensis, zoonosis.
INTRODUCTION
Schistosoma (S.) haematobium was endemic in some foci in southern Europe, such as Portugal and Greece, until the 1960s of the last century [1, 2]. Autochthonous transmission of human schistosomiasis was first reported in the French island of Corsica in 2014, and the schistosome responsible for this emergence was identified as a hybrid between S. haematobium and S. bovis [3, 4]. Until now, we do not know whether this hybridization is ancient or still ongoing. The ongoing transmission was confirmed to occur in southeastern Corsica, specifically in the Cavu River and the Solenzara River [5, 10-12].
Italy, in particular, Sardinia, has a comparable climate to Corsica. The distance between the two islands is 12 km. The freshwater snail Bulinus truncatus, a vector of S. haematobium, is endemic in some regions of southern Europe, including Corsica, Spain, and Portugal, where it transmits the zoonotic Schistosoma bovis [13-19]. In Italy, specifically in Sardinia and Sicily, Bulinus truncatus remains endemic [20]. Furthermore, schistosomiasis in ungulates, caused by Schistosoma bovis, which is endemic in Sardinia, is transmitted by the same vector snail [21, 22]. However, no recent official data are available regarding the presence of Bulinus truncatus in Sardinia. Anecdotal evidence, such as photographs shared by users on an online forum dedicated to Mediterranean biodiversity, suggests that Bulinus truncatus is still present on the island [23]. This forum is used by naturalists and amateur biologists who often share geo-referenced photographs of local fauna, including mollusks. Therefore, we aim to evaluate the risk of autochthonous transmission of human schistosomiasis in Italy, with a particular focus on Sardinia, by analyzing environmental, parasitological, and epidemiological data. We conducted a narrative review, synthesizing peer-reviewed publications, historical records, surveillance data, and supporting grey literature, including unpublished data and expert field observations. We also considered ecological factors, host–vector–parasite interactions, and socio-demographic trends relevant to schistosomiasis transmission dynamics in southern Europe.
THE LIFE CYCLE OF SCHISTOSOMES
The life cycle of schistosomiasis involves a definitive mammalian host and an intermediate vector mollusc. The definitive human host becomes infested in freshwater bodies when the swimming larvae, called furcocercariae, actively penetrate the intact skin. Subsequent stages include juvenile schistosomula, which circulate in the human blood vessels until they reach the portal vessels in the liver. Here, female and male mate and swim as a worm pair via the splanchnic and intestinal vessels until they reach the intestinal capillaries or, via the plexus haemorrhoidarius, the capillaries of the bladder. Here, the female worms lay ova which are excreted with urine and/or the feces of the host. When the eggs are excreted into a freshwater body, ciliated larvae called miracidia hatch from the egg and swim towards a snail vector. The larvae actively penetrate the snail, undergo several multiplication stages, and develop into furcocercariae, which are subsequently released from the snail and swim towards the definitive host.
FACTORS FOR THE ESTABLISHMENT OF AN AUTOCHTHONOUS HUMAN SCHISTOSOMIASIS TRANSMISSION
Factors required for the establishment of an autochthonous Human schistosomiasis transmission include
– The infested definitive mammalian host.
– The excretion of ova into a freshwater body.
– The existence of specific vector snails in the freshwater body.
– The exposure of the human host to the freshwater body.
– The capacity of vector snails and schistosomes to overwinter.
• Migrants infested with S. haematobium have been identified through screening in Italy, including the island of Sardinia [13, 24]. Bovines were found infested by S. bovis in Torpè village, with two of three infested by S. bovis, and in Ballao village, two of two infested by S. bovis [15, 25, 26]. In the villages of Posada, Budoni, Irgoli, Tortoli, and Bari Sardo, none of the 21 bovines and the 15 ovines analyzed were found infested by S. bovis. The presence of both S. haematobium arriving from outside Sardinia and of an autochthonous S. bovis gives the possibility of reproducing the same scheme as in Corsica, with a hybrid form of schistosome in Sardinia.
