Le Infezioni in Medicina, n. 3, 384-393, 2023
doi: 10.53854/liim-3103-12
CASE SERIES
Multifaceted realities of scrub typhus: a case series from southern India
Diviya Bharathi Ravikumar1, Barath Prashanth Sivasubramanian2, Sruthi Nandhaa Shanmugam3, Vanitha Krishnaswamy4, Ali Rabaan5,6,7, Jaffar A. Al-Tawfig8,9,10, Raghavendra Tirupathi11
1Department of Internal Medicine, ESIC Medical College and PGIMSR, Chennai, India;
2Department of Infectious Diseases, University of Texas Health Science Centre, San Antonio, USA;
3Department of Internal Medicine, Kasturba medical college, Mangalore, India;
4Department of Pediatrics, KAPV Government Medical College, Trichy, India;
5Molecular Diagnostic Laboratory, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia;
6College of Medicine, Alfaisal University, Riyadh, Saudi Arabia;
7Department of Public Health and Nutrition, The University of Haripur, Haripur, Pakistan;
8Specialty Internal Medicine and Quality Department, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia;
9Infectious Diseases Division, Department of Medicine, Indiana University School of Medicine, Indianapolis, USA;
10Infectious Diseases Division, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, USA;
11Cure Drug Repurposing Collaboratory
Article received 11 June 2023, accepted 31 July 2023
Corresponding author
Barath Prashanth Sivasubramanian
Email: barathprashanth18196@gmail.com
SummaRY
Scrub typhus is an acute febrile illness caused by Orientia tsutsugamushi, a Gram-negative bacillus, commonly occurring in the Asia-Pacific region. It is transmitted to humans by the bite of an infected Leptotrombidium mite and the bacterium causes endothelial dysfunction resulting in widespread vasculitis and the possible development of thrombocytopenia, meningitis, acute respiratory distress syndrome, and infrequently, myocarditis. Early diagnosis and prompt treatment are crucial in managing scrub typhus. Here, we present four cases of scrub typhus with a comprehensive literature review. This study highlights the significance of considering scrub typhus as a possible diagnosis in patients of all ages from endemic regions who exhibit symptoms such as fever, thrombocytopenia, or transaminitis, even in the absence of typical clinical features. Two cases exhibited the characteristic lesion of eschar at the site of mite feeding. One case involved a middle-aged woman who was diagnosed with typhus-induced myocarditis with left ventricular dysfunction. Another case involved a 23-day-old neonate with poor feeding and seizures, who was diagnosed with late-onset sepsis with meningitis. Scrub typhus was confirmed in all cases using a positive qualitative IgM ELISA. However, it is preferred to use paired (ELISA before and after antibiotic therapy) or quantitative titers for confirmation. Healthcare providers must consider the patient’s exposure history and clinical presentation to diagnose and treat scrub typhus promptly.
Keywords: Myocarditis, scrub typhus, meningitis, eschar, mite bites.
INTRODUCTION
Scrub typhus, caused by Orientia tsutsugamushi (formerly Rickettsia tsutsugamushi discovered in 1930), is a bacterial infection transmitted to humans through the bite of an infected mite of the genus Leptotrombidium, commonly known as chiggers. Chiggers serve as the bacterium’s reservoir, and the infection is mostly prevalent in South and East Asia and parts of the Pacific Rim [1, 2]. The two major categories of vertebrates that carry chiggers are the “maintaining hosts,” including rodents, shrews, and ground-dwelling birds, and the “incidental hosts,” which include other birds and larger mammals such as humans [3]. In Asia, the seasonality of human scrub typhus has been well documented. Japan, South Korea, Taiwan, and northern parts of China report the infection almost exclusively occurring from spring until early winter. Thailand, Burma, and India have found the disease to be most prevalent from June to November but may occur year-round [4].
Scrub typhus has been on the rise recently, with an estimated 1 million cases occurring annually [5]. Hospitalization is required for about a third of cases due to the involvement of multiple organs and is associated with high fatality rates [6]. According to a study conducted in India, 24.4% of patients with unexplained fever with or without multi-system involvement were found to have scrub typhus, and 53.1% of those with scrub typhus had acute kidney injury [7]. Scrub typhus, if left untreated, has a mortality rate of around 6%, rising to 13% when appropriate antibiotics are not used. Complications can lead to higher mortality rates, with 14% in case of central nervous system infection and 20% in case of multiple organ [8]. The most common complications include hepatitis (40.5%), thrombocytopenia (28.4%), acute respiratory distress syndrome (ARDS) (20.5%), acute kidney injury (19.2%), meningitis (16.4%), shock (16.2%), and myocarditis (15.5%) [6]. Thus, in this study, we present four cases to illustrate the varying presentations and complications of scrub typhus.
Case Presentation - 1
A 45-year-old woman from South India presented to a primary care facility with a two-day history of intermittent fever, headache, severe vomiting, lower abdominal pain, and loss of appetite. On room air, her SpO2 was 98%, body temperature was 39°C, blood pressure was 120/80 mm Hg, pulse rate was 101 beats per minute, and respiratory rate was 20 breaths per minute. The patient’s qSOFA score was 0, indicating she was not at high risk of sepsis. The patient had mild anemia (hemoglobin 11.2 g/dl), neutrophilic leukocytosis (WBC - 11,430/mm3), elevated liver enzymes (AST - 129 U/L, ALT - 70 U/L), and ongoing inflammation (CRP levels of 3.5 mg/dL).
