Le Infezioni in Medicina, n. 2, 209-215, 2021
ORIGINAL ARTICLES
Use of renin-angiotensin system inhibitors and clinical predictors of COVID-19 severity in a tertiary hospital in the city of Buenos Aires
Jessica Barochiner1,2, Rocío Martínez1,2, Patricia Roxana Conti1, Marcos José Marín1, Ery Ayelén Ko3, María Sol Osorno3
1Hypertension Section, Internal Medicine Department, Hospital Italiano de Buenos Aires, Buenos Aires, Argentina;
2Instituto de Medicina Traslacional e Ingeniería Biomédica (IMTIB), UE de triple dependencia CONICET - Instituto Universitario del Hospital Italiano (IUHI)- Hospital Italiano (HIBA), Buenos Aires, Argentina;
3Internal Medicine Residency, Internal Medicine Department, Hospital Italiano de Buenos Aires, Buenos Aires, Argentina
Corresponding author
Jessica Barochiner
E-mail: jessica.barochiner@hospitalitaliano.org.ar
SummaRY
Information regarding predictors of a worse COVID-19 prognosis in the South American population is scarce. We aimed to determine whether the blockade of the renin-angiotensin system is associated with a worse clinical course of COVID-19, and to evaluate what clinical variables are associated with COVID severity in our population. We included adult subjects with rtPCR-confirmed COVID-19. The use of renin system inhibitors was defined according to its registration in the electronic medical record or the hospital pharmacy registry during the previous three months. Our endpoint was a composite of death or mechanical ventilation requirement. Patients were followed up until discharge or death. A multiple logistic regression model was used to determine the predictors of the composite endpoint. In all, we included 4930 COVID+ patients, the median age was 52 years, and 48.1% were male. The endpoint occurred in 488 patients (9.9%). In adjusted analysis, neither angiotensin converting enzyme inhibitors nor angiotensin receptor blockers were associated with the outcome. Independent predictors of mortality and/or mechanical ventilation requirement were age, male sex, a history of diabetes and/or chronic kidney disease, smoking and dementia. To conclude, renin system inhibitors seem to be unrelated to COVID-19 severity, whereas prognosis is independently associated with age, male sex and comorbidities.
Keywords: COVID-19, renin system inhibitors, severity; mechanical ventilation, comorbidities.
INTRODUCTION
The outbreak of COVID-19, caused by a new beta coronavirus (SARS-CoV-2), has become an unprecedented pandemic, with considerable morbidity and mortality, having detected to date more than 100 million confirmed cases and more than 2 million deaths around the world so far (https://gisanddata.maps.arcgis.com/apps/opsdashboard/ index.html#/bda7594740fd40299423467b48e9ecf6).
Several reports in medical literature show that certain conditions, such as older age, the presence of cardiovascular risk factors and established cardiovascular disease are more frequent in patients infected by COVID-19 who have a worse evolution [1-4]. However, many of these studies involve unadjusted analyses.
On the other hand, patients with the aforementioned comorbidities are often treated with blockers of the renin-angiotensin system, such as converting enzyme inhibitors (ACEI) and Angiotensin II Receptor Blockers (ARB). Interestingly, controversy has been raised about the potential harm or benefits of these antihypertensive drugs in the context of COVID-19 infection [5-8]. In fact, SARS-CoV-2 virus uses the Angiotensin Converting Enzyme (ACE2) receptor to enter cells [9]. Some studies show that ACEI and ARB cause an over-expression of this receptor in animal models, which could increase the susceptibility to SARS-CoV [10, 11]. At the same time, there is also evidence that the activation of the renin-angiotensin system and the down-regulation of ACE2 caused by SARS-CoV might be involved in the lung injury induced by the virus [12]. Under this second perspective, the use of ACEI/ARB, in addition to its proven benefits in patients with cardiovascular disease, could reduce lung injury resulting from the activation of the renin-angiotensin system. Some studies, mainly in the Asian and Anglo-Saxon populations, seem to show that ACEI/ARB per se are not associated with a worse evolution of COVID-19 [13-15]. Studies conducted in Latin American populations are currently very scarce. The particular characteristics of these populations, as well as their distinctive pharmacogenetic profile, would prevent the extrapolation of data from other cultures. The association between the renin inhibitors and COVID severity and the factors related to a worse evolution could in fact be different. Therefore, we aimed to determine whether the use of ACEI/ARB is associated with a worse clinical evolution of COVID-19 infection, in terms of mortality or requirement for mechanical ventilation, as well as to evaluate what other clinical variables are associated with this worse evolution in a tertiary university hospital in the city of Buenos Aires.
