Le Infezioni in Medicina, n. 3, 277-282, 2023
doi: 10.53854/liim-3103-2
REVIEWS
Therapy initiation and rapid start with Bictegravir/Emtricitabine/Tenofovir Alafenamide in PLWH
Andrea Antinori
Clinical Department of Infectious Diseases, National Institute for Infectious Diseases Lazzaro Spallanzani IRCCS, Rome, Italy
Article received 25 June 2023, accepted 31 July 2023
Corresponding author
Andrea Antinori
E-mail: andrea.antinori@inmi.it
SummaRY
Advanced HIV naive represents an unfavorable prognostic condition due to a persistent high risk of death, increased probability of virological failure, immunologic impairment, clinical progression, and immune reconstitution inflammatory syndrome (IRIS), cumulative adverse drug events, drug-drug interactions and increased healthcare costs.
Currently, all international guidelines recommend the rapid initiation of ART, especially in late-stage naive patients.
Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF), due to its efficacy high genetic barrier, good safety profile, and low DDI potential, is one of the regimens recommended for overall rapid initiation by international guidelines. B/F/TAF has been tested in observational or uncontrolled pilot studies (OPERA, RAINBOW), while a large randomized controlled trial is currently ongoing (LAPTOP).
In conclusion, B/F/TAF is an ideal combination for the initiation of antiretroviral therapy, particularly in the HIV late presenter or advanced HIV disease patient, even in the context of rapid start or same-day treatment regimens, where the initiation of treatment usually occurs in the absence of information on viral load, CD4 count, biochemical profile and HIV transmitted resistance.
Keywords: Bictegravir, Emtricitabile, Tenofovir, PLWH.
INTRODUCTION
Late HIV diagnosis was associated with adverse outcomes, increased risk of HIV transmission, and high healthcare costs. A 2010 consensus statement defined late HIV presentation as a presentation to care with a CD4 count <350 cells/μL or an AIDS-defining event. This definition has been used across Europe for clinical research and public health monitoring for over 10 years. Radical changes have recently been observed regarding the best time to start antiretroviral therapy (ART), in a model of an universal approach to starting therapy. CD4 cell count at the time of ART initiation has been shown to be directly related to the extent of CD4 recovery and life expectancy. It is noteworthy that, despite these main improvements, the proportion of people with advanced HIV disease still remains a major challenge.
Differently from late presentation (CD4 count less than 350 cells/mm3 or AIDS-defining event), WHO has defined advanced HIV disease for adults as CD4 cell count <200 cells/mm3 or WHO stage 3 or 4 events. Up to 20% of individuals newly diagnosed with HIV in the US have advanced HIV infection (CD4<200 cells/μL), whereas an advanced HIV infection was observed in 35% of new HIV diagnoses in Europe (9% with AIDS presentation) and in 40% of new HIV diagnoses in Italy in 2022. Advanced HIV naïve represents an unfavorable prognostic condition due to a persistent high risk of death, increased probability of virological failure, immunologic impairment, clinical progression, and immune reconstitution inflammatory syndrome (IRIS). Advanced HIV status for naïve individuals was also related to cumulative adverse drug events and drug-drug interactions and is associated with increased healthcare costs. According to observational study data, male gender, advanced age, migrant status, heterosexual intercourse, or injecting drug users (IDUs) as a mode of transmission are all factors commonly associated with late presentation and with advanced HIV disease.
