Le Infezioni in Medicina, n. 2 , 236-241, 2021
ORIGINAL ARTICLES
Outcome of HBV screening and vaccination in a migrant population in southern Italy
Maria Mazzitelli1, Giuseppe Greco1, Francesca Serapide1, Vincenzo Scaglione1, Helen Morrone1, Nadia Marascio2, Aida Giancotti2, Maria Carla Liberto2, Giovanni Matera2, Enrico Maria Trecarichi1, Carlo Torti1
1Department of Medical and Surgical Sciences, Infectious and Tropical Diseases Unit, “Magna Graecia” University, Catanzaro, Italy;
2Department of Health Sciences, Clinical Microbiology Unit, “Magna Graecia” University, Catanzaro, Italy
Corresponding author
Maria Mazzitelli
E-mail: m.mazzitelli88@gmail.com
SummaRY
Chronic hepatitis B virus (HBV) infection is a major health problem worldwide. Although Italy is considered a low prevalence setting for HBV infection, following significant migration in recent years there has been an increase in the occurrence of the disease. Italian guidelines recommend that all migrants be screened, vaccinated and treated for HBV, as required. Unfortunately, screening and vaccination in this population can be challenging for several reasons. We therefore conducted an analysis to evaluate the efficacy and outcome of the pathways of care (from screening to treatment) for HBV in a population of migrants. We evaluated 330 migrants who came to our centre between August 2015 and October 2018, and who were residing in seven different centres for refugees and asylum seekers. At the first evaluation, only 30% of them had already received screening for HBV. After our intervention, 23 (6.9%) were diagnosed as HBsAg carriers, whereas 204 (61.8%) were potentially eligible for vaccination. At a follow-up evaluation of the latter group, only 56.9% had by then been vaccinated, 17.6% had the vaccination course ongoing, and 17.1% had not started their vaccination course. Among those who were HBsAg positive, 73.9% were still in care at month 6 of follow-up, and only 43.3% were in care one year later. Our results demonstrated that both screening and vaccination strategies for HBV need to be improved in migrant populations. Similarly, a reinforcement of the network to keep in care migrants who initiated treatment or deserve clinical monitoring is necessary.
Keyword: HBV, screening, vaccination, migrant.
INTRODUCTION
More than 300 million people worldwide suffer from chronic hepatitis caused by Hepatitis B Virus (HBV) and many of them die for its complications, such as liver cirrhosis or hepatocellular carcinoma (HCC) [1]. Deaths related to HBV complications amount to 780,000 every year [2]. Most patients do not report any symptom during acute infection, but in a small percentage of cases acute HBV infection can be fatal [3].
In Italy, the prevalence of chronic Hepatitis B surface Antigen (HBsAg) carriers is low (less than 2% of individuals), mainly thanks to mandatory vaccination campaigns established in 1992 [4]. However, Italy has recently been exposed to a huge migratory phenomenon that may increase the prevalence of this infection [5]. Indeed, most migrants come from hyper-endemic areas for HBV infection, where they are more likely to acquire the infection during childhood and are at a higher risk of developing chronic infection.
Guidelines recommend all migrants to be screened for chronic viral infections, including HBV [6-8]. It is also recommended, to perform vaccination for those who do not have immunization for HBV, according to serological status, and to treat those who meet specific criteria [9].
We conducted an analysis to evaluate the efficacy and outcome of the pathways of care for HBV (from screening to treatment) in migrant populations. The first objective was to evaluate whether the serological screening for HBV was adequately performed (including at least HBsAg, HBcAb and HBsAb). Secondly, we aimed at estimating the proportion of migrants who were vaccinated, among those who were susceptible. Lastly, after the first clinical check, we assessed the level of adherence to the proposed interventions (further analysis for screening, vaccinations, retention into care for those who were diagnosed as HBsAg carriers).
PATIENTS AND METHODS
The Infectious and Tropical Disease Unit of “Magna Graecia”, University of Catanzaro (Italy), coordinated the study. The setting was the migrant outpatient clinic, which is run once a week in our centre since August 2015. The study was conducted with the approval of the PARAMI study protocol, approved by the Local Ethics Committee (reference n°: n. 108, 27 April 2017). Study procedures were in accordance with the Declaration of Helsinki and with Principles of Good Clinical Practice.