The chest radiograph showed no abnormalities, while ECG indicated sinus tachycardia. Testing revealed negative for dengue, malaria, and typhoid. In view of her symptoms and neutrophilic leukocytosis, a bacterial etiology was presumed, and was started on intravenous ceftriaxone. Her condition did not improve and was transferred to the tertiary care facility on the fourth day of illness. Patient had temperature of 39 degrees C, 108 beats per minute, her saturation was well maintained, and respiratory rate was 17 breaths per minute. On further probing, the patient revealed a history of insect bite on her back. On examination, 2 x 1 cm eschar with surrounding inflammation was found on the right suprascapular area (Figure 1).
Table 1 - Laboratory values at the time of admission.
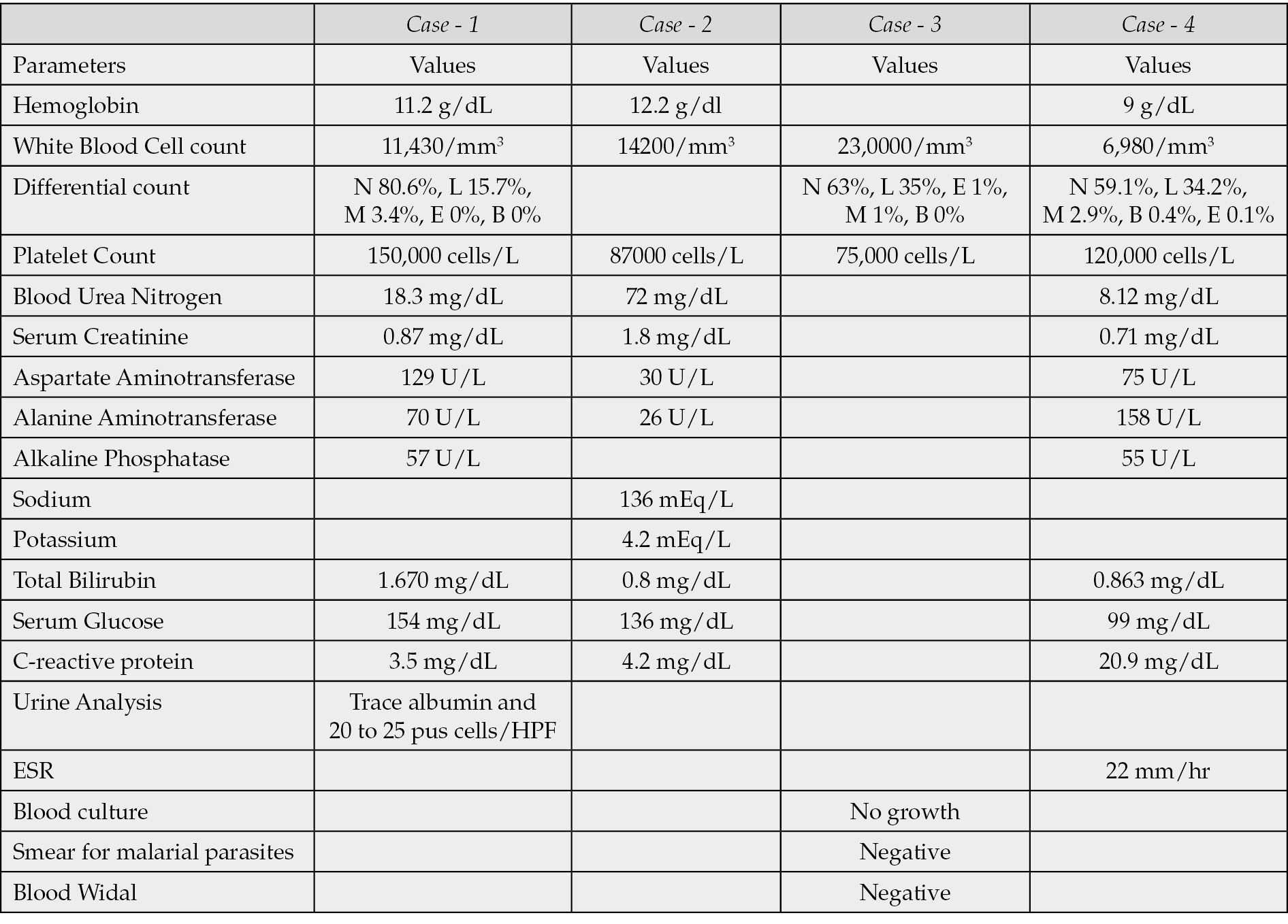

Figure 1 - An eschar with surrounding inflammation on the right suprascapular area
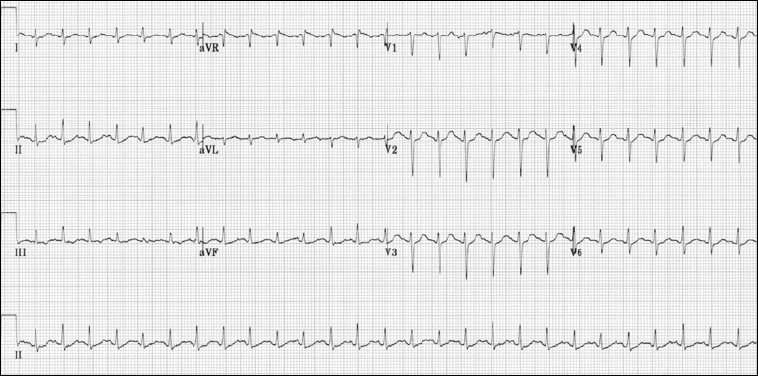
Figure 2 - EKG of Myocarditis
ELISA yielded positive results for IgM scrub typhus and negative results for IgG scrub typhus and leptospirosis. PCR testing for COVID-19 was also negative. Due to the patient’s prolonged fever and decreasing platelet count, an ultrasound of the abdomen was performed, which revealed mild splenomegaly measuring 12.3 cm and grade 1 fatty liver.
