Le Infezioni in Medicina, n. 3, 421-424, 2023
doi: 10.53854/liim-3103-18
LETTERS TO THE EDITOR
Chagas disease in Italy: an update of epidemiological studies
Spinello Antinori1,2, Andrea Giacomelli2, Federico Sabaini1,2, Giacomo Casalini1,2, Anna Lisa Ridolfo2
1Department of Biomedical and Clinical Sciences, Università degli Studi di Milano, Italy;
2III Division of Infectious Diseases, ASST Fatebenefratelli Sacco, Luigi Sacco Hospital, Milan, Italy
Article received 26 June 2023, accepted 11 July 2023
Corresponding author
Spinello Antinori
E-mail: spinello.antinori@unimi.it
Dear Editor,
We read with interest the paper by Raglio et al. reporting their seven-years’experience regarding Chagas disease (CD) screening among Bolivian migrants in Bergamo province [1]. Overall, they showed a 19% prevalence for CD serology (210/1105) with 11.7% prevalence among pregnant women (60/512). In their experience only one newborn had a confirmed congenital Chagas disease and this case has been previously published as a single case report and as a part of a study demonstrating a 4.3% rate of vertical transmission of Trypanosoma cruzi [2, 3]. These figures are in agreement with a systematic review and meta-analysis conducted by Colombo et al. on Latin American (LA) pregnant women living outside endemic areas [4]. They found a 4.2% pooled prevalence of T. cruzi infection among LA pregnant women with a 15.5% pooled prevalence in pregnant women from Bolivia and a global rate of congenital transmission of 3.5% [4].
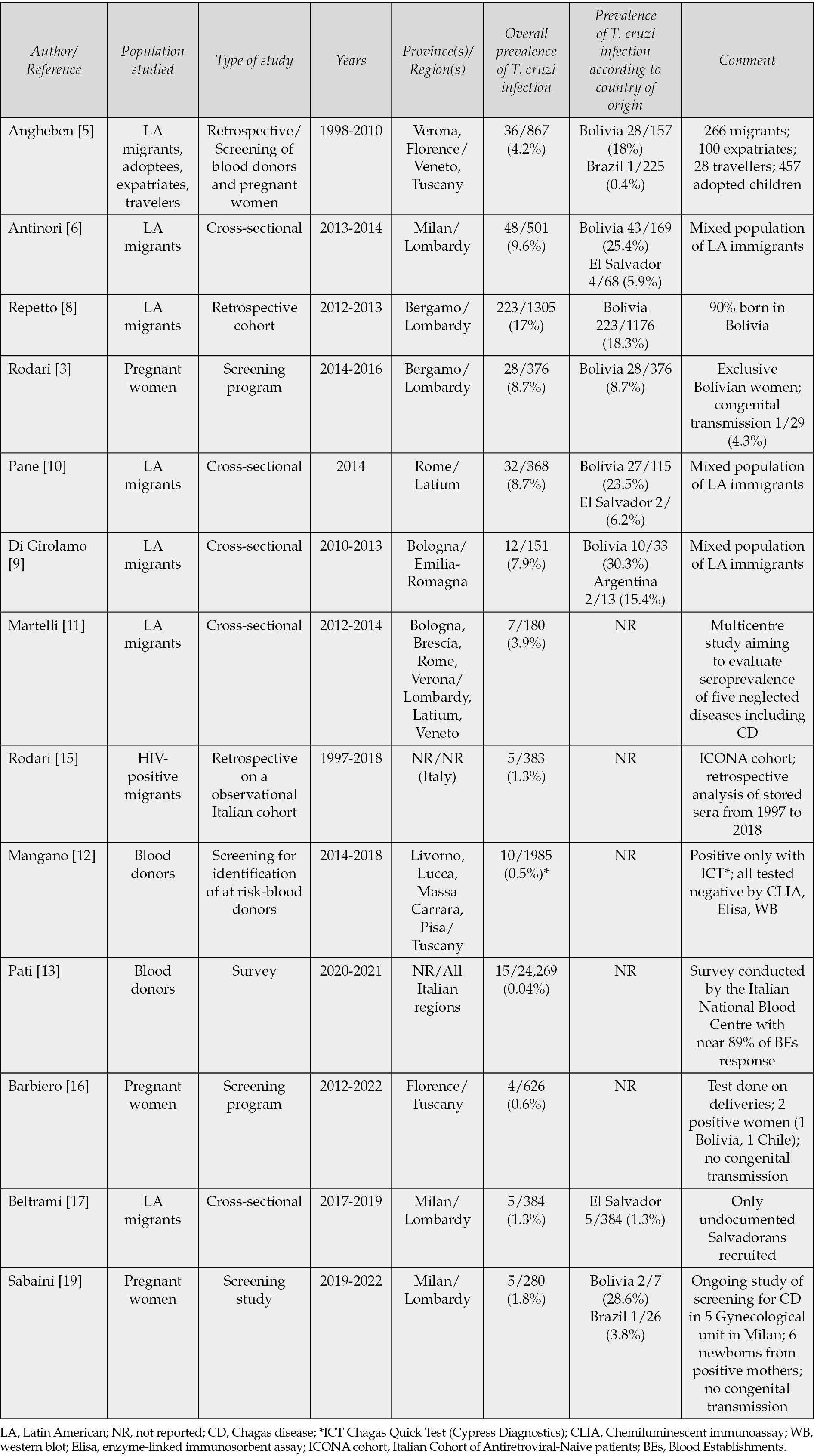
However, Raglio et al. citing a study by Angheben et al. state that “it was confirmed that among Bolivians immigrants 30.7% had a positive serological results, which is in accordance with other published studies but in contrast with to Antinori et al., that showed a lower prevalence of positive results” [5, 6]. At variance with their statement, the prevalence of CD reported by Angheben among Bolivian migrants was 18% and in our study 25.4% [4,6]. As shown in table 1 [3, 5, 7-13, 15-19], the three-four fold higher prevalence reported in different studies conducted so far in Italy among Bolivian immigrants in comparison with the country seroprevalence estimates (6.1%) by World Health Organization are probably the consequence of the phenomenon of cluster immigration from areas with the highest seroprevalence (for instance Santa Cruz, Cochabamba) [14]. However, it should be highlighted that not only Bolivians, who are certainly those at highest risk of having acquired CD in their country of origin, but also other population of LA immigrants should be targeted for serological screening as demonstrated by Beltrami et al., in their recent study involving Salvadoran people [17]. In non-endemic countries such as Italy, autochthonous cases of CD can occur by vertical transmission from mother to child, by