PATIENTS AND METHODS
Design and population
This was an ambispective cohort that pertains to our COVID-19 institutional registry. We included patients with a confirmed-COVID-19 diagnosis with rtPCR, between March 12th and October 10th, 2020, who had a complete follow-up in our hospital. Pregnant women were excluded.
The design of the study complied with the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1964 and Declaration of Tokyo, 1975, as revised in 2008). The study protocol was approved by the local ethics committee (Comité de Ética de Protocolos de Investigación, #5625). The patients duly authorized the use of the information in their medical records under the protection of their confidentiality through informed consent.
Definition of clinical variables
As part of the COVID-19 institutional registry, a form was filled out for each patient with a confirmed diagnosis, gathering data on age, sex, history of hypertension, diabetes, chronic kidney disease, coronary heart disease, peripheral vascular disease, cerebrovascular disease, heart failure, asthma, Chronic Obstructive Pulmonary Disease (COPD), smoking habits, history of dementia and current institutionalization in a geriatric facility. This piece of information was collated and validated in comparison to the electronic health care records.
The use of ACEI or ARB was defined according to its registration in the electronic medical record at the time of the diagnosis or the hospital pharmacy registry during the previous three months.
The evaluated end-point was a composite of death or mechanical ventilation requirement. Patients were followed up until epidemiological discharge or death.
Statistical analysis
Among the possible analytical strategies to determine the association between the use of ACEI/ARB and other clinical variables with the evolution of COVID-19, we opted to use logistic regression, given its greater interpretability [16]. We consider this to be a valid option given that the pathology implies a brief follow-up, where no significant losses are expected during it, so censored observations should not be a problem. Unadjusted and adjusted odds ratios (OR) with their respective 95% confidence intervals were estimated. A two-tailed p value <0.05 was considered statistically significant.
RESULTS
In this study 4,930 COVID-19 positive patients were included. Among them, 48.1% were male, the median age was 52 years (interquartile range 36-70), 26.3% were hypertensive, 9% were diabetic and 3.7% had a history of chronic kidney failure. The baseline characteristics are showed in Table 1.
Table 1 - Baseline characteristics of the study population.
|
Variable |
All patients |
On ACEI/ARB |
Not on ACEI/ARB |
p value |
|
n=4930 |
n=788 |
n=4142 |
||
|
Age, years (IQR) |
52 (36-70) |
74 (63-86) |
47 (34-63) |
<0.001 |
|
Male sex, % (n) |
48.1 (2372) |
47.6 |
50.6 |
0.1 (ns) |
|
Hypertension, % (n) |
26.3 (1298) |
83.4 |
15.5 |
<0.001 |
|
Diabetes, % (n) |
9 (442) |
21.6 |
6.6 |
<0.001 |
|
CKD, % (n) |
3.7 (183) |
9.5 |
2.6 |
<0.001 |
|
CHD, % (n) |
3.3 (161) |
10.9 |
1.8 |
<0.001 |
|
PVD, % (n) |
1.6 (77) |
4.9 |
1 |
<0.001 |
|
Cerebrovascular disease, % (n) |
4.8 (237) |
13.6 |
3.1 |
<0.001 |
|
Heart failure, % (n) |
5 (245) |
14 |
3.3 |
<0.001 |
|
Asthma, % (n) |
3.3 (161) |
4.6 |
3 |
0.03 |
|
COPD, % (n) |
3.5 (171) |
8.4 |
2.5 |
<0.001 |
|
Current smoker, % (n) |
9.4 (461) |
14.7 |
8.3 |
<0.001 |
|
Past smoker, % (n) |
13.5 (668) |
24.8 |
11.4 |
<0.001 |
|
Dementia, % (n) |
4.6 (229) |
10.4 |
3.6 |
<0.001 |
|
Institutionalized, % (n) |
4.1 (200) |
11 |
2.7 |
<0.001 |
CHD, coronary heart disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; IQR, interquartile range; ns, non-significant; PVD, peripheral vascular disease.
Regarding the use of ACEI/ARB, 16% of patients (n=788) were on treatment with these drugs. In particular, 420 patients were taking ACEI, and 368 were taking ARB. The patients who used these drugs, compared to those who did not, were older and had a more frequent history of hypertension, diabetes, chronic kidney disease, coronary disease, peripheral vascular disease, cerebrovascular disease and heart failure. In addition, those treated with ACEI/ARB had a higher chance to be institutionalized in a geriatric facility and to have dementia (Table 1).
During follow-up, the combined end-point occurred in 488 patients (9.9%). There were 396 deaths (8%) and 174 patients required mechanical ventilation (3.5%). The Figure 1 depicts the number of COVID-19 cases and the occurrence of the end-point per decade of life.