After the diagnosis of scrub typhus was confirmed, the patient met the criteria for systemic inflammatory response syndrome (SIRS) (heart rate of 108 beats per minute, temperature of 39°C). She was admitted to the general medical ward, ceftriaxone was discontinued, and intravenous doxycycline was added. As the patient met the criteria for SIRS, intravenous route was chosen. Two days after starting antibiotics, the patient’s fever subsided, and was changed to oral doxycycline 100 mg twice daily for five days. The patient was given analgesics and antiemetics to alleviate the symptoms, and she was discharged following symptomatic improvement.
Case Presentation - 2
A 45-year-old female presented to the emergency department with a five-day history of fever associated with vomiting and breathlessness for three days. She also complained of orthopnea and had an eschar on her lower abdomen that was noticed a week ago.
On examination, the patient was conscious and cooperative. Her blood pressure was 130/90 mm Hg, pulse was 120/min, and her oxygen saturation was 93% with nasal oxygen at 4 liters/min. Basal crepitations were noted over the lung fields. An eschar was present on her right lower quadrant of the abdomen. She had pitting pedal edema on both legs. Jugular vein was not distended.
Further investigations revealed a decreased platelet count and elevated blood urea nitrogen and creatinine on admission. An ultrasound of the kidneys revealed increased cortical echoes bilaterally, indicating inflammation. An IgM ELISA for scrub typhus was positive. Her chest x-ray, liver function tests, and electrolyte levels were within normal limits. The patient had non-specific ST and T wave changes in V2 to V5 in EKG.
An ECHO showed global hypokinesia of the left ventricle, grade 3 left ventricular diastolic dysfunction, severe left ventricular systolic dysfunction, and an ejection fraction of 30 percent. Right ventricular dysfunction was also noted. No associated valvular conditions were present. Table 2 shows the Echocardiography findings found before and after treatment and figure 3 show the Echocardiography image.