Currently, all international guidelines (DHHS, WHO, IAS-USA, EACS) recommend the rapid initiation of ART, especially in late-stage naïve patients. The strategy of rapid ART initiation was supported by the evidence from randomized trials performed in resource-limited settings, in which all stages of HIV infection were evaluated. A meta-analysis conducted by Ford et al. in low-income countries, including four randomized trials, demonstrated that rapid initiation of ART (within 14 days), even in patients with advanced HIV, is superior to standard of care in terms of probability of ART initiation, patient retention in care, viral suppression, rate of AIDS progression/death and risk of HIV spread in the population by ongoing viral transmission. Furthermore, a multicentre randomized clinical trial conducted in participants with AIDS presentation in the US and South Africa demonstrated the superiority of early ART (within 14 days of initiation of treatment of acute opportunistic infection) with no increase in adverse events or loss of virological response compared to delayed ART. Unfortunately, these data are not generalizable to a different social context, which remains an important limitation of this rate of evidence. In high-income countries, data on rapid ART strategies in advanced HIV naïve people are mostly derived from retrospective observational studies, such as those led in the city of San Francisco. However, it must be considered that rapid initiation means starting ART before the results of many laboratory tests are available, which may limit the choice of ART.
Integrase inhibitors (INSTIs), co-administered with two nucleosides reverse transcriptase inhibitors (NRTIs), are recommended as first-line treatment for HIV by international guidelines [DHHS, IAS-USA, EACS]. Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF), due to its efficacy high genetic barrier, good safety profile, and low DDI potential, is one of the regimens recommended for overall rapid initiation by international guidelines. Despite the evidence on the use of B/F/TAF as a rapid start strategy, scientific evidence on the rapid initiation of antiretroviral therapy with B/F/TAF in the advanced HIV patient is still limited. A recent study showed that, in ART-naïve patients with advanced disease who started on B/F/TAF, the incidence rate of regimen discontinuation was lower compared to boosted regimens based on darunavir (DRV/b), dolutegravir (DTG) and elvitegravir/cobicistat (EVG/c).
The OPERA cohort
In the OPERA cohort, all ART-naïve adults with advanced HIV (CD4<200 cells/μL) starting a three-drug regimen of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) or a three-drug regimen of boosted darunavir (bDRV), dolutegravir (DTG) or elvitegravir/cobicistat (EVG/c) were selected. A Cox proportional hazards model was used to estimate the time required to reach a CD4 cell count ≥200 cells/μL. A linear mixed model was used to assess changes in the CD4/CD8 ratio from baseline. Inverse probability weighting was used to control for confounding factors (Figure 1). Association between regimen and a) attainment of a CD4 cell count ≥200 cells/μ3, or b) changes in CD4:CD8 ratio was investigated. Analyzing the results of the OPERA Study, among the 1,349 individuals included, those starting B/F/TAF were less likely to have a history of AIDS-defining disease, any comorbidities, or ADAP/Ryan White coverage. Compared to those starting B/F/TAF, a statistically lower probability of achieving a CD4 cell count ≥200 cells/μL was observed with bDRV (HR 0.76; 95%CI 0.60-0.96), DTG (HR 0.82; 95%CI 0.69-0.98) and EVG/c (HR 0.73; 95%CI 0.57-0.93) (Figure 1A). All groups presented a similar pattern of changes in the CD4/CD8 ratio: a rapid increase in the first 6 months, followed by a slower increase thereafter (Figure 1B). Overall, only 40 individuals (4%) achieved a normalization of the CD4/CD8 ratio (expressed as a value ≥1). The Authors concluded that among individuals with advanced HIV infection, B/F/TAF initiation was associated with a faster CD4 cell count recovery (>200 cells/μL). No difference was observed in CD4:CD8 ratio changes over time across groups. Moreover, a CD4:CD8 ratio normalization was rare with all regimens.