We conducted a retrospective collection of data concerning HBV serology in migrants who were referred to our outpatient clinic by hosting centres for screening procedures (the patients were actively recruited by infectious diseases specialists). Six months and one year after the first clinical check performed in our centre, we contacted the hosting centres where migrants were residing, and checked if migrants had been following the advices that they were provided with. Migrants received the support of a cultural mediator during our observation time, in order to make them fully understand the objectives and importance of adhering to both screening and vaccination procedures for HBV.
All data regarding patients were collected in Excel® database. Data collected were: gender, age, country of origin, date of arrival in Italy, HBV serology results available at the first clinical check, and available vaccination records. Then, database was integrated with follow-up data.
Participants were categorised as follows: HBsAg positive (when Hepatitis B surface antigen was present), vaccinated and immune (those who displayed a negative score for HBsAg and HBcAb, and a HBsAb higher than 10 UI/ml at screening serological tests), naturally immunised (subjects who displayed a negative HBsAg, a positive HBcAb and a HBsAb higher than 10 UI/ml at screening serological tests) and those with occult HBV infection (OBI) without HBsAb (according to OBI definition given by Raimondo et al.) [10].
Statistical analysis was also performed, in order to explore any differences possibly associated with probability for HBsAg positive patients of being retained into the study or being lost to follow-up. Data are reported as mean, percentages, standard deviation (SD), as appropriate.
RESULTS
Patient characteristics and testing
During the study period (August 2015-October 2018), we evaluated 330 migrants who came to our centre and who were residing in seven different centres for refugees and asylum seekers (Figure 1). The epidemiological and demographic characteristics of the patients are reported in Table 1. Most migrants (197/330, 59.7%) were already in Italy for three months or longer.
At the first evaluation (see Figure 2), only 99/330 (30%) migrants had already received a screening for HBV soon after their arrival in Italy. Among those 99 migrants, 6 (6.1%) were HBsAg positive, but were not linked to any care system and had not performed any other test; 9 (9.1%) had already been vaccinated with a full schedule; 64 (64.6%) were eligible for vaccination; 11 (11.1%) had natural immunization; 9 (9.1%) had a seronegative occult HBV infection (OBI).
Two hundred and thirty one out of 330 (70%) subjects had never been screened before and were prescribed HBV testing after consultation in our centre. Among those 231 migrants, 28 (12.1%) refused further testing, 17 (7.3%) were HBsAg positive, 29 (13.6%) had natural immunity, 17 (7.3%) had seronegative OBI, and 140 (59.2%) were seronegative. Results of this screening and follow-up procedure are described in Figure 2.
Figure 1 - Map of the distribution of centres where the study population resided.
Table 1 - Epidemiological and demographic characteristics of our migrant population (n=330).
|
Characteristics |
N (%) |
|
Age (mean, SD) |
19.9 (11.5) |
|
Gender Male Female |
275 (83.3) 55 (16.7) |
|
Country of origin Bangladesh Congo Eritrea Gambia Guinea Iraq Ivory Coast Libia Mali Nigeria Other African Countries Pakistan Senegal Syria |
42 (12.7) 8 (2.5) 10 (3.1) 55 (16.7) 12 (3.6) 19 (5.7) 20 (6.1) 12 (3.6) 20 (6.1) 30 (9.1) 29 (8.8) 14 (4.2) 17 (5.1) 42 (12.7) |
|
Older than 18 years Yes No |
193 (58.5) 137 (41.5) |
|
Time from arrival in Italy to observation (mean, SD) Within 4 weeks From 5 to 11 weeks From 12 to 23 weeks From 24 to 27 weeks From 48 to 52 weeks Beyond 52 weeks |
29 (8.8) 104 (31.5) 31 (9.4) 58 (17.6) 34 (10.3) 74 (22.4) |
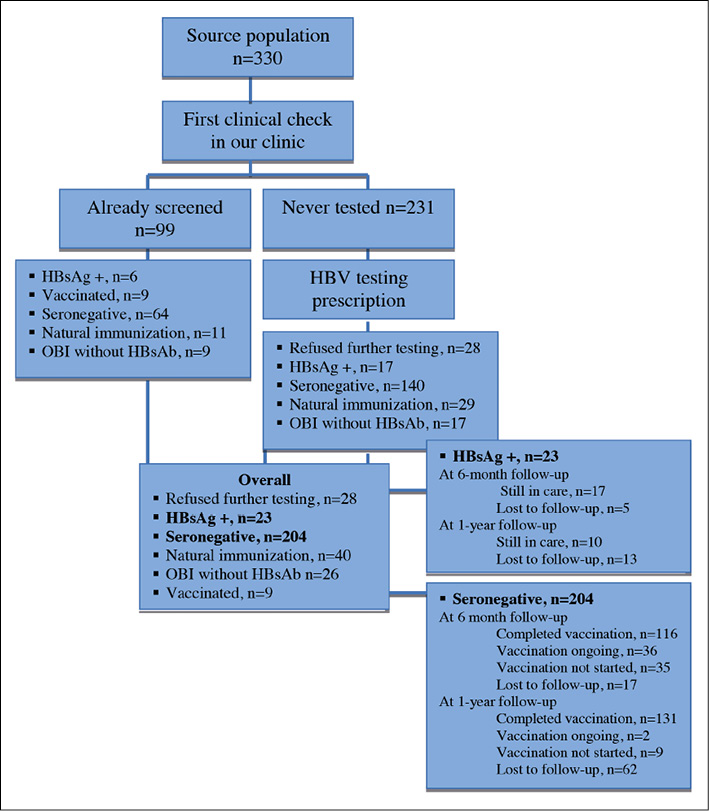
Figure 2 - Study flow.