transfusion with blood and blood products and through the transplant of solid organs or hematopoietic stem cells. As far as the mother-to child transmission, following the first case described in Bergamo, a cluster of congenitally infected children has been identified in Milan among Bolivian immigrants [2, 18]. Except for the Tuscany Region where serogical screening for CD is included among the free laboratory investigations that can be performed during pregnancy according to a Regional resolution [16] we are aware of this chance only available in Bergamo and in Milan as a part of an ongoing study [19]. In Italy blood donation by at risk candidate donors (i.e., people born in Latin America or from Latin American mothers and travellers with a history of rural or outdoors activities in endemic countries) is regulated by the Italian transfusion regulation (L.219, D.M. 02/11/2015) [20]. Two studies so far addressed this issue : the first one conducted in Tuscany evaluated the use of an immunochromatographic test (ICT) as a screening on donated blood and the second one was a survey conducted by the Italian National Blood Centre (INBC) to gather information on the management of donors at risk of CD in the national Blood Establishments (BEs) [12, 13]. The study by Mangano et al., provided evidence of the lack of sensitivity and specificity of ICT as a screening test for blood donors at risk of CD [12]. The INBC survey involving a representative sample of BEs during the years 2020 and 2021showed a low rate of confirmed positive blood donation: 0.06% in 2020 (66/100,000 donors tested) and 0.05% in 2021 (55/100,000 donors tested) [13]. A last point that should be considered is the risk of reactivation of CD among people living with HIV (PLWH) or those undergoing immunosuppression for transplantation [21]. To the best of our knowledge only one retrospective study performed on LA HIV-infected migrants enrolled in the Italian Cohort of Antiretroviral Naive (ICONA) patients have been done in Italy [15]. The study showed a 1.3% prevalence of subjects with confirmed positive serology for T. cruzi with an high rate of discordant results (3.34%). In conclusion, CD is an emerging neglected disease in Italy [22] and further studies are needed to better characterise this issue with important implications of public health.
Table 1 - Studies conducted in Italy on Chagas disease prevalence in different setting and populations
Conflict of interest
None to declare.
Funding sources
None to declare
REFERENCES
[1] Raglio A, Clemente L, Guarneri D, et al. Prevention of congenital Chagas disease by screening of mothers and monitoring of serological tests of neonates: the seven years’experience. Infez Med. 2023; 2, 243-249.
[2] Bargiggia G, Ruggeri M, Ortalli G, et al. Congenital Chagas disease in a Bolivian newborn in Bergamo (Italy). Infez Med. 2018; 2, 93-96.