Tourists and expatriates from endemic areas are also at risk of schistosomiasis in Europe and Italy [27-29]. Although they represent a smaller proportion of schistosomiasis cases diagnosed in Europe and have different clinical presentations (often acute schistosomiasis), they remain a potential reservoir of infestation, as demonstrated by the outbreak in Corsica, also due to the ease of movement within the European continent [30].
• Excretion of eggs (from urine and/or feces) into freshwater bodies could happen in Sardinia, from humans, from ruminants, but also rodents as it is the case in South Benin [31, 32].
• Bulinus truncatus, the freshwater snail, is most probably present in Sardinia. The latest scientific report was published in 2012 [33]. On an internet blog, a photo of a Bulinus snail was taken in 2007. Another conceivable vector snail, Planorbarius meditjensis, formerly implicated in the transmission of schistosomiasis in Portugal, Spain, and Morocco but absent from Corsica, would also need to be looked for in Sardinia [14, 15].
Indirect confirmation of the possibility of a permanent autochthonous life cycle is the presence of local Schistosoma bovis endemicity in local domestic animals such as bovines and ovines, because the same vector snails transmit the latter schistosome species. S. bovis was collected from bovines in the South-East part of Sardinia (Ballao village) [25, 26, 34, 35]. Two experimental studies of the cercarial shedding rhythm of S. bovis showed that (i) the Sardinian population emerged from its Bulinus truncatus snail host significantly earlier than the Sudanese and Spanish populations, supporting the existence of genetic variability of the emergence rhythms and (ii) that the cercarial emission is situated early in the morning (peak at 8 am). The chronotype of S. bovis in Sardinia indicates that, at the time (1986), S. bovis was not interacting with S. haematobium (indeed, when both schistosomes interact, the cercarial emission pattern exhibits at least two peaks) [31, 32].
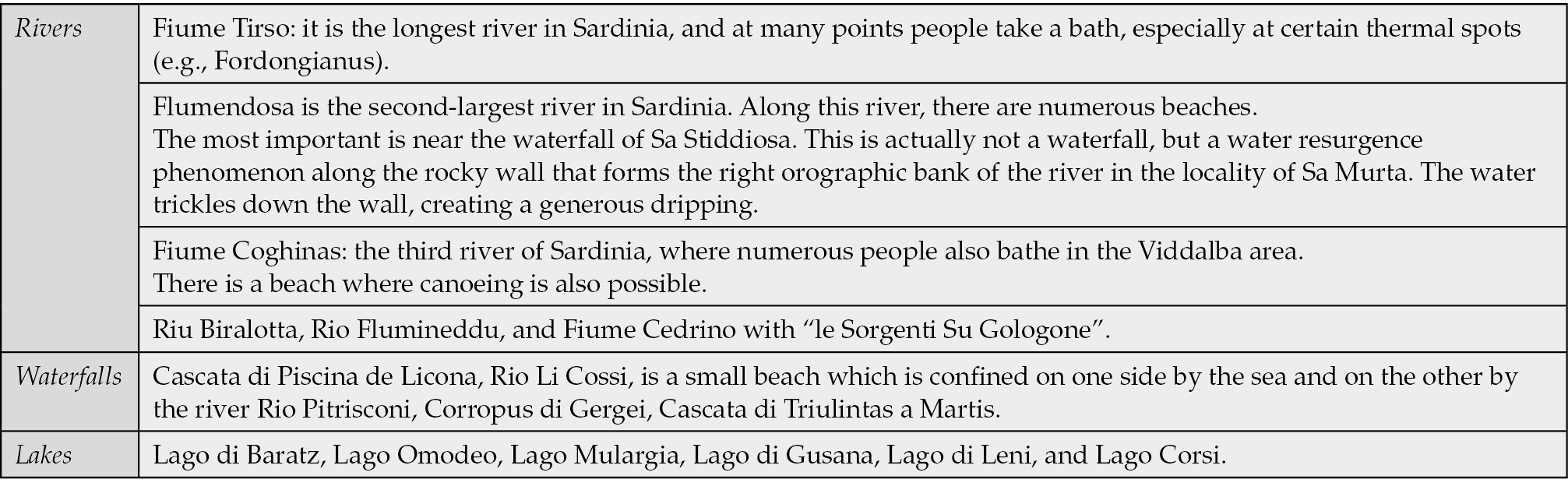
• Tourists taking baths in freshwater bodies, such as those found in Corsica, are far less common in Italy compared to Corsica. Conceivable transmission sites, however, are found, for example, in the Barbagia region of Sardinia. Several freshwater sites in Sardinia are popular for bathing and may serve as potential transmission foci (Table 1). Bulinus truncatus was found in the Barbagia region of Sardinia, in the villages of Suaredda (San Teodoro) and Ballao, as well as in the Flumendosa and Bari Sardo rivers [26]. Prevalence was, from North to South, 0.3%, 0%, 0%, 0% and 11.3% in Suaredda, Bari Sardo, Flumendosa and Ballao, respectively (Mouahid and Moné, unpublished data obtained during August 1986 in collaboration with Efisio Arru from the University of Sassari).
Table 1 - Open freshwater bodies in Sardinia as potential transmission sites of schistosomiasis.