In the unadjusted analyses, both previous uses of ACEI or ARB showed a significant association with mortality or mechanical ventilation requirement: OR 3.5 (95%CI 2.7-4.4, p<0.001) for ACEI, and OR 2.8 (95%CI 2.1-3.6, p<0.001) for ARB. However, in the adjusted analysis, statistical significance was lost (OR 1.1 [95% CI 0.8-1.5] and OR 0.9 [95% CI 0.7-1.3]), for ACEI and ARB, respectively, after controlling for age, sex and co-morbidities. On the other hand, the predictors that were significantly associated with a worse evolution of COVID-19 in the multivariable analysis were: older age, male sex, a history of diabetes and/or chronic kidney disease, being a smoker and having a diagnosis of dementia (Table 2).
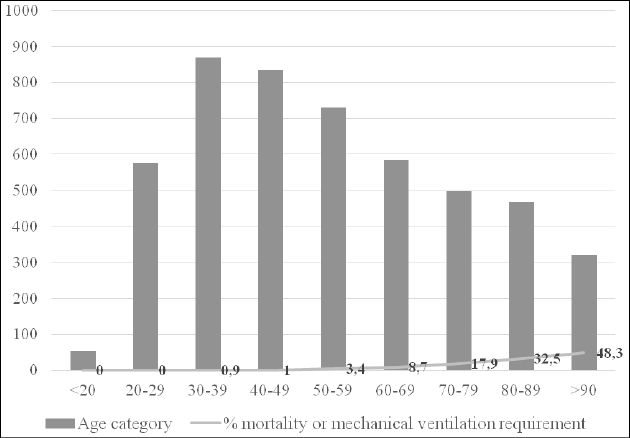
Figure 1 - Number of COVID-19 cases and occurrence of the composite end-point per decade of life.
Table 2 - Multiple logistic regression analysis for the composite end-point (mortality and/or mechanical ventilation requirement).
|
Variable |
OR (95%CI) |
p value |
|
ACEI |
1.1 (0.8-1.5) |
0.5 (ns) |
|
ARB |
0.9 (0.7-1.3) |
0.9 (ns) |
|
Age* |
2.4 (2.2-2.6) |
<0.001 |
|
Male sex |
1.9 (1.5-2.4) |
<0.001 |
|
Hypertension |
1 (0.8-1.3) |
0.9 (ns) |
|
Diabetes |
1.5 (1.1-1.9) |
0.01 |
|
CKD |
2.1 (1.4-3.2) |
<0.001 |
|
CHD |
1.1 (0.7-1.7) |
0.7 (ns) |
|
PVD |
1.2 (0.7-2.2) |
0.5 (ns) |
|
Cerebrovascular disease |
1.1 (0.7-1.5) |
0.8 (ns) |
|
Heart failure |
1.3 (0.9-1.8) |
0.2 (ns) |
|
Asthma |
1.1 (0.6-2.1) |
0.7 (ns) |
|
COPD |
1 (0.7-1.5) |
0.9 (ns) |
|
Current smoker |
1.7 (1.2-2.4) |
0.003 |
|
Past smoker |
0.9 (0.6-1.2) |
0.4 (ns) |
|
1.5 (1.03-2.1) |
0.03 |
|
|
Institutionalized |
0.8 (0.6-1.2) |
0.3 (ns) |
*For each 10 year-increase. ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CHD, coronary heart disease; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; ns, non-significant; PVD, peripheral vascular disease.
DISCUSSION
In this study, we found that the use of ACEI or ARB is not associated with a worse COVID-19 prognosis. On the other hand, being older, male, smoker, and having a history of diabetes, chronic kidney disease or dementia are all independent predictors of COVID-19 severity.
Since the beginning of the pandemic, the use of renin-angiotensin system inhibitors was questioned because of its potentially harmful effect, given that these drugs may up-regulate ACE2, an enzyme the virus uses to enter the cells it infects [9]. However, in accordance with our results, several observational studies currently support the fact that ACEI/ARB do not seem to be harmful in the context of the COVID-19 infection [17-19]. As a matter of fact, they may be protective, especially in some sub-populations such as hypertensive patients [20-22]. In fact, many scientific societies have advocated for the continuation of these drugs in patients chronically treated with them that become infected. Experts argue that ACEI/ARB may counterbalance the virus-induced reduction in pulmonary ACE2 by increasing the expression of ACE2. This would lower the production of inflammatory cytokines, exerting a protective role on lung injury [23, 24].
