Le Infezioni in Medicina, n. 2 , 216-223, 2021
ORIGINAL ARTICLES
Long-term clinical and serological follow-up of paediatric patients infected by SARS-CoV-2
Carmelina Calitri1, Francesca Fantone1, Stefania Benetti1, Maria Maddalena Lupica1, Maria Giovanna Ignaccolo1, Elena Banino1, Alice Viano1, Mariella Pace1, Annalisa Castella2, Flavio Gaido3, Franco Garofalo1, and the ASLTO3 Study Group on Paediatric COVID-19
1Department of Paediatrics, Infermi Hospital, ASLTO3, Turin, Italy;
2Department of Hygiene and Public Health, ASLTO3, Turin, Italy;
3Department of Diagnostics, ASLTO3, Turin, Italy
Corresponding author
Carmelina Calitri
E-mail: carmelina_calitri@libero.it
SummaRY
Studies concerning Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection in paediatrics are limited to children mainly selected from hospitals, where patients with complications and comorbidities are managed. We aimed to describe the course of the Coronavirus Disease 2019 (COVID-19) in a population of children enrolled by place of residence, from diagnosis to recovery, with a long-term clinical and serological follow-up. We identified patients aged <14 years old living in the Turin Health District 3 who had SARS-CoV-2 detected in at least one nasopharyngeal swab from 1st March to 1st June 2020. Epidemiological and clinical features of SARS-CoV-2 infection were collected by way of a telephone inquiry. Enrolled patients were tested for SARS-CoV-2 serology in order to provide evidence of seroconversion and persistence of specific antibodies some time after the infection. A total of 46 patients with SARS-CoV-2 infection/COVID-19 were identified. The main pattern of viral transmission was intra-family. Eleven children were totally asymptomatic. If symptoms appeared, the disease had a mild course. A single case of COVID-19-related respiratory insufficiency was registered. Among children who underwent serological evaluation, 84% had seroconversion. No significant differences in antibody development were found according to the age and the burden of the disease. Children tested farther from the primary infection had lower antibody index titer values than the others. In conclusion, COVID-19 has a good prognosis in paediatric age. Children are able to develop a valid immune response, although their index titers seem to decrease a long time after the disease.
Keywords: Paediatric, COVID-19, SARS-CoV-2, respiratory insufficiency, antibodies.
INTRODUCTION
At the end of December 2019, the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) was identified as a new member of the betacoronavirus family and as the causative agent of the Coronavirus Disease 2019 (COVID-19). It spread rapidly worldwide becoming responsible for the first 21st-century pandemic: on February 5th, 2021, there were more than 104 million confirmed cases of COVID-19, with over 2 million registered deaths [1].
During the early stages of the outbreak, it was thought that children were rarely affected by SARS-CoV-2 [2]. Successive reports suggested that children had the same risk as adults of being infected, but had fewer symptoms and a less aggressive course of the disease, with a lower fatality rate. In May 2020, the first reports on serious complications in children affected by COVID-19 emerged [2-4].
Major paediatric case studies enroll children selected from hospitals, where patients with complications and comorbidities are mainly managed. Moreover, follow-up data after their hospital discharge or about patients directly referred to the territorial medical services are lacking.
The purpose of this study was to describe the SARS-CoV-2 infection/COVID-19 course in a population of children selected by place of residence, from diagnosis to possible hospital admission and recovery, with a long-term clinical and serological follow-up.
PATIENTS AND METHODS
The Turin Sanitary District 3 (ASLTO3) is located in Turin (Piedmont Region, Italy) and covers a surface of 3,049 m2 with a population of 581,281 inhabitants. Two hospitals are located in this territory, with a Paediatric Department in each of them. On 1st June, 2020, the Turin Sanitary District 3 included 68,880 children aged <14 years old.
During the Italian lockdown period (from March to June 2020), all the nasopharyngeal swabs (NPS) for SARS-CoV-2 identification performed in the Piedmont region were registered on a regional online platform, still in use at the time of this publication.
By virtue of a systematic search on this platform, we identified all the patients aged <14 years old living in the ASLTO3 who performed a SARS-CoV-2 NPS for clinical or epidemiological reasons (COVID-19 suggesting symptoms and/or close contact with a COVID-19 patient) from 1st March to 1st June, 2020. Swabs were processed in certified laboratories by the Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) technology, ending in a qualitative result (positive/negative). We enrolled all the patients <14 years old with at least one SARS-CoV-2 positive NPS.