A diagnosis of Scrub typhus causing myocarditis was made. The patient was treated with Doxycycline 100 mg iv twice daily and Dexamethasone 4 mg iv twice daily, and analgesics. Following treatment, the patient’s condition significantly improved within a week, and the steroids were tapered off. A repeat ECHO performed after her recovery showed no regional wall motion abnormalities, Grade 1 LVDD, no right ventricular dysfunction, and an ejection fraction of 64%.
Table 2 - Echocardiography findings - Before and After treatment.
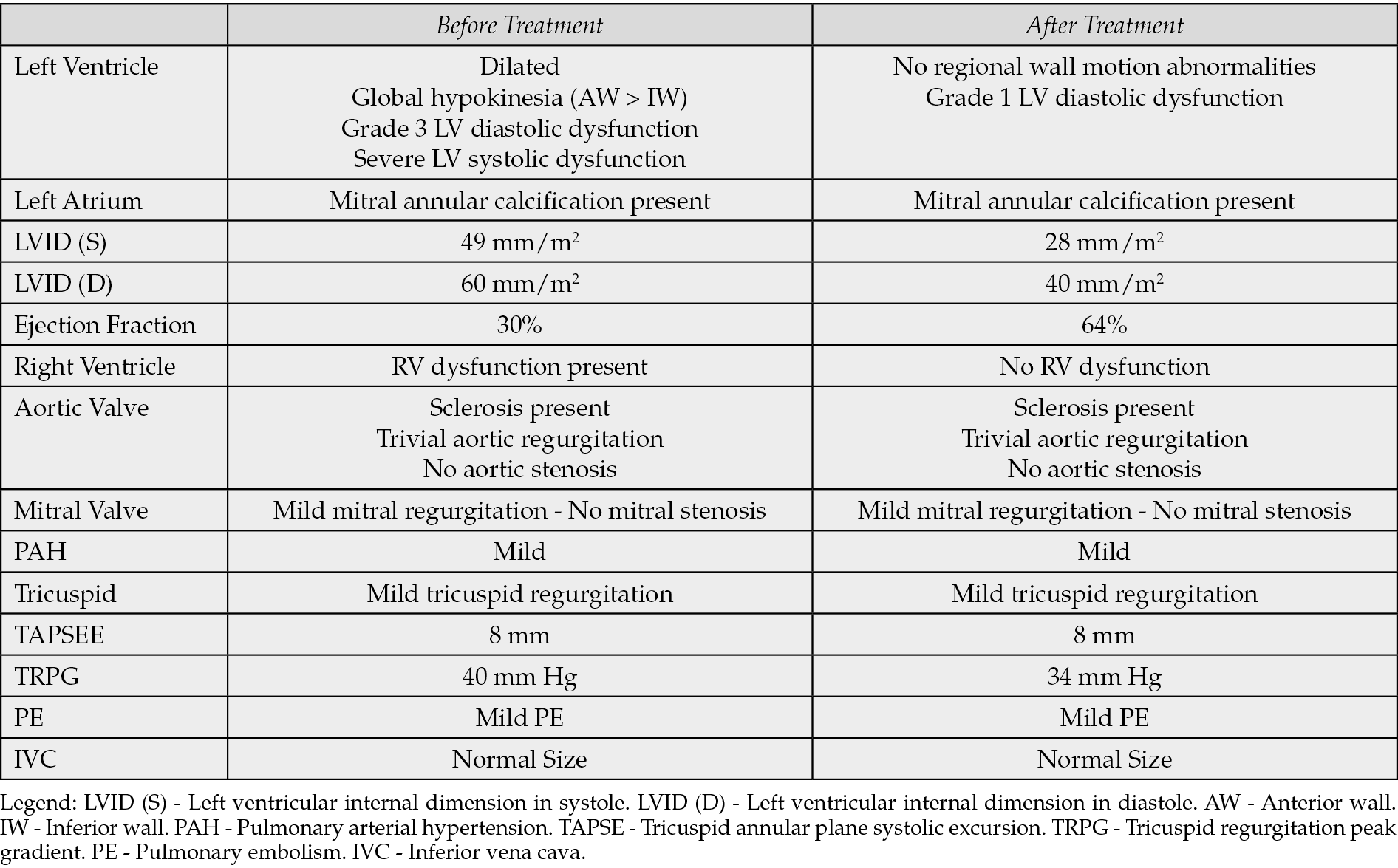
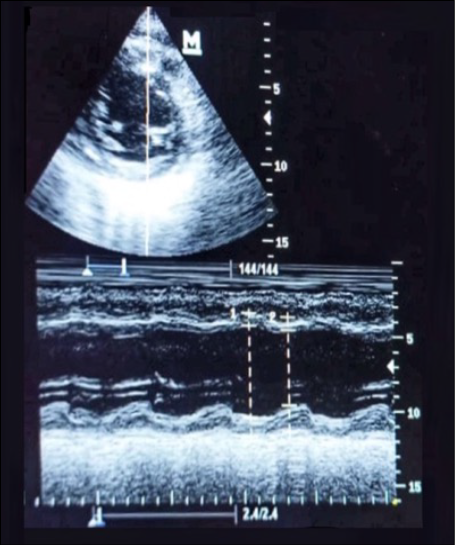
Figure 3 - Echocardiography findings.
Case presentation - 3
A 23-day-old neonate presented with poor feeding, lethargy, and fever for three days and a history of clonic seizures on the third day. On examination, the child was febrile, irritable, and had hepatosplenomegaly with ongoing seizure activity. No pallor, icterus, edema, eschars, or purpura were observed. Vital signs included a heart rate of 148/min, respiratory rate of 46/min, and temperature of 37°C. The abdomen was distended with hepatosplenomegaly. Lab tests revealed leukocytosis and thrombocytopenia with a third spacing of fluid evident on chest x-ray and ultrasound. The qualitative CRP was positive, and the ELISA IgM scrub test was positive. A lumbar puncture showed neutrophilic predominance, leading to a diagnosis of late-onset sepsis with meningitis due to bacteremia.
Treatment involving antiepileptics and intravenous doxycycline was given for seven days. The baby responded well to treatment with no recurrence of seizures after the second day. Symptoms subsided by the third day and the neonate regained normal activity by the fourth day. Patient was discharged successfully on the seventh day after completion of the course.
Table 3 - CSF studies.
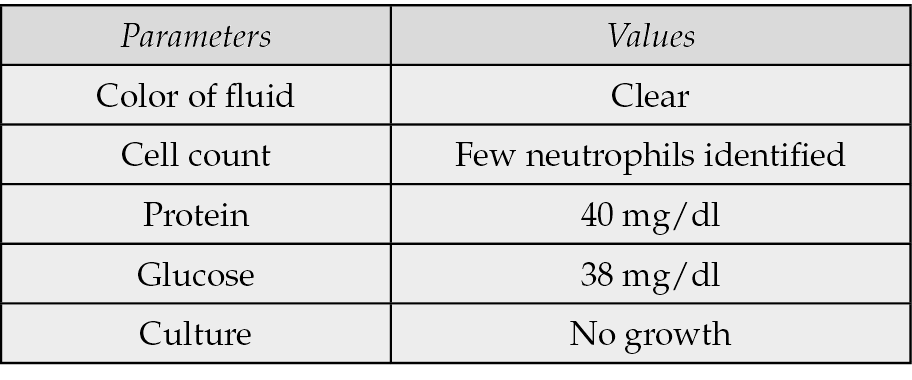
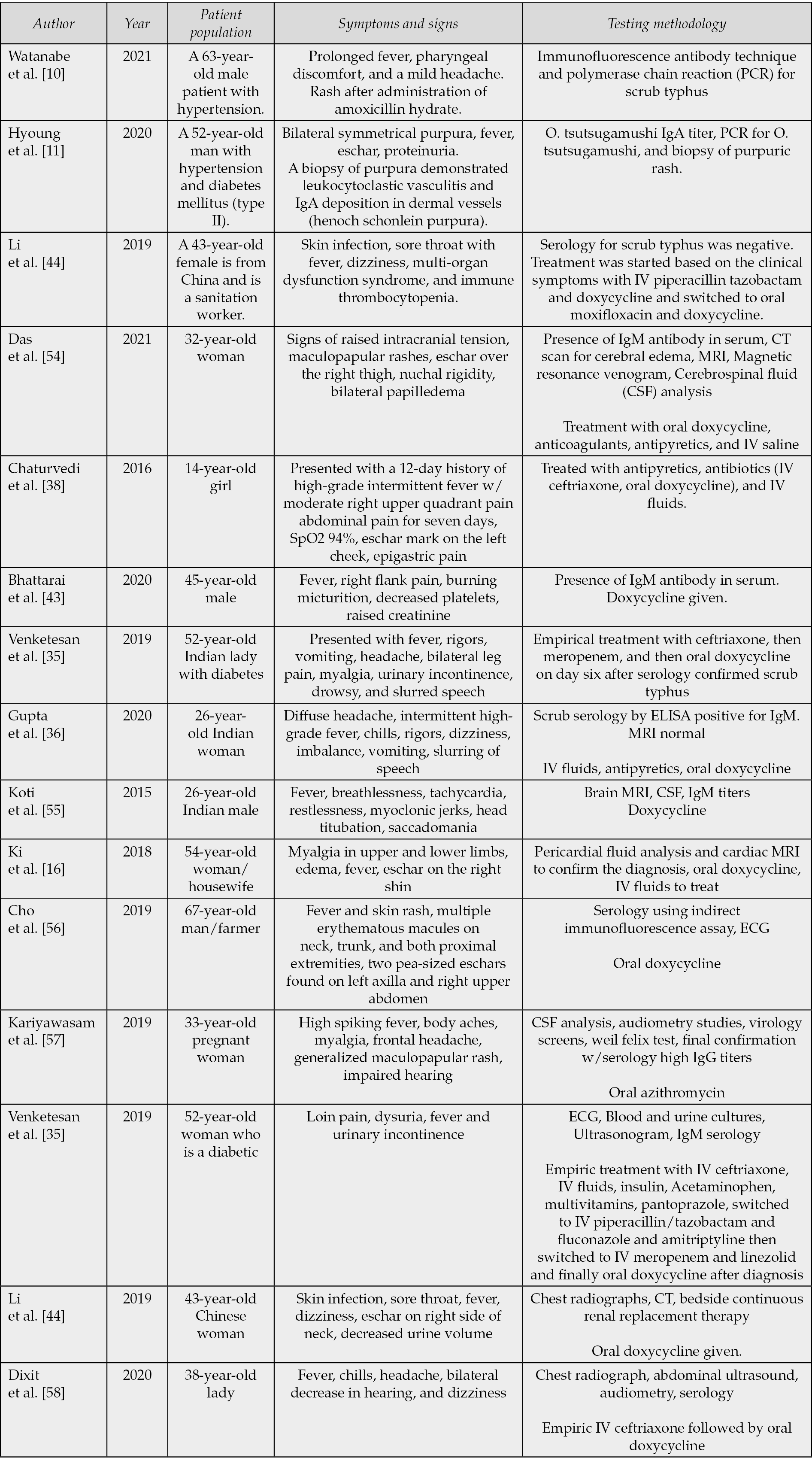
Table 4 - Literature review on Atypical Presentations of Scrub Typhus.
Case Presentation - 4