[3] Rodari P, Angheben A, Gennari G, et al. Congenital Chagas disease in a non-endemic area: results from a control programme in Bergamo Province Northern Italy. Travel Med Infect Dis. 2018;25, 31-34.
[4] Colombo V, Giacomelli A, Casazza G, et al. Trypanosoma cruzi infection in Latin American pregnant women living outside endemic countries and frequency of congenital transmission: a systematic review and meta-analysis. J Travel Med 2021, 28(1), taa170, 1-9.
[5] Angheben A, Anselmi M, Gobbi F, et al. Chagas disease in Italy: breaking an epidemiological silence. Euro Surveill. 2011; 16(37), pii=19969.
[6] Antinori S, Ridolfo AL, Giacomelli A, et al. Chagas disease in Italy: the study’s contribution of Italian researchers. Panminerva Med. 2019;61(4), 464-472.
[7] Antinori S, Galimberti L, Grande R, et al. Chagas disease knocks on our door: a cross-sectional study among Latin American immigrants in Milan, Italy. Clin Microbiol Infect. 2018; 24, 1340.e1-1340.e6.
[8] Repetto EC, Zachariah R, Kumar A, et al. Neglect of a neglected disease in Italy: the challenge of access-to-care for Chagas disease in Bergamo. Plos Negl Trop Dis. 2015; 9(9), e0004103.
[9] Di Girolamo C, Martelli G, Ciannameo A, et al. Chagas disease in a non-endemic country: a multidisciplinary research, Bologna, Italy. J Immigrant Minority Health. 2016;18, 616-623.
[10] Pane S, Giancola ML, Piselli PL, et al. Serological evaluation for Chagas disease in migrants from Latin American countries resident in Rome, Italy. BMC Infect Dis. 2018; 18, 212.
[11] Martelli G, Di Girolamo C, Zammarchi L, et al. Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: a cross-sectional study. Clin Microbiol Infect. 2017;23, 335.e1-335.e5.
[12] Mangano VD, Prato M, Marvelli A, Moscato G, Bruschi F. Screening of at-risk blood donors for Chagas disease in non-endemic countries: lessons from a 2-year experience in Tuscany, Italy. Transfusion Med. 2021; 31, 63-68.
[13] Pati I, Cruciani M, Masiello F, et al. Chagas disease and transfusion risk in Italy: the results of a National survey. Pathogens. 2022; 11,1229.
[14] WHO. Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidem Rec. 2015;90, 33-44.
[15] Rodari P, Tamarozzi F, Tais S, et al. Prevalence of Chagas disease and strongyloidiasis among HIV-infected Latin American immigrants in Italy- The CHILI study. Travel Med Infect Dis. 2022;48, 102324.
[16] Barbiero A, Mazzi M, Mantella A, et al. A questionnaire integrated with digital medical record improved the coverage of a control program for congenital Chagas disease in Tuscany, Italy. Microorganims. 2023;11(1), 154.
[17] Beltrami M, Grande R, Giacomelli A, et al. Chagas disease prevalence among migrants from El Salvador in Milan: a cross-sectional study of an often-overlooked population. Infect Dis. 2023 June 15; 1-8. doi: 10.1080/23744235.2023.2222817. 55 (8), 559-566. Online ahead of print.
[18] Antinori S, Galimberti L, Grande R, et al. Family cluster of Chagas disease among Bolivian immigrants in Italy: high rate of maternal-fetal transmission. Travel Med Infect Dis. 2022; 49, 102370.
[19] Sabaini F, Giacomelli A, Ierardi M, et al. Trypanosoma cruzi infection in Latin American pregnant women living in Milan, Italy: a cross-sectional study. 33rd ECCMID, Copenhagen, Denmark 15-18 April 2023.
[20] Decreto del Ministero della Salute 2 Novembre 2015. Disposizioni relative ai requisiti di qualità e sicurezza del sangue e degli emocomponenti. Gazzetta Ufficiale n.300- Suppl. Ordinario n.69, 28 Dicembre 2015. Available: https://www.gazzettaufficiale.it/eli/id/2015/12/2815A09709/sg
[21] Clark EH, Bern C. Chagas disease in people with HIV: a narrative review. Trop Med Infect Dis. 2021;6(4), 198.
[22] Guerri-Guttemberg RA, Ciannameo A, Di Girolamo C, Milei JJ. Chagas disease: an emerging public health problem in Italy? Infez Med 2018; 17(1), 5-13.