Epidemiological and clinical features of SARS-CoV-2 infection/COVID-19 in these children were collected by way of a telephone inquiry. Enrolled patients were invited to be tested for SARS-CoV-2 serology in order to provide evidence of seroconversion and persistence of specific antibodies a long time after the infection. Three serological methods were performed on a single serum sample per patient. Biosynex COVID-19 BSS (IgG/IgM - BI - Biosynex Swiss SA, Fribourg, Switzerland) is a rapid chromatographic immunoassay for the qualitative detection of IgG and IgM antibodies to SARS-CoV-2 in human whole blood, serum or plasma. The test target is the Spike (S) protein Receptor Binding Domain (RBD). Declared sensitivity and specificity for IgM are 92.6% and 99.2%, for IgG 100% and 99.5%. The same target was used by the Access SARS-CoV-2 IgG Assay by Beckman Coulter (BC- Beckman Coulter Inc, Brea, California, United States), a qualitative immunoassay that detects IgG. Declared sensitivity and specificity for IgG are 100% and 99.8% respectively. The Abbott (AB) SARS-CoV-2 IgG assay (Abbott Diagnostics, Abbott Park, Illinois, United States) is a chemiluminescent microparticle immunoassay for the qualitative detection of IgG against the SARS-CoV-2 nucleocapsid (N) protein. Declared sensitivity and specificity depend on time of testing [5].
Qualitative results and index values reported by AB and BC instruments were used in the analyses. Cut off values for positivity were 1.4 for AB serology and 1.0 for BC one.
Statistical analysis was performed using SPSS per Windows release 27.0 (SPSS Inc, Illinois USA). Data were described as absolute and relative frequencies for categorical variables, as mean and standard deviation (SD) or median and interquartile range (IQR) for continuous variables.
The distribution was assessed as normal with the Kolmogorov–Smirnov test. The chi-squared test was used to evaluate proportions, while the Student-t test was performed to evaluate comparisons within quantitative variables. Statistical significance was set at p<0.05, and all of the p-values were two-tailed. Correlations are expressed by the Pearson correlation coefficient (r).
The study was approved by the local Ethics Committee (protocol number 10073 of 23 July 2020).
All the parents signed an informed consent to allow their children to take part in the study protocol.
Patients’ anonymity has been preserved.
RESULTS
Population characteristics
From 1st March to 1st June, 2020, 46 paediatric patients were tested positive for SARS-CoV-2 among 548 children <14 years old who underwent an NPS (8%). The great majority (31) performed the test both for clinical (presence of suggestive symptoms) and epidemiological (presence of a COVID-19 relative) reasons, 12 as at least one of their family members was affected, and only 3 exclusively for symptoms development.
The median age of the study population was 8 years old (1 day old-13.8 years - Figure 1) with 22 male and 24 female. Ten sets of siblings were identified, for a total of 35 families involved in the analysis. No one had been vaccinated for flu in the 2019-2020 season. Eight patients born preterm, only one was <1 year old at the time of infection. Six patients were affected by mild chronic diseases (one atopic dermatitis, 5 inhalant allergies with asthma in one case only). For 39 (85%) children a COVID-19 close contact was identified within their own family (the mother in 21 cases, the father in 14, the grandmother in 3, the aunt in 1). For one child an Emergency Department (ED) access 2 weeks before symptom onset was considered a possible risk factor for SARS-CoV-2 infection.
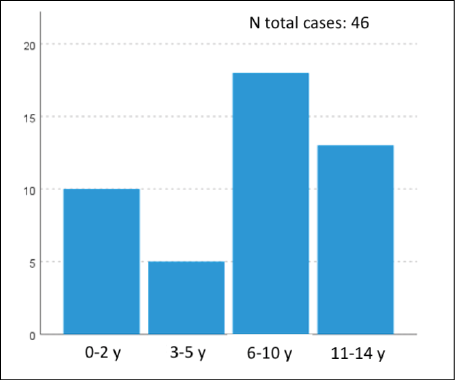
Figure 1 - Age distribution among the study population.