Other factors, such as older age, have been described to be consistently related to a worse COVID-19 prognosis across different studies [25-27]. In a meta-analysis conducted by Fang et al., including more than 10,000 COVID-19 cases from 61 studies, older age was significantly associated with COVID-19 severity. The biggest standard mean difference (SMD) was detected for death (SMD: 1.06, 95% CI: 0.85-1.26, p<0.001). This fact could be influenced both by the physiological aging process and, especially, by the higher prevalence of frailty and co-morbidities in elderly patients that contribute to a decrease in functional reserve that reduces the intrinsic capacity to react to infections [28].
In accordance with our results, the male sex was described as an independent predictor of COVID-19 severity in literature [29-31]. Many factors have been considered to explain this gender difference: a higher expression of angiotensin-converting enzyme-2 in men, sex-based immunological differences driven by sex hormones and X chromosome, differences in lifestyle (e.g., higher levels of smoking and drinking among men compared to women) and a less responsible attitude towards the COVID-19 pandemic in men than women, the former being more reluctant to adopt preventive measures such as frequent hand-washing, wearing a face mask, and obeying stay-at-home orders [32].
Moreover, in accordance with this work, co-morbidities such as diabetes and chronic kidney disease have consistently shown a significant association with COVID-19 prognosis in multivariable analyses. Iaccarino et al., for example, found that both co-morbidities doubled the chance of death in COVID-19 infected patients [33]. In turn, in a study conducted by Sun et al. in patients with COVID-19, both diabetes and chronic kidney disease were found to be independent predictors of death (OR 5.26 and 2.71, respectively) and acute respiratory distress syndrome and/or respiratory failure (OR 4.38 and 3.53 for diabetes and chronic kidney disease, respectively) [34]. Other studies have also confirmed the prognostic value of these co-morbidities [35, 36].
As regards smoking habits, some studies - like this - have found an independent association with COVID-19 severity, while others have not. For instance, in a Provincial-level ecological study conducted in Iran that included 43,950 lab-confirmed COVID-19 hospitalizations and 5,391confirmed COVID-19 deaths, provinces with a higher prevalence of cigarette smoking (incidence rate ratio 1.81; 95% CI: 1.01, 3.27) had a higher likelihood of COVID-19 death rates [37]. Moreover, in a study conducted by Liu et al., multivariable logistic analyses indicated that a history of smoking was an independent risk factor for disease progression [38]. Different mechanisms have been proposed for the association, such as a depletion of glutathione levels in smokers, which is essential for the proper functioning of the immune system [39]. On the other hand, in a nationwide, Italian observational study conducted by Polverino et al., including data from 3,179 COVID-19 inpatients, and in a meta-analysis conducted by Silverio et al. including 45 studies and 18,000 patients, smoking did not significantly affect mortality [40, 41]. It is possible that selection biases and confounders such as gender might play a role in these paradoxical results.
Hypertension is also a variable with conflicting results: early in the course of the pandemic, this risk factor was consistently described to be more frequently found among those with the worse COVID-19 prognosis [42, 43]. However, when studies performing adjusted analyses became available, many failed to detect hypertension as an independent risk factor for COVID-19 severity [33, 34, 44]. This was the case in our study. It has been hypothesized that the association between hypertension and COVID-19 prognosis probably varies according to the severity of hypertension and the presence of other risk factors, such as end-organ damage or established cardiovascular disease [45].
Regarding the history of cardiovascular disease, this study did not find any association with COVID-19 severity. There are conflicting results on this issue: while some studies did not find a relationship, others showed that established cardiovascular disease such as heart failure and ischemic heart disease were related to a worse clinical evolution [26, 46-48].
One interesting finding in our study is that dementia is an independent predictor of COVID prognosis. Few studies have also found this association [49]. A worse baseline health status, delayed access to health care and inability to express some initial symptoms have been postulated as possible explanations for a higher risk for a worse outcome in this population [50].
Finally, results in this work must be interpreted within the context of the study limitations. First, this is a single center study, representative of Argentine middle-class medicated hypertensives, mainly of European descent. Therefore, our results may not be generalizable to other populations. Moreover, we do not have information on the grade of control of risk factors such as hypertension and diabetes, such as data on whether ACEI or ARB were continued during the course of COVID-19 infection, which could have influenced the outcomes. On the other hand, our study has also some strengths: regarding the registration of events, our hospital has a long history in the use of electronic medical records focused on the patient, being the first Argentine hospital certified as 100% computerized by the Society of Information Systems and Management in Health (HIMSS). This results in a high-quality recording of the events of the present study. Another strength is that the analysis of possible predictors of a worse COVID outcome is adjusted for potential confounders.