• Bulinus truncatus is a snail that is known to resist the winter temperatures in Mediterranean countries, including Italy, France, Spain, and Portugal [21]. The schistosomes were thought not to be capable of overwintering inside the snails, but they can survive the winter easily inside the mammalian host. A recent study confirmed, however, that schistosomes insider snails can resist temperatures as low as 4°C [36]. Another risk factor is climate change, which is favorable to the establishment of a life cycle. There is circumstantial evidence of the influence of climate change by the observation that Napoleon’s troops who returned from Egypt in 1798 with urinary schistosomiasis did not cause an outbreak of schistosomiasis in Europe, namely in Corsica [37].
Concluding, in Italy, specifically in Sardinia, a situation similar to that in Corsica may occur, where local vector snails are present and humans, whether adults or children, who may not be aware of their infestation, infest these snails, introducing the possibility of permanent autochthonous transmission of schistosomiasis. To prevent this from happening, systematic screening of migrant populations and returnees from endemic areas, as well as treatment for those who are infested, is necessary. For first-line screening of potentially exposed individuals, particularly migrants and returnees from endemic regions, urine reagent strips (e.g., hematuria dipsticks) are a rapid, low-cost, and scalable tool suitable for field use. In individuals with a positive or high-risk status, parasitological confirmation via urine filtration microscopy or serological testing (e.g., ELISA and/or immunochromatography) should be performed to confirm the diagnosis and guide treatment. Additionally, malacological surveillance of potential transmission sites is necessary to assess the snail population in these areas. Education about schistosomiasis and its chronic forms should be strengthened among healthcare workers [38]. Clinicians should be aware of the possibility that, in some circumstances, schistosomiasis may occur in individuals who have never travelled to known endemic areas. Additionally, the disease could not be detected via conventional screening and diagnostic methods when it is in its chronic stage.
Conflict of interest
None declared.
Funding
There was no financial support.
REFERENCES
[1] França C. A preliminary note on Bilharziosis indigenous in Portugal. Trans R Soc Trop Med Hyg. 1921; 15: 180-181.
[2] Bustinduy AL, Richter J, King CH. Chapter 57: Schistosomiasis. Manson’s Tropical Diseases -Twentyfourth Edition. 2024: 706-733.
[3] Moné H, Holtfreter MC, Allienne JF, et al. Introgressive hybridizations of Schistosoma haematobium by Schistosoma bovis at the origin of the first case report of schistosomiasis in Corsica (France, Europe). Parasitol Res. 2015; 114: 4127-4133.