Follow-up data on management of people who were HBsAg carriers
Overall, 23 out of 330 migrants (7%) were diagnosed as HBsAg positive. Following our advice, all of them were linked to care and performed abdominal ultrasound, liver function tests, alpha-fetoprotein test and transient elastography (according to current guidelines for the management of Hepatitis B) [5]. All of these tests were prescribed and booked by an Infectious Disease specialist. Treatment was prescribed for patients who met specific criteria (high liver stiffness at transient elastography, HBV DNA levels higher than 2,000 UI/ml, increased levels of ALT) [5]. Fifteen out of 23 (65.2%) presented moderate/severe liver disease, with high levels of HBV-DNA, and indication for treatment. Two of these patients (13.3%) were cirrhotic, even if very young (one 19-year-old male and one 18-year-old male).
At month 6 of follow-up, out of 23 patients who were HBsAg positive, 5 (21.7%) were lost to follow-up or transferred from their hosting centres and no further data are available about their treatment and process of care. After one year of follow-up, only 10 patients (43.4%) were still retained into care and were receiving treatment and their mean age was 21 years (SD: 0.2). Comparing HBsAg positive migrants who were lost to follow-up at the yearly evaluation (13/23) to those who were retained into care (10/23), the only characteristic associated with the likelihood of being lost to follow-up was the length of stay in Italy: indeed, HBsAg positive migrants who were residing in Italy for less than six months were more likely to be lost to follow-up compared to those residing in Italy for more than six months (9/13 vs 2/10, p=0.02).
Follow-up results on vaccination
After the first consultation and HBV testing prescription, 204/330 (61.8%) migrants resulted to be eligible for vaccination. At month 6 of follow-up, 116/204 (56.9%) had already been vaccinated, 36/204 (17.6%) had the vaccination course ongoing and 35/204 (17.1%) migrants had not started the vaccination course at all. Seventeen out of 204 (8.3%) migrants moved to other centres or were lost to follow-up and no data are available about any vaccination performed elsewhere. After one year of follow-up, among 204 who were potentially eligible for vaccination, only 142 (69.6%) migrants were still residing in their centres. Of these, 131/142 (92%) completed their vaccination course for HBV (mean age was 19.7 years, SD: 10.2), 2/142 (1.4%) had the vaccination course ongoing, and 9/142 (6.3%) migrants had not started the vaccination. Sixty-two migrants out of 204 (30.4%) left their centres, and 17 migrants had still to complete the vaccination course.
DISCUSSION
Considering the screening and vaccination strategies for migrants, our results clearly demonstrated that several issues are still ongoing; in fact, both timely screening and vaccination campaigns should be performed for migrants and refugees soon after their arrival in hosting countries.
Possible delays could be explained by inability of local health services to deal with the management of a considerable amount of people arriving in a short period of time. A shortage of both staff and facilities for vaccinations and screening procedures could also contribute. Indeed, among migrants who exhibited HBV serology at the first medical check and were potentially eligible for vaccination, only a small proportion was actually vaccinated. Moreover, more than 50% of our study population could have received vaccination after their arrival, since they showed negative results for all HBV markers at first clinical check and were in Italy for more than three months.