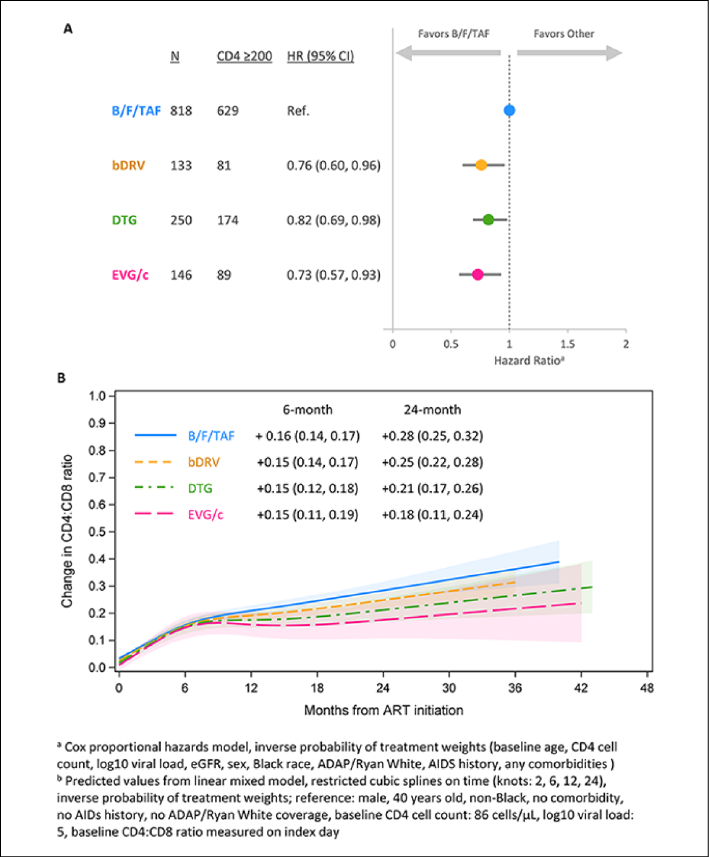
Figure 1
Association between regimen and (A) reaching a CD4 cell count ≥200 cells/μ3, or (B) changes in CD4/CD8 ratio from index. (modified from Mounzer K, et al. 24th International AIDS Conference - AIDS 2022; Abst.#EPB148).
The Rainbow Study
The aim of the Rainbow study was to evaluate the feasibility, efficacy, and safety of a rapid ART initiation strategy (within 7 days from HIV diagnosis) based on BIC/FTC/TAF in people living with HIV (PLWH) presenting with advanced HIV-1 disease, defined as a CD4+ cell count below 200 cell/mm3 and/or an AIDS-defining event. Rainbow was a pilot, single-center, single-arm, prospective, phase IV, clinical trial conducted in a tertiary care Italian hospital from the 1st of May 2020 to the 31st of December 2021. 30 ART-naive participants (Table 1), presenting at HIV-1 diagnosis with an advanced disease, described as the presence of an AIDS-defining condition and/or CD4 cell count <200 cells/μL, were enrolled in the study. Exclusion criteria were: CrCl <30 mL/min, severe hepatic impairment, active tuberculosis (TB), cryptococcosis, pregnancy or breastfeeding, and systemic cancer chemotherapy. Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) 50/200/25 mg in a single-tablet was started within 7 days of HIV diagnosis. The primary endpoint was a time-to-clinical or virologic failure (VF) (ITT analysis). Safety and feasibility were also assessed.
A total of 30 patients (Table 1) were enrolled: 16% female, 90% white, median age 45 years (38-58), 43% had CDC stage disease C, CD4 cell count was 90 cells/μL (39-147), HIV RNA log10 cp/ml 6.0 (5.4-6.4), 40% of patients had ≥1 comorbidity. The proportion of patients with HIV RNA <50 cp/mL increased from 9/30 (30%) at week 4 to 27/30 (90%) at week 48 (Figure 2). No viral rebound was observed. The proportion with CD4 >200 cells/μL increased from 2/30 (7%) at BL to 24/30 (80%) at week 48. HIV-DNA decreared, CD4/CD8 improved, BMI increased,while eGFR decreased slightly (Figure 3). There were no ART interruptions due to toxicity or VF. Three participants had 6 SAEs (4 unrelated; 2 potentially related) to B/F/TAF: one had seizures (week 4 and week 12) + PML with IRIS (week 5), two had pneumocystis pneumonia with IRIS (week 4) + pneumomediastinum (week 5); three had clinical worsening (week 1) + acute appendicitis and disseminated TB with IRIS (week 2) which required switch to different ART. There were no changes in ART based on examination of the baseline genotype (no NRTI mutations, only 3 accessory INSTI mutations [E157Q, G163K, L74I]; no INSTI major mutations).