[4] Holtfreter MC, Moné H, Müller-Stöver I, et al. Schistosoma haematobium infections acquired in Corsica, France, August 2013. Eurosurveillance. 2014; 19: 20821.
[5] Rothe C, Zimmer T, Schunk M, et al. Developing endemicity of schistosomiasis, Corsica, France. Emerg Infect Dis. 2021; 27: 319-321.
[6] Noël H, Ruello M, Maccary A, et al. Large outbreak of urogenital schistosomiasis acquired in Southern Corsica, France: monitoring early signs of endemicization? Clin Microbiol Infect. 2018; 24: 295-300.
[7] Ramalli L, Mulero S, Noël H, et al. Persistence of schistosomal transmission linked to the cavu river in southern Corsica since 2013. Euro Surveill. 2018; 23(4): 18-00017.
[8] Beltrame A, Buonfrate D, Gobbi F, et al. The hidden epidemic of schistosomiasis in recent African immigrants and asylum seekers to Italy. Eur J Epidemiol. 2017; 32: 733-735.
[9] Boissier J, Grech-Angelini S, Webster BL, et al. Outbreak of urogenital schistosomiasis in Corsica (France): an epidemiological case study. Lancet Infect Dis. 2016; 16: 971-979.
[10] Berry A, Moné H, Iriart X, et al. Schistosomiasis haematobium, Corsica, France. Emerg Infect Dis. 2014; 20: 1595-1597.
[11] Wellinghausen N, Moné H, Mouahid G, et al. A family cluster of schistosomiasis acquired in Solenzara River, Corsica (France) - Solenzara River is clearly a transmission site for schistosomiasis in Corsica. Parasitol Res. 2022; 121: 2449-2452.
[12] Saint F, Boissier J, Arnaud P, et al. Urinary schistosomiasis: The Corsican file. Fr J Urol. 2025; 35(1): 102799.
[13] Gabrielli AF, Garba Djirmay A. Schistosomiasis in Europe. Curr Trop Med Rep. 2023; 10: 79-87.
[14] Calavas D, Martin PMV. Schistosomiasis in cattle in Corsica, France. Emerg Infect Dis 2014; 20: 2163-2164.
[15] Moné H, Mouahid G, Morand S. The Distribution of Schistosoma bovis Sonsino, 1876 in Relation to Intermediate Host Mollusc–Parasite Relationships. Adv Parasitol. 1999; 44: 99-138.
[16] Doby JM, Rault B, Deblock S, et al. [Snails and bilharziasis in Corsica. Distribution, frequency and biology of “Bulinus truncatus”]. Ann Parasitol Hum Comp. 1966: 337-339.
[17] Brumpt E. Cycle évolutif complet de Schistosoma bovis - Infection naturelle en Corse et infection expérimentale de Bulinus contortus. Ann Parasitol Hum Comp. 1930; 8: 17-50.
[18] Dollfus RP. Sur la presence en France et en Corse du Bulinus contortus (Michaud), hôte intermmédiaire de Schistosoma haematobium (Bilharz). Extrait Du Bulletin de La Societé de Pathologie. 1922: 207-212.
[19] Grétillat S. Rapport sur une mission effectuée en Corse au sujet de l’épidémiologie de certaines affections à trématodes des animaux domestiques (bilharziose bovine et distomatose bovine et ovine). Annales de Parasitologie Humaine et Comparee. 1962; 38: 471-481.
[20] Mouahid A, Moné H, Arru E, et al. Analyse comparative du rythme d’émission des cercaires de trois souches de Schistosoma bovis. Parassitologia. 1987; 29: 79-85.
[21] Rollinson D, Stothard JR, Southgate VR. Interactions between intermediate snail hosts of the genus Bulinus and schistosomes of the Schistosoma haematobium group. Parasitology. 2001; 123 Suppl. S245-S260. doi: 10.1017/s0031182001008046.