Table 1 - Clinical manifestations of COVID-19 in symptomatic patients.
|
Type of symptom |
Number of patients / all symptomatic children (35) |
Median days duration (IR) of symptoms |
|
Fever |
23/35 (71%) |
2 (1-21) |
|
Headache |
11/35 (31%) |
3 (1-7) |
|
Cough |
10/35 (28%) |
7 (3-45) |
|
Weakness |
9/35 (26%) |
3 (1-7) |
|
Diarrhoea |
9/35 (26%) |
2 (1-20) |
|
Anosmia |
7/35 (20%) |
10 (5-20) |
|
Muscle pain |
6/35 (17%) |
3,5 (1-7) |
|
Ageusia |
6/35 (17%) |
10 (5-20) |
|
Coryza |
3/35 (8%) |
32 (3-32) |
|
Conjunctivitis |
2/35 (6%) |
7,5 (7-8) |
|
Abdominal pain |
2/35 (6%) |
4,5 (1-7) |
|
Dyspnoea |
1/35 (3%) |
7 |
|
Sore throat |
1/35 (3%) |
12 |
|
Vomiting |
1/35 (3%) |
1 |
|
Rash |
1/35 (3%) |
7 |
SARS-CoV-2 infection clinical features
SARS-CoV-2 symptoms are summarized in Table 1: 35 children presented COVID-19, 11 were totally asymptomatic. All the patients performed at least 3 NPS (one at diagnosis and 2 negative control for recovery). In 32 cases the first NPS was processed at a median of 6.5 days (0-87) after symptom onset, in the remaining 3, it was performed before disease emergence as the patients were in close contact with a COVID-19 subject.
No relationship between age, sex or symptom development was found.
Symptomatic children performed a significantly major number of NPSs than asymptomatic ones (p=0.04). Sixteen children registered more than one positive swab, with a median of 26 days (17-46) persistence of positivity.
The majority of enrolled patients did not need a clinical evaluation; only 11 children were examined, mostly at the time of diagnosis (median 1.5 days – 0-32 after symptom onset) and mostly in ED (9). Four children needed a hospital stay: 3 infants <3 months of age (see below), and a 13-year-old girl found to be infected in a screening performed for a surgical intervention (appendectomy). In these patients, hospital stay was prolonged for a median of 4 days (1-29).
All children recovered from the disease without sequelae.
Particular cases
A 13-year-old male was evaluated in the ED for a prolonged cough (45 days), with anosmia and ageusia regressed after 5 days. Chest radiography and echography showed no evidence of pathological patterns. He presented 3 consecutive positive NPS covering a period of 38 days. The child was treated with two 5-day cycles of azithromycin with a total recovery.
A female neonate tested positive one day after her birth. Her mother presented with mild COVID-19 at labour. The baby was referred to an intensive care unit for close monitoring: no symptoms occurred and no alterations in hematological tests were found. SARS-CoV-2 was not detected in the maternal breast milk. She was discharged after 6 days of hospitalization. Successively, three consecutive SARS-CoV-2 NPS were positive, the first negative was registered after 46 days from diagnosis.
A 1-month-old girl, born preterm at 35+2 weeks from a twinning gestation, was admitted to the ED for initial lethargy and poor feeding, ending in acute respiratory insufficiency resulting in respiratory arrest. She was intubated and referred to a Neonatal Intensive Care Unit. She was supported with antibiotics for concomitant isolation of Haemophilus influenzae and Enterobacter cloacae in the bronchoalveolar fluid. No evidence of pneumonia and no neurological complications were found. She was discharged after a 28-day hospitalization with a total remission of symptoms. Two of her brothers tested positive for SARS-CoV-2 while her twin sister tested negative, all of them were totally asymptomatic.
A 2-month-old child had rhinitis and mild pharyngitis but was detained in hospital as her mother presented with respiratory distress at the ED.
SARS-CoV-2 serology
Thirty-two children were examined for SARS-CoV-2 serology (Table 2). It was performed at a median of 107.5 days (72-172) after the first SARS-CoV-2 detection in their NPS.