A 38-year-old woman from South India presented to the emergency department with a four-day history of intermittent fever, body pain, headache, multiple episodes of vomiting, and abdominal pain. No eschar was found in the scalp, face, mucous membranes, wrists, ankles, palms, and soles. On room air, her SpO2 was 98%, body temperature was 99.6°F, blood pressure was 110/70 mm Hg, pulse rate was 98 beats per minute, and respiratory rate was 18 breaths per minute. The patient’s qSOFA score was 0, indicating she was not at high risk of sepsis. On admission, the lab values indicate anemia (hemoglobin-9 g/dl), active inflammation (CRP - 20.9, ESR - 22 mm/hr), platelet count was 120,000/L, and occult stool blood was positive. The chest radiograph was normal. ECG showed a sinus rhythm of 75 beats/min. ELISA assay was positive for IgM Scrub typhus. The patient’s prolonged fever with abdominal pain prompted an abdomen ultrasound, which revealed mild splenomegaly of 13.2 cm and a right ovarian follicular cyst. After the diagnosis of scrub typhus, the patient was admitted and was started on intravenous doxycycline twice daily for two days. Due to repeated episodes of vomiting, an intravenous route was preferred. Following improvement of symptoms, oral doxycycline was given twice daily for five days. The fever subsided on the 6th day and the patient became asymptomatic.
Discussion
In the cases described, the patients presented with fever and other symptoms, including vomiting, headache, abdominal pain, breathlessness, poor feeding, lethargy, and seizures. The patients had various clinical syndromes associated with Scrub typhus infections. Investigations involved ELISA for scrub typhus, chest X-ray, ultrasound, and ECHO. Treatment involved doxycycline and supportive therapy for symptom relief. The patients responded well and showed clinical improvement. Scrub typhus can have varying clinical presentations, from mild to severe, including organ failure and death. Symptoms can begin insidiously or abruptly, including fever, intense headache, diffuse myalgias, and a possible rash or eschar. In patients with scrub typhus, the frequency of eschars is highly variable. In one report, 46% of patients in South Vietnam developed eschars [9]. The development of vasculitis and lymphocytic infiltration of blood vessels in scrub typhus may result in atypical clinical manifestations. Rashes similar to infectious mononucleosis and Henoch schonlein purpura have been reported [10, 11].