Table 1 - Baseline demographic and clinical characteristics of the 30 patients enrolled in the Rainbow Study (modified from Camici M, et al. 24th International AIDS Conference - AIDS 2022; Abst.#EPB151).
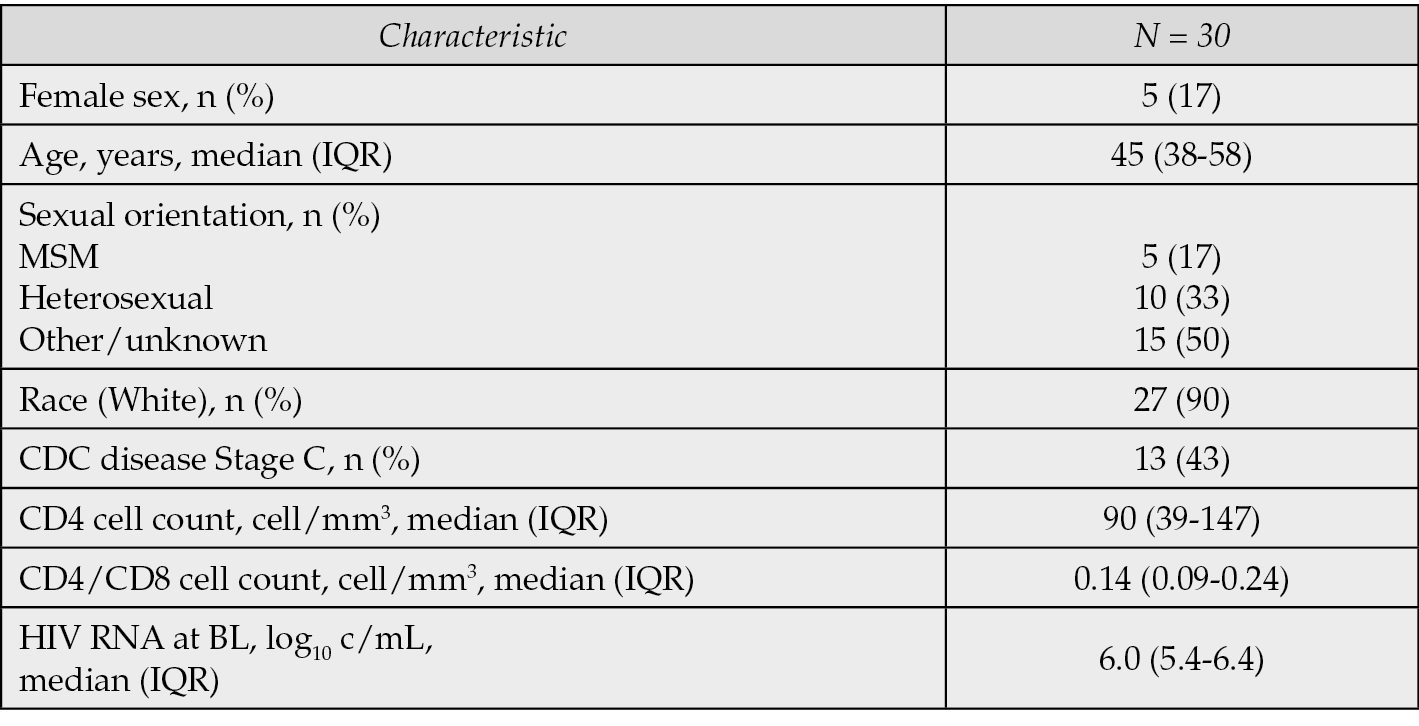
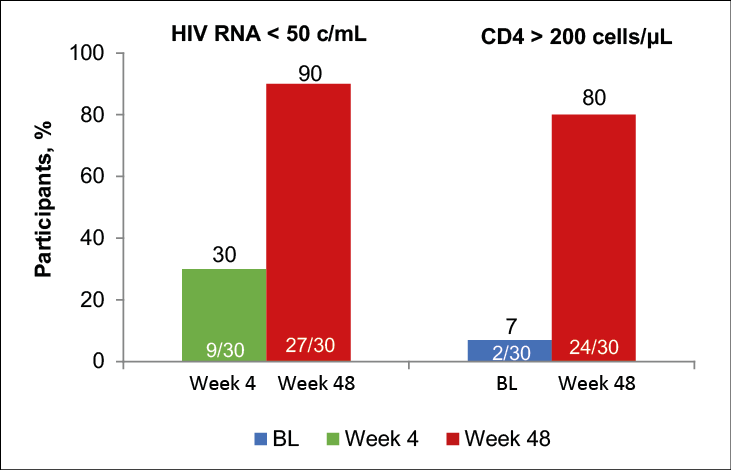
Figure 2 - Rates of Virologic Suppression and CD4 Count >200 Cells/µL in the Rainbow Study (modified from Camici M, et al. 24th International AIDS Conference - AIDS 2022; Abst.#EPB151).