Table 2 - Serology testing results per patient.
|
Age (years)/ sex (male/female)/ symptomatic-asymptomatic |
Particular clinical conditions |
Interval (days) between first positive NPS- first negative NPS |
Interval (days) between first positive NPS-serology testing |
Index values AB IgG (vs N- protein) (pos >1.4) |
Index value BC IgG (vs RBD-domain of S-protein) (pos >1.0) |
|
12.3/female/aymptomatic |
15 |
72 |
1 |
2,5 |
|
|
13.6/female/symptomatic |
7 |
105 |
1,6 |
2 |
|
|
8.6/female/asymptomatic |
7 |
105 |
4,4 |
2 |
|
|
11.8/male/symptomatic |
30 |
83 |
1,6 |
0,4 |
|
|
8.5/male/symptomatic |
13 |
83 |
6,3 |
4,8 |
|
|
13.4/female/symptomatic |
18 |
122 |
3,6 |
2,9 |
|
|
12.3/female/symptomatic |
22 |
110 |
3,3 |
9,9 |
|
|
12.4/male/symptomatic |
EBV acute infection |
17 |
172 |
0 |
0 |
|
9.8/male/symptomatic |
9 |
147 |
2,7 |
1,1 |
|
|
0.7/female/symptomatic |
31 |
111 |
2,9 |
3 |
|
|
4/male/symptomatic |
17 |
157 |
0,8 |
0,5 |
|
|
12.6/male/symptomatic |
Prolonged cough |
38 |
157 |
0,7 |
0,3 |
|
8.2/male/symptomatic |
24 |
134 |
0,1 |
0 |
|
|
9.5/male/symptomatic |
17 |
83 |
7,1 |
2,3 |
|
|
6.9/male/asymptomatic |
14 |
85 |
4,3 |
1,6 |
|
|
10.7/female/symptomatic |
21 |
142 |
2,7 |
1,3 |
|
|
1.6/female/symptomatic |
10 |
110 |
7,6 |
8,8 |
|
|
13.8/male/symptomatic |
23 |
99 |
4 |
2,2 |
|
|
0.3/female/asymptomatic |
4 |
102 |
5,8 |
9,9 |
|
|
3.4/female/symptomatic |
15 |
91 |
5,8 |
4,3 |
|
|
9.7/female/symptomatic |
35 |
89 |
4,1 |
1,4 |
|
|
4.2/male/symptomatic |
19 |
91 |
4,9 |
3,9 |
|
|
0.7/female/symptomatic |
30 |
91 |
1,6 |
2,3 |
|
|
7/male/symptomatic |
11 |
103 |
0,1 |
0,1 |
|
|
7.7/male/symptomatic |
24 |
121 |
4,7 |
1 |
|
|
11.8/female/symptomatic |
23 |
121 |
1,9 |
1,9 |
|
|
9/male/asymptomatic |
17 |
133 |
1,9 |
1,3 |
|
|
5.4/male/asymptomatic |
17 |
133 |
3,1 |
2 |
|
|
0.1/female/symptomatic |
Acute respiratory insufficiency |
17 |
134 |
0,7 |
2,3 |
|
6.8/female/asymptomatic |
46 |
132 |
3,4 |
0,5 |
|
|
9/female/symptomatic |
16 |
92 |
6,6 |
3,9 |
|
|
6.4/male/symptomatic |
16 |
92 |
2,3 |
2,3 |
Abbreviations: Nasopharyngeal swab: NPS; AB: Abbott serology; BC: Beckmann-Coulter serology; EBV: Epstein-Barr virus.
No IgM were detected by the BI method. A total of 27 patients (84%) tested positive for at least one type of SARS-CoV-2 IgG. Twenty-three children (72%) had specific antibodies detected in all three methods. Two children resulted positive only to AB serology, whereas 2 tested positive only to BI and BC methods. Five (16%) of the enrolled patients have no IgG detected in any of the methods used. Among them, two had no COVID-19 contacts before diagnosis, none of their relatives became infected, and one resulted as being affected by Epstein-Barr Virus (EBV) acute infection.
Among the particular cases described, the 1-month-old child with acute respiratory insufficiency tested positive only to the BC method (index 2.3). The 13-year-old boy with a prolonged cough resulted negative for all the serological methods used.
No significant differences among asymptomatic and symptomatic children were found both in terms of serology results and index values (Table 3). No statistical significance between symptoms development and positive/negative AB and BC serology and/or their index values was found. Children with more than one positive NPS did not develop greater index values than the others.