According to a study by Varghese et al., the occurrence of cardiovascular complications was seen in 42% and neurologic manifestations in 20% of patients with scrub typhus [12]. Myocarditis, in particular, is rare (1.6%) among scrub typhus patients [13]. These patients are usually elderly individuals (OR=1.04, 95%CI: 0.99-1.09) and had longer hospital stays (OR=1.17, 95% CI: 0.98-1.40) [14]. An elevated total bilirubin level, the incidence of ST elevations on EKG, and paroxysmal atrial fibrillation are more common in those with acute myocarditis than those without [15]. Myocarditis has presented along with rhabdomyolysis [16] and scrub typhus can also cause pericarditis [17] and fulminant perimyocariditis [18]. With regards to ECG changes, abnormalities were identified both in the febrile and convalescent stages of the illness [19]. Studies reported that clinical examination findings at presentation cannot truly reflect on the hemodynamic changes of the patient and ECG is required in scrub typhus [20, 21]. Second-degree heart blocks, relative bradycardia, prolonged QT interval, atrial fibrillation, and ischemic changes have been noted [20, 22-24]. New onset atrial fibrillation is rare (incidence of 1%) and commonly seen in elderly males who have an underlying cardiovascular disease [25, 26]. The ischemic changes in scrub typhus (incidence of 15.1%) are due to bacteria-induced vasculitis and present with no evidence in coronary angiography [23, 27]. Biomarkers such as cardiac troponin, CK-MB, and Brain natriuretic peptide are found to be elevated, and reduced EF is detected [28]. Chest radiography findings have also shown significant associations in patients with cardiovascular dysfunction and must be performed routinely [29].
When encountering any acute febrile illness presenting with an acute onset neurological disorder in the tropics or subtropics, scrub typhus infection should be considered as one of the differentials [30]. Scrub-induced vasculitis, direct bacterial invasion into the CSF, and type 2 hypersensitivity reaction targeting self-antigens are the most common mechanisms by which CNS manifestations occur [31]. A clinically detectable neurological involvement is seen in 20% of patients, seizures in 6.3–21.6% [32], and meningoencephalitis in 12.4% [33]. In India, 25% of acute encephalitic syndromes are due to scrub typhus [32]. Rarely, scrub typhus can cause cerebral venous thrombosis [34], sudden bilateral sensorineural hearing loss [35], cerebrellitis [36], and Guillain barre syndrome [37]. Organ involvement presenting as lobar pneumonia [38], ARDS [39], liver dysfunction [40], pancreatitis [41], acute kidney injury [42], and pyelonephritis [35, 43] have occurred. Furthermore, atypical presentations such as rhabdomyolysis [16], immune thrombocytopenia with multi-organ dysfunction [44], disseminated intravascular coagulation [45], and even hemophagocytic syndrome [46] have been noted.
A conclusive diagnosis of acute scrub typhus infection is obtained using the immunofluorescent antibody (IFA) assay. In situations where there is a lack of trained personnel and fluorescent microscopes, the use of recombinant 56KDa TSA in Scrub typhus IgM ELISA could be a viable alternative to IFA [47]. According to Coleman et al, the utilization of r56KDa TSA in IgM ELISA resulted in a sensitivity and specificity of 93.0% and 94.0%, respectively [48]. In a separate study conducted in India, the sensitivity and specificity of IgM ELISA were reported as 86.5% and 97.5%, respectively [49]. Antibiotics like doxycycline, rifampicin, and azithromycin are commonly used to treat scrub typhus patients, with doxycycline being the drug of choice. Treatment usually involves administering doxycycline at 100mg twice daily for 7-15 days or chloramphenicol 500 mg four times daily orally for 7-15 days [26]. Azithromycin may also be an alternative, especially for pregnant women, 500mg orally for three days [50]. According to a study by Varghese et al., a 7-day intravenous course of doxycycline and azithromycin was superior to either treatment alone in terms of death on the 28th day, persistent complications on the 7th day, or persistent fever on the 5th day (33% vs 47%). The time until PCR negativity was also shorter in the combination group [12]. A study in South India showed the case fatality rate of the disease to be as high as 12.2% [52]. The disease’s mortality is attributable to late presentation, delayed diagnosis, and drug resistance [53]. A high index of suspicion and a detailed history, including recent travel and the presence of rash, help establish the diagnosis and reduce mortalities [36, 51].
Conclusion
In conclusion, Scrub typhus, a disease transmitted through mites, requires a high index of suspicion in endemic areas. Serology using paired quantitative titers is an advised method for diagnosis. Early identification and prompt initiation of antibiotics can significantly reduce the risk of complications associated with this disease. Therefore, healthcare providers and public health officials in endemic regions must prioritize increasing awareness and implementing effective diagnostic and treatment strategies to reduce the morbidity and mortality associated with Scrub typhus.
References
[1] El Sayed I, Liu Q, Wee I, et al. Antibiotics for treating scrub typhus. Cochrane Database Syst Rev. 2018; 9: CD002150.
[2] Xu G, Walker DH, Jupiter D, et al. A review of the global epidemiology of scrub typhus. PLoS Negl Trop Dis. 2017; 11, e0006062.
[3] Traub R, Wisseman CL Jr. The ecology of chigger-borne rickettsiosis (scrub typhus). J Med Entomol. 1974; 11, 237-303.
[4] Elliott I, Pearson I, Dahal P, et al. Scrub typhus ecology: a systematic review of Orientia in vectors and hosts. Parasit Vectors. 2019; 12, 513.
[5] Lu D, Wang T, Luo Z, et al. Evaluation of the Therapeutic effect of antibiotics on scrub typhus: a systematic review and network meta-analysis. Front Public Health. 2022; 10, 883945.