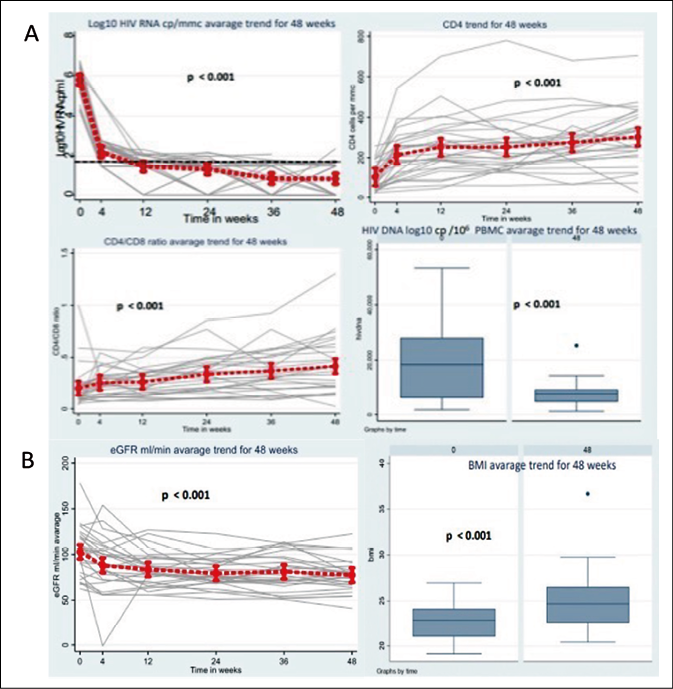
Figure 3 - Viral decay, immunological results, and eGFR average trend for 48 weeks in the Rainbow Study (modified from Camici M, et al. 24th International AIDS Conference - AIDS 2022; Abst.#EPB151).
The Rainbow study is the first ART rapid treatment clinical trial focused on an advanced HIV population in a real-world clinical setting. The results support the efficacy, safety, and feasibility of a rapid start strategy with B/F/TAF in patients with advanced HIV. Moreover, 30/40 of the patients diagnosed with advanced HIV infection met the eligibility criteria and were enrolled in the study, and this observation supports the feasibility of the rapid ART strategy even in such a challenging scenario. It was notework that, the study was performed during the COVID-19 pandemic, when hospitals were significantly overburdened and health services were extensively involved in the management of COVID-19. Efficacy analysis showed high effectiveness of rapid ART with B/F/TAF with rapid viral decay and 90% viral efficacy at week 48. When using a rapid initiation strategy, information on transmitted HIV resistance, renal function, and HBV co-infection may not be available before therapy starting. Given the safe renal profile, high potency and genetic barrier, and activity against HBV, B/F/TAF could be considered an attractive option in a rapid onset strategy setting.