The AB IgG average index values in Abbott positive children were 3±2.1. The BC IgG average index values in Beckman Coulter positive children were 2.6±2.5. Index values of AB and BC serology demonstrated a similar trend in positive patients (p<0.001 with Pearson’s coefficient r=0.639).
Children tested further after the SARS-CoV-2 infection diagnosis had lower AB and BC index values than the others (respectively p=0.005 with r= -0.485 and p=0.006 and r=-0.477).
Table 3 - Evaluation of Abbott and Beckman Coulter index values serology per sex and clinical manifestation.
|
Patients tested |
No. positive patients |
Male (n) |
Female (n) |
Symptomatic (n) |
Asymptomatic (n) |
|
|
IgG Abbott (N-protein) (average index value ±SD) |
32 |
25 |
2.8±2.3 (16) |
3.6±2.1 (16) |
3.1±2.3 (25) |
3.4±1.6 (7) |
|
IgG Beckman Coulter (RBD domain S-protein) (average index value ±SD) |
32 |
25 |
1.5±1.4 (16) |
3.7±3.1 (16) |
2.5±2.5 (25) |
2.8±3.2 (7) |
Sibling group
Apart from the study population, 5 more children underwent serology tests, according to their parents’request, as they were siblings of the enrolled patients. All of them had no SARS-CoV-2 RT-PCR identification at the time of the development of symptoms or contact. Three were mild symptomatic, two had no symptoms at the time of their relatives’ disease. All of them tested positive to the three serological methods used (IgM negative in BI methods, IgG positive in BI, AB and BC method). No one needed a medical evaluation and/or was hospitalized during the disease. No sequelae were found in this population.
DISCUSSION
We described the COVID-19 course in a paediatric population with no a-priori selection criteria and with a complete clinical follow-up, including evaluation of immunological response vs SARS-CoV-2.
Our study confirms what is already described regarding COVID-19 in children. The large burden of transmission is within households, and in our case series 85% of patients had a previously infected family member [2, 6]. Children are often asymptomatic, up to 35% of the cases described: the number of asymptomatic and symptomatic patients is equally balanced in our population compared with other studies [2, 7]. If patients develop symptoms, these are generally self-limited and do not need specific therapies [2, 7]. In our population, fever was the most frequent presenting symptom, followed by cough and weakness. Headaches are rarely described, presented by 31% of our patients [2, 8]. Gastrointestinal manifestations such as vomiting, diarrhea and abdominal pain were as frequent as the respiratory ones in our case studies, confirming the SARS-CoV-2 tropism for both locations [2, 8].
Why the paediatric age is so different from the adult one both in incidence and in disease severity is still unknown [8]. Many hypotheses have been formulated, mainly regarding the mediators necessary for viral entry (decreased expression of angiotensin-converting enzyme 2) and the immune system reaction (decreased toll-like receptor-induced responses, reduced proinflammatory cytokine production and a higher proportion of regulatory T cells) [8].
Complicated courses mostly concern early childhood and previously compromised children [2,4,9-11]. The Multisystem Inflammatory Syndrome in children (MIS-C) is a rare complication of COVID19, often affecting patients at school age, and may involve multiple vital organs requiring aggressive immunosuppressive treatment to recovery [3, 12]. COVID-19 can manifest as lethargy and poor feeding, with complications such as respiratory distress and pneumonia, rash and disseminated intravascular coagulation in neonates and infants [2]. The 1-month-old baby who presented with respiratory insufficiency and required intensive treatments was born preterm by twin-birth.
Currently, the great matter of debate is the development of an adequate and protective immune response after SARS-CoV-2 infection and how long it lasts in patients.
In our case series, we investigate the presence of SARS-CoV-2 specific antibodies in children who have recovered a long time after the infection. To our knowledge, this is one of the first case studies considering this aspect exclusively in the paediatric age.
To perform the most accurate analysis according to our means, we chose to use three different serology methods, each one evaluating antibodies directed vs a specific target. SARS-CoV-2 has 4 major structural proteins (S-protein, envelope, membrane and nucleocapsid-N). The S-protein is essential to viral fusion, entry and transmission; in particular, its N-terminal S1 subunit containing the RBD is responsible for virus binding with host cells. Many Authors suggest that the S-protein, in particular the RBD-S site, is the main strategical and potentially sole target for neutralizing antibodies [12-16]. With BI and BC serology we evaluated these types of antibodies.