[6] Devasagayam E, Dayanand D, Kundu D, et al. The burden of scrub typhus in India: A systematic review. PLoS Negl Trop Dis. 2021; 15, e0009619.
[7] Kumar V, Kumar V, Yadav AK, et al. Scrub typhus is an under-recognized cause of acute febrile illness with acute kidney injury in India. PLoS Negl Trop Dis. 2014; 8, e2605.
[8] Bonell A, Lubell Y, Newton PN, et al. Estimating the burden of scrub typhus: A systematic review. PLoS Negl Trop Dis. 2017; 11, e0005838.
[9] Berman SJ, Kundin WD. Scrub typhus in South Vietnam. A study of 87 cases. Ann Intern Med. 1973; 79, 26-30.
[10] Watanabe Y, Mashimo S, Ichige H, et al. Scrub typhus mimicking the clinical course of infectious mononucleosis: a case report. J Rural Med 2021; 16, 62-66.
[11] Im JH, Choi SJ, Chung M-H, et al. A case of Henoch-Schönlein purpura associated with scrub typhus. BMC Infect Dis. 2020; 20, 286.
[12] Varghese GM, Dayanand D, Gunasekaran K, et al. Intravenous Doxycycline, Azithromycin, or Both for Severe Scrub Typhus. N Engl J Med. 2023; 388, 792-803.
[13] Gaba S, Gupta M, Singla N, et al. Clinical outcome and predictors of severity in scrub typhus patients at a tertiary care hospital in Chandigarh, India. J Vector Borne Dis. 2019; 56, 367-372.
[14] Karthik G, Sudarsan TI, Peter JV, et al. Spectrum of cardiac manifestations and its relationship to outcomes in patients admitted with scrub typhus infection. Pediatr Crit Care Med. 2018; 7, 16-23.
[15] Chin JY, Kang K-W, Moon KM, et al. Predictors of acute myocarditis in complicated scrub typhus: an endemic province in the Republic of Korea. Korean J Intern Med. 2018; 33, 323-330.
[16] Ki Y-J, Kim D-M, Yoon N-R, et al. A case report of scrub typhus complicated with myocarditis and rhabdomyolysis. BMC Infect Dis. 2018; 18, 551.
[17] Chang JH, Ju MS, Chang JE, et al. Pericarditis due to Tsutsugamushi disease. Scand J Infect Dis. 2000; 32, 101-102.
[18] Lee N-J, Shih H-I, Lin C-H, et al. Scrub Typhus Complicated With Fulminant Perimyocarditis. J Acute Med. 2023; 13, 84-88.
[19] Fang CY, Dennis DT, Lee JB. Electrocardiographic changes in scrub typhus patients. Southeast Asian J Trop Med Public Health. 1977; 8, 503-509.
[20] Gupta S, Jesrani G, Gaba S, et al. Scrub typhus manifesting as electrocardiographic disturbance: A case report and review of literature. Turk J Emerg Med. 2022; 22, 47-50.
[21] Moek F, Poe P, Charunwatthana P, et al. The reliability of the clinical examination in predicting hemodynamic status in acute febrile illness in a tropical, resource-limited setting. Trans R Soc Trop Med Hyg. 2018; 112, 200-205.
[22] Aronoff DM, Watt G. Prevalence of relative bradycardia in Orientia tsutsugamushi infection. Am J Trop Med Hyg. 2003; 68, 477-479.
[23] Choi S-W, Yun NR, Choi D-H, et al. Scrub Typhus and Abnormal Electrocardiography. Am J Trop Med Hyg. 2019; 100, 399-404.
[24] Manappallil RG, Nambiar J, Anil R. Afebrile scrub typhus infection with cardiac manifestation. BMJ Case Rep; 14. Epub ahead of print 13 April 2021. Doi: 10.1136/bcr-2020-240223.
[25] Jang S-Y, Kang K-W, Kim JH, et al. New-onset atrial fibrillation predicting for complicating cardiac adverse outcome in scrub typhus infection. Clin Cardiol. 2019; 42, 1210-1221.
[26] gupta h, parchani a, choudhury a, et al. atrial fibrillation in scrub typhus: a series of four cases. Cureus 2022; 14, e25338.
[27] Pradeesh A, Vasudevan B, Sharma N, et al. A rare case of scrub typhus vasculitis presenting as acute coronary syndrome diagnosed by skin manifestations. Indian J Dermatol Venereol Leprol. 2022; 88, 184-187.
[28] Pannu AK, Debnath MK, Sharma N, et al. Circulating cardiac biomarkers and echocardiographic abnormalities in patients with scrub typhus: A prospective cohort study from a tertiary care center in North India. J Vector Borne Dis. 2021; 58, 193.
[29] Charoensak A, Chawalparit O, Suttinont C, et al. Scrub typhus: chest radiographic and clinical findings in 130 Thai patients. J Med Assoc Thai. 2006; 89, 600-607.
[30] Ghosh R, Mandal A, León-Ruiz M, et al. Rare neurological and neuropsychiatric manifestations of scrub typhus: a case series of 10 cases. Neurologia. Epub ahead of print 28 July 2022. Doi: 10.1016/j.nrleng.2022.07.001.
[31] Garg D, Manesh A. Neurological Facets of Scrub Typhus: A Comprehensive Narrative Review. Ann Indian Acad Neurol. 2021; 24, 849-864.
[32] Basu S, Chakravarty A. Neurological Manifestations of Scrub Typhus. Curr Neurol Neurosci Rep. 2022; 22, 491-498.