The LAPTOP Study
The main aim of the LAPTOP study is to compare two different types of antiretroviral treatment, in terms of efficacy and improvement in side effects, for patients diagnosed with advanced HIV infection. This is the first large randomized controlled trial comparing treatments for patients in this situation. The two different types of treatment are the enhanced protease inhibitor (PI) combination, in the form of combination tablets containing darunavir, cobicistat, emtricitabine, and tenofovir alafenamide, and the integrase inhibitor (INI) combination containing bictegravir, emtricitabine, and tenofovir alafenamide. Both drug combinations have been approved for use in Europe. To compare the two treatments, half of the participants in the LAPTOP study will receive the PI treatment and the other half the INI treatment. A total of 440 participants will be recruited from sites across Europe and randomized in an open-label design to one of the two arms of the study. After randomization to one of the two treatment regimens, patients will participate in approximately 9 follow-up visits over the course of one year. They will be asked to provide blood samples, to ensure viral efficacy and eventually selected drug-resistance mutations during treatment. During the study, patients will be also asked to complete questionnaires to assess their quality of life and HIV symptoms. The LAPTOP Study is currently still ongoing and the results were not yet available.
CONCLUSIONS
Although there is still limited evidence on the use of specific antiretroviral regimens in HIV late presenter or advanced disease patients, the B/F/TAF-containing combination has been tested in observational or uncontrolled pilot studies, while a large randomized controlled trial is currently ongoing. The characteristics of high potency, high genetic barrier, high safety, and low level of pharmacological interactions make this combination an ideal profile for the initiation of antiretroviral therapy in the HIV late presenter or advanced HIV disease patient, even in the context of rapid start or same-day treatment regimens, where the initiation of treatment usually occurs in the absence of information on viral load, CD4 count, biochemical profile and HIV transmitted resistance.
Funding
None.
Conflict of interest
None to declare.
REFERENCES
[1] Mussini C, Manzardo C, Johnson M, et al. Late Presenter Investigators. Patients presenting with AIDS in the HAART era: a collaborative cohort analysis. AIDS. 2008 Nov 30; 22 (18), 2461-9. doi: 10.1097/QAD.0b013e328314 b5f1.
[2] Late presenters working group in COHERE in EuroCoord; Mocroft A, Lundgren J, Antinori A, et al. Late presentation for HIV care across Europe: update from the Collaboration of Observational HIV Epidemiological Research Europe (COHERE) study, 2010 to 2013. Euro Surveill. 2015; 20 (47). doi: 10.2807/1560-7917.ES.2015.20.47.30070.
[3] Montlahuc C, Guiguet M, Abgrall S, et al. French Hospital Database ANRS CO4 cohort. Impact of late presentation on the risk of death among HIV-infected people in France (2003-2009). J Acquir Immune Defic Syndr. 2013 Oct 1; 64 (2), 197-203. doi: 10.1097/QAI.0b013e31829cfbfa.
[4] Antinori A, Coenen T, Costagliola D, et al. European Late Presenter Consensus Working Group. Late presentation of HIV infection: a consensus definition. HIV Med. 2011 ; 12 (1): 61-64. doi: 10.1111/j.1468-1293.2010.00857.x. [5] Zolopa A, Andersen J, Powderly W, et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial. PLoS One. 2009; 4 (5), e5575. doi: 10.1371/journal.pone.0005575.
[6] Mounzer K, Brunet L, Fusco J, et al. Advanced HIV infection in the US: immune response to ART initiation. 24th International AIDS Conference - AIDS 2022; Abst.#EPB148.
[7] Camici M, Gagliardini R, Lanini S, et al. A pilot study of the impact of a rapid ART initiation in advanced HIV disease. 24th International AIDS Conference - AIDS 2022; Abst.#EPB151.
[8] Neat ID Foundation: The Late Presenter Treatment Optimisation Study (LAPTOP). ClinicalTrials.gov Identifier: NCT03696160; https://clinicaltrials.gov/ct2/show/NCT03696160.