AB serology detects specific antibodies vs N-protein. N-protein is extremely abundant inside the virus or inside infected cells, but it is shielded from antibodies by viral or cellular membranes. For this reason, it is unlikely that N-protein specific antibodies can directly neutralize SARS-CoV-2. However, their presence can be considered a marker of SARS-CoV-2 infection in positive patients. Notably, AB serology was used for a seroprevalence survey in Italy after the lockdown period.
When activated, B and T cells start the production of antibodies: IgM production is transient and leads to an isotype switch to IgA and IgG. The SARS-CoV-2 seroconversion window may range from a few days to 3 weeks after symptom onset. The median duration of the IgM detection period is reported to be 5 days, whereas IgG are detected at a median of 14 days after symptom onset [13,17]. As no one was enrolled with acute infection, none of our patients had IgM.
The seropositivity rate for SARS-CoV-2 IgG is reported to reach 100% if people are tested at the early stages of illness, with a peak at 40-50 days after disease onset. Later, a slight decrease of antibody titer is registered in adults [14-16]. This kinetics involves both S-protein specific antibodies and N-protein ones [16]. Our findings support these data. We tested the children at a median of 107 days after symptom onset or diagnosis, and we obtained a seropositivity rate of 84%. Patients tested further after the diagnosis demonstrated significantly lower index titers than the others, with the same kinetics for RBD-site specific antibodies and N-protein ones. We can hypothesize children tend to lose their systemic antibodies over time.
On the other hand, we know there are 5% of adults who do not seroconvert after SARS-CoV-2 infection [14]. None of our seronegative patients had a well-known immune deficiency. For two patients only (among them the child with acute EBV infection) a false positive SARS-CoV-2 NPS can be hypothesized, as the infection occurred during the lockdown period, a COVID-19 contact was not identified and no relatives became affected contemporarily or after their diagnosis [18].
In adults, the magnitude of humoral response seems to depend on the duration and gravity of SARS-CoV-2 manifestations: patients with a worse clinical classification had higher antibody titers than mild ones [15-17]. Mild disease was also associated with transient serum titers [17], as well as the 40% of asymptomatic individuals whose antibody response disappeared after 8 weeks [19]. This seems not to be valid in paediatric age. In our cohort, asymptomatic children showed the same ability to develop an acquired immune response vs SARS-CoV-2 as symptomatic ones, both in terms of antibody detection (a long time after the symptom onset) and in the index values registered: symptoms development does not seem to be relevant for antibody production in paediatric age. These findings are consistent with those of Weisberg et al., where children with different disease severities (with or without MIS-C) exhibited similar antibody profiles. However, patients with MIS-C seemed to have relative stability of antibody abundance over a period of 2-4 weeks after discharge [12].
Among adults, antibody titers have considerable variations depending on age [14, 15, 17]. Conversely, we did not evidence significant differences in terms of antibody development capability according to age in our children.
Twenty-five children (and all the 5 PCR-negative siblings tested) had specific antibodies vs RBD-S-protein, the target related to the virus neutralization in vitro; according to previous studies, they developed potential neutralizing antibodies with expectable protection against re-infection [13, 14, 17]. At the moment, children are excluded from vaccination programs, so this information regarding their acquired immunity vs SARS-CoV-2 may be very useful. Among common coronaviruses, neutralizing antibodies seem to provide protection from re-infection or attenuate disease, even if individuals are reinfected. The real durability of SARS-CoV-2 neutralizing antibodies in infected humans is not yet known, as well as the minimum titer that will protect them against re-infections. However, SARS-CoV-2 may induce specific memory T and B cells which seem to be durable over time and may play an important role in long-term protection even in seronegative people [20].
In conclusion, our study confirms a good COVID-19 prognosis in children. They are able to produce and maintain detectable antibodies, regardless of disease symptoms development, a long time after the onset of infection. However, further data about the persistence of humoral and cellular immunity over time are needed. Establishing a correlate of protection together with understanding antibody kinetics will be relevant in the paediatric population, which is actually left out of SARS-CoV-2 vaccination programs.
Conflicts of interest
No conflicts of interest to declare.
Funding
None
Acknowledgments
Thanks to prof. Franca Basta for language revision.