[22] De Carneri I. Parassitologia generale e umana - Zanichelli. 11th ed. 1989.
[23] Natura Mediterraneo - Forum Naturalistico. Planorbidae Bulinus (Isidora) truncatus (Audoin 1827)-LMD n.d. https://www.naturamediterraneo.com/forum/topic.asp?TOPIC_ID=39054. (accessed May 15, 2025).
[24] Geremia N, Vito A De, Lai V, et al. Human urogenital schistosomiasis in west and sub-saharan africa migrants in sardinia, italy: A retrospective monocentric study. J Infect Dev Ctries. 2022; 16: 1359-1363.
[25] Mouahid A, Mone H. Interference of Echinoparyphium elegans with the host-parasite system Bulinus truncatus-Schistosoma bovis in natural conditions. Ann Trop Med Parasitol. 1990; 84: 341-348.
[26] Mouahid A, Moné H. Echinoparyphium elegans (Looss, 1899) (Digenea: Echinostomatidae): the life cycle and redescription of the adult with a revision of the 43-spined members of the genus Echinoparyphium. Syst Parasitol. 1988; 12: 149-157.
[27] Salvador F, Bocanegra C, Treviño B, et al. Imported schistosomiasis in travelers: Experience from a referral tropical medicine unit in Barcelona, Spain. Travel Med Infect Dis. 2024; 60:102742. doi: 10.1016/j.tmaid.2024.102742.
[28] Marchese V, Beltrame A, Angheben A, et al. Schistosomiasis in immigrants, refugees and travellers in an Italian referral centre for tropical diseases. Infect Dis Poverty. 2018; 7(1): 55. doi: 10.1186/s40249-018-0440-5.
[29] Lingscheid T, Kurth F, Clerinx J, et al. Schistosomiasis in european travelers and migrants: Analysis of 14 years tropnet surveillance data. Am J Trop Med Hyg. 2017; 97: 567-574.
[30] Gautret P, Mockenhaupt FP, Von Sonnenburg F, et al. Local and International Implications of Schistosomiasis Acquired in Corsica, France. Emerg Infect Dis 2015; 21(10): 1865-1868.
[31] Savassi BAES, Mouahid G, Lasica C, et al. Cattle as natural host for Schistosoma haematobium (Bilharz, 1852) Weinland, 1858 x Schistosoma bovis Sonsino, 1876 interactions, with new cercarial emergence and genetic patterns. Parasitol Res. 2020; 119: 2189-2205.
[32] Savassi BAES, Dobigny G, Etougbétché JR, et al. Mastomys natalensis (Smith, 1834) as a natural host for Schistosoma haematobium (Bilharz, 1852) Weinland, 1858 x Schistosoma bovis Sonsino, 1876 introgressive hybrids. Parasitol Res. 2021; 120: 1755-1770.
[33] Welter-Schultes FW. European non-marine molluscs, a guide for species identification / Bestimmungsbuch für europäische Land- und Süsswassermollusken. Planet Poster Editions. 2012.
[34] Medda A, Adamo F. [Schistosomiasis in Sardinia due to the adult forms of Schistosoma bovis (Sonsino 1876) in man]. Nuovi Ann Ig Microbiol. 1961; 12: 321-324.
[35] Biocca E. [Mollusc vectors of schistosomiasis in Sardinia and in the Mediterranean area: taxonomy and epidemiology]. Parassitologia. 1980; 22: 247-255.
[36] Mulero S, Rey O, Arancibia N, et al. Persistent establishment of a tropical disease in Europe: The preadaptation of schistosomes to overwinter. Parasit Vectors. 2019; 12.
[37] Cox FEG. History of human parasitology. Clin Microbiol Rev. 2002; 15: 595-612.
[38] Marchese V, Remkes A, Kislaya I, et al. Awareness and knowledge regarding female genital schistosomiasis among European healthcare workers: a cross-sectional online survey. Global Health. 2025; 21(1): 2.