The proactive approach applied by our Infectious Disease specialist significantly improved the vaccination rate and linkage into the health care system. Applying guideline recommendations for screening in migrants is essential for two main reasons. Firstly, it is crucial to diagnose and to treat people who are at high risk for developing complications as soon as possible; indeed, despite the young age of our patients, in most cases a treatment was necessary, since all subjects had high HBV-DNA levels and/or increased liver stiffness. Two subjects, although very young, were already cirrhotic. Secondly, it is important to vaccinate non-immune subjects in order to prevent spreading of the infection, especially in small and restricted communities, where also other infectious diseases with similar mechanisms tend to spread widely [11]. Moreover, these two cost-effective preventive strategies would result in saving resources for the National Health Service.
By contrast, the adherence to the programs of screening and vaccination, as well as retention into care of HBsAg carrier patients among the migrant population, represent a major public health challenge.
Indeed, low level of adherence was confirmed to be frequent in this population during follow-up, especially for those who were residing in Italy for less than six months. Moreover, the lack of a National network dedicated to the follow-up of migrants who are on treatment for Hepatitis B is a crucial issue. We do not know, in fact, whether people who started treatment in our centre and then moved are still on treatment or not.
Therefore, increasing adherence has to be one of the main goals. In order to reduce loss to follow-up rate and non-adherent behaviours, a possible approach could be represented by health education campaigns among migrants. In fact, it is fundamental that migrants fully understand the importance of being tested for HBV, of preventing HBV infection through vaccination, and of treating the infection as needed. This remained a critical point in our experience, despite the presence of a cultural mediator during clinical checks. Furthermore, greater efforts by the Health Care Service are required, in order to facilitate access to care. In our case, prolonged contact with the hosting centres helped to reach higher rates of response, especially for vaccination.
The major limitation of this study is the lack of a long-term follow-up evaluation and the high proportion of people who were lost to follow-up (especially those who were HBsAg positive).
Moreover, people defined as OBI did not receive follow-up, therefore we were not able to assess any further need for treatment. Since other possible minor limitations may affect a retrospective study (such as limited number of patients and lack of interventions to improve adherence), confirmation of our findings by means of a prospective study would be advisable. Lastly, it would be interesting to program a multicentric study at a National level for an adequate and in-depth analysis of the issue.
Conflict of interest
Nothing to be disclosed.
Ethical approval
The study was conducted with the approval of the PARAMI study protocol, approved by the Local Ethics Committee (reference n°: n. 108, 27 April 2017).
Funding
Dr Maria Mazzitelli was supported as PhD student by European Commission (FESR FSE 2014-2020) and by Calabria Region (Italy). European Commission and Calabria Region cannot be held responsible for any use, which may be made of information contained therein.
REFERENCES
[1] Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: New estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012; 30 (12), 2212-9.
[2] Jefferies M, Rauff B, Rashid H, Lam T, Rafiq S. Update on global epidemiology of viral hepatitis and preventive strategies. World J Clin Cases. 2018; 6 (13), 589-99.
[3] Gilson R, Brook MG. Hepatitis A, B, and C. Sex Transm Infect. 2006; 82 (Suppl. 4), iv35-9.
[4] Niederau C. Chronic hepatitis B in 2014: Great therapeutic progress, large diagnostic deficit. World J Gastroenterol. 2014; 20 (33), 11595-617.
[5] Cuomo G, Franconi I, Riva N, et al. Migration and health: A retrospective study about the prevalence od HBV, HIV, HCVm tuberculosis and syphilis infeciotns amongts newly arrived migrants screened at the Infectious Diseases Unit of Modena, Italy. J Infec Pub Health. 2019; 12 (2), 200-204.
[6] Kärki T, Napoli C, Riccardo F, et al. Screening for infectious diseases among newly arrived migrants in EU/EEA Countries - Varying practices but consensus on the utility of screening. Int J Environ Res Public Health. 2014; 11 (10), 11004-14.
[7] Napoli C, Dente MG, Kärki T, Riccardo F, Rossi P, Declich S. Screening for infectious diseases among newly arrived migrants: Experiences and practices in Non-EU countries of the Mediterranean basin and black sea. Int J Environ Res Public Health. 2015; 12 (12), 15550-8.
[8] WHO. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection. Geneva: World Health Organization; 2015.
[9] Lampertico P, Agarwal K, Berg T, et al. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017; 67 (2), 370-98.
[10] Raimondo G, Locarnini S, Pollicino T, et al. Update of the statement on biology and clinical impact of occult hepatitis B virus infection. J Hepatol. 2019; 71 (2), 397-408.
[11] Mazzitelli M, Torti C, Greco G, et al. Prevalence of parasitic infections in migrants: Do official symptom-driven guidelines apply to the current situation? Infez Med. 2018; 26 (4)