[33] Agrawal A, Parida P, Rup AR, et al. Scrub Typhus in Paediatric Age Group at a Tertiary Care Centre of Eastern India: Clinical, Biochemical Profile and Complications. J Family Med Prim Care. 2022; 11, 2503-2506.
[34] Biswas U, Ghosh R, Chakraborty A, et al. Cerebral Venous Sinus Thrombosis Following Scrub Typhus Infection: A Case Report and a Review of the Literature. Med Res Arch. 10. Epub ahead of print October 2022. Doi: 10.18103/mra.v10i10.3196.
[35] Venketesan S, Jain D, Viswanathan S, et al. Case Report: Acute pyelonephritis and hearing loss in scrub typhus. F1000Res. 2019; 8, 312.
[36] Gupta S, Grover S, Gupta M, et al. Cerebellitis as a rare manifestation of scrub typhus fever. BMJ Case Rep; 13. Epub ahead of print 14 May 2020. Doi: 10.1136/bcr-2019-233993.
[37] Sawale VM, Upreti S, Singh TS, et al. A rare case of Guillain-Barre syndrome following scrub typhus. Neurol India. 2014; 62, 82-83.
[38] Sethuraman VK, Balasubramanian K. An unusual clinical presentation of scrub typhus. Cureus. 2019; 11, e5568.
[39] Saxena A, Khiangte B, Tiewsoh I. Scrub typhus complicated by acute respiratory distress syndrome and multiorgan failure; an unrecognized alarming entity in central India: a report of two cases. J Family Med Prim Care 2014; 3, 80-83.
[40] Chung J-H, Lim S-C, Yun N-R, et al. Scrub typhus hepatitis confirmed by immunohistochemical staining. World J Gastroenterol. 2012; 18, 5138-5141.
[41] Chaturvedi A, Gupta M, Bhardwaj S, et al. Scrub typhus masquerading as acute pancreatitis. BMJ Case Rep; 2016. Epub ahead of print 9 May 2016. Doi: 10.1136/bcr-2015-213929.
[42] Vikrant S, Dheer SK, Parashar A, et al. Scrub typhus associated acute kidney injury-a study from a tertiary care hospital from western Himalayan State of India. Ren Fail. 2013; 35, 1338-1343.
[43] Bhattarai T, Poudel SC, Pokharel N, et al. Scrub typhus as a rare cause of acute pyelonephritis: case report. BMC Infect Dis. 2020; 20, 322.
[44] Li W, Huang L, Zhang W. Scrub typhus with multi-organ dysfunction syndrome and immune thrombocytopenia: a case report and review of the literature. J Med Case Rep. 2019; 13, 358.
[45] Ono Y, Ikegami Y, Tasaki K, et al. Case of scrub typhus complicated by severe disseminated intravascular coagulation and death. Emerg Med Australas. 2012; 24, 577-580.
[46] Lin Y-H, Lin Y-H, Shi Z-Y. A case report of scrub typhus-associated hemophagocytic syndrome and a review of literature. Jpn J Infect Dis. 2014; 67, 115-117.
[47] Koraluru M, Bairy I, Varma M, et al. Diagnostic validation of selected serological tests for detecting scrub typhus. Microbiol Immunol. 2015; 59, 371-374.
[48] Coleman RE, Sangkasuwan V, Suwanabun N, et al. Comparative evaluation of selected diagnostic assays for the detection of IgG and IgM antibody to Orientia tsutsugamushi in Thailand. Am J Trop Med Hyg. 2002; 67, 497-503.
[49] Prakash JAJ, Abraham OC, Mathai E. Evaluation of tests for serological diagnosis of scrub typhus. Trop Doct. 2006; 36, 212-213.
[50] G K P, R R. A case series of scrub typhus in obstetrics. J Clin Diagn Res 2014; 8, OR01-3.
[51] Mahdi AS, Al-Khalili SM, Chung CC, et al. Scrub Typhus Complicated by ARDS, Myocarditis, and Encephalitis Imported to Oman from Nepal. Oman Med. J 2019; 34, 254-256.
[52] Chrispal A, Boorugu H, Gopinath KG, et al. Scrub typhus: an unrecognized threat in South India - clinical profile and predictors of mortality. Trop Doct. 2010; 40, 129-133.
[53] Mahajan SK. Scrub typhus. J Assoc Physicians India. 2005; 53, 954-958.
[54] Das S, Chattopadhyay S, Munsi K, et al. Scrub typhus with cerebral venous sinus thrombosis: a rare presentation. BMJ Case Rep; 14. Epub ahead of print 28 April 2021. DOI: 10.1136/bcr-2020-241401.
[55] Koti N, S Mareddy A, K Nagri S, et al. Dancing eyes and dancing feet in scrub typhus. Australas Med J. 2015; 8, 371-372.
[56] Cho JH, Lee CH. Pulmonary Artery Thrombosis Associated with Scrub Typhus. Infect Chemother. 2019; 51, 73-76.
[57] kariyawasam agta, palangasinghe dr, fonseka cl, et al. bilateral sensorineural deafness in a young pregnant female presenting with a fever: a rare complication of a reemerging disease-spotted fever group Rickettsioses. Case Rep Infect Dis. 2019; 2019, 5923146.
[58] Dixit J, Jadon RS, Ray A, et al. Scrub typhus with bilateral sensorineural hearing loss: A unique case report. J Vector Borne Dis. 2020; 57, 101-103.