Here are the members of the ASLTO3 Study Group on paediatric COVID-19 who contributed to the realization of the study: Sandra Giordanino, Silvana Oderda, Sonia Zangara, Luca Roasio, Maria Rita Cavallo, Angela Gallone, Claudia Farenzena, Eleonora Brunatti, Rosarita Frand Genisot, Elisa Mondiglio, Barbara Troia.
REFERENCES
[1] World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available at: https://COVID-19.who.int. [accessed: 5 February 2021].
[2] Zimmermann P, Curtis N. COVID-19 in Children, Pregnancy and Neonates: A Review of Epidemiologic and Clinical Features. Pediatr Infect Dis J. 2020; 39 (6), 469-77.
[3] Nakra NA, Blumberg DA, Herrera-Guerra A, Lakshminrusimha S. Multi-System Inflammatory Syndrome in children (MIS-C) following SARS-CoV-2 infection: review of clinical presentation, hypothetical pathogenesis, and proposed management. Children (Basel). 2020; 7 (7), 69.
[4] Mercolini F, Donà D, Girtler Y, et al. First paediatric COVID-19 associated death in Italy. J Pediatr Child Health. 2020; doi: 10.1111/jpc.14994.
[5] Bryan A, Pepper G, Wener MH, et al. Performance characteristics of the Abbott Architect SARSCoV-2 IgG assay and seroprevalence in Boise, Idaho. J Clin Microbiol. 2020. 58:e00941-20.
[6] Munro APS, Faust SN. Addendum to: Children are not COVID-19 super spreaders: time to go back to school. Arch Dis Child. 2021; 106 (2), e9.
[7] Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020; 109 (6), 1088-95.
[8] Lingappan K, Karmouty-Quintana H, Davies J, Akkanti B, Harting MT. Understanding the age divide in COVID-19: why are children overwhelmingly spared? Am J Physiol Lung Cell Mol Physiol. 2020; 319 (1), L39-44.
[9] Garazzino S, Montagnani C, Donà D, et al. Multicentre Italian study of SARS-CoV-2 infection in children and adolescents, preliminary data as of 10 April 2020. Euro Surveill. 2020; 25 (18), 2000600.
[10] Patel PA, Chandrakasan S, Mickells GE, Yildirim I, Kao CM, Bennett CM. Severe paediatric COVID-19 presenting with respiratory failure and severe thrombocytopenia. Paediatrics. 2020; 146 (1), e20201437.
[11] Bellino S, Punzo O, Rota MC, et al. COVID-19 WORKING GROUP. COVID-19 Disease severity risk factors for paediatric patients in Italy. Paediatrics. 2020; 146 (4), e2020009399.
[12] Weisberg SP, Connors TJ, Zhu Y, et al. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat Immunol. 2021; 22 (1), 25-31.
[13] Yi X, Cao J. What to Expect from Antibody Assays of SARS-CoV-2? J Appl Lab Med. 2020; 5 (5), 1126-30.
[14] Wajnberg A, Amanat F, Firpo A, et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science. 2020; 370 (6521), 1227-30.
[15] Wang X, Guo X, Xin Q, et al. Neutralizing Antibodies Responses to SARS-CoV-2 in COVID-19 Inpatients and Convalescent Patients. Clin Infect Dis. 2020; 71 (10), 2688-94.
[16] Dan JM, Mateus J, Kato Y, et al. Immunological memory to SARS-CoV-2 assessed for greater than six months after infection. Science. 2021; 371 (6529), eabf4063.
[17] Cervia C, Nilsson J, Zurbuchen Y, et al. Systemic and mucosal antibody secretion specific to SARS-CoV-2 during mild versus severe COVID 19. J Allergy Clin Immunol. 2021; 147 (2), 545-57.
[18] Cohen R, Jung C, Ouldali N, et al. Assessment of spread of SARS-CoV-2 by RT-PCR and concomitant serology in children in a region heavily affected by COVID-19 pandemic. medRxiv 2020; doi: https://doi.org/10.1101/2020.06.12.20129221
[19] Long QX, Tang XJ, Shi QL, et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med. 2020; 26 (8), 1200-4.
[20] Cox RJ, Brokstad KA. Not just antibodies: B cells and T cells mediate immunity to COVID-19. Nat Rev Immunol. 2020; 20 (10), 581-2.