In conclusion, after adjusting for age, sex and comorbidities, the use of ACEI or ARB was not associated with a worse outcome of COVID-19, in terms of mortality or the requirement for mechanical ventilation. The independent predictors of this worse evolution were older age, male sex, a history of diabetes and/or chronic kidney failure, smoking habits, and dementia.
Conflict of interest
The authors declare that there are not conflicts of interest.
Funding
None
REFERENCES
[1] Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. [The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China]. Zhonghua Liu Xing Bing Xue Za Zhi. 2020; 41 (2), 145-51.
[2] Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395 (10229), 1054-62.
[3] Guan WJ, Liang WH, Zhao Y, et al. China Medical Treatment Expert Group for Covid-19. Comorbidity and its impact on 1590 patients with Covid-19 in China: A Nationwide Analysis. Eur Respir J. 2020; 55 (5), 2000547.
[4] Yang J, Zheng Y, Gou X, et al. Prevalence of co-morbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020; 94, 91-5.
[5] Kuster GM, Pfister O, Burkard T, et al. SARS-CoV2: should inhibitors of the renin-angiotensin system be withdrawn in patients with COVID-19? Eur Heart J. 2020; 41 (19), 1801-3.
[6] Danser AHJ, Epstein M, Batlle D. Renin-Angiotensin System Blockers and the COVID-19 pandemic: at present there is no evidence to abandon renin-angiotensin system blockers. Hypertension. 2020; 75 (6), 1382-5.
[7] Patel AB, Verma A. COVID-19 and Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: What Is the Evidence? JAMA. 2020; 323 (18), 1769-70.
[8] Vaduganathan M, Vardeny O, Michel T, et al. Renin-Angiotensin-Aldosterone System Inhibitors in patients with Covid-19. N Engl J Med. 2020; 382 (17), 1653-9.
[9] Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 Cell entry depends on ACE2 and TMPRSS2 and is Blocked by a clinically proven protease inhibitor. Cell. 2020; 181 (2), 271-80.e8.
[10] Ferrario CM, Jessup J, Chappell MC, et al. Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation. 2005; 111 (20), 2605-10.
[11] Ishiyama Y, Gallagher PE, Averill DB, et al. Up-regulation of angiotensin-converting enzyme 2 after myocardial infarction by blockade of angiotensin II receptors. Hypertension. 2004; 43 (5), 970-6.
[12] Kuba K, Imai Y, Rao S, et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat Med. 2005; 11 (8), 875-9.
[13] Reynolds HR, Adhikari S, Pulgarin C, et al. Renin-Angiotensin-Aldosterone System Inhibitors and Risk of Covid-19. N Engl J Med. 2020; 382 (25), 2441-8.
[14] de Abajo FJ, Rodríguez-Martín S, Lerma V, et al.; MED-ACE2-COVID19 study group. Use of renin-angiotensin-aldosterone system inhibitors and risk of COVID-19 requiring admission to hospital: a case-population study. Lancet. 2020; 395 (10238), 1705-14.
[15] Zhang P, Zhu L, Cai J, et al. Association of inpatient use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ Res. 2020; 126 (12), 1671-81.
[16] Katz M. Multivariable Analysis A Practical Guide for Clinicians and Public Health Researchers. Third Edition. Cambridge University Press; 2011.
[17] Flacco ME, Acuti Martellucci C, Bravi F, et al. Treatment with ACE inhibitors or ARB and risk of severe/lethal COVID-19: a meta-analysis. Heart. 2020; 106 (19), 1519-24.
[18] Baral R, White M, Vassiliou VS. Effect of Renin-Angiotensin-Aldosterone System Inhibitors in patients with COVID-19: a Systematic Review and Meta-analysis of 28,872 Patients. Curr Atheroscler Rep. 2020; 22 (10), 61.
[19] Covino M, De Matteis G, Burzo ML, et al. Gemelli against COVID-19 Group. Angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers and prognosis of hypertensive patients hospitalised with COVID-19. Intern Med J. 2020; 50 (12), 1483-91.
[20] Pirola CJ, Sookoian S. Estimation of Renin-Angiotensin-Aldosterone-System (RAAS)-Inhibitor effect on COVID-19 outcome: A Meta-analysis. J Infect. 2020; 81 (2), 276-81.
[21] Zhang X, Yu J, Pan LY, et al. ACEI/ARB use and risk of infection or severity or mortality of COVID-19: A systematic review and meta-analysis. Pharmacol Res. 2020; 158, 104927.
[22] Barochiner J, Martínez R. Use of inhibitors of the renin-angiotensin system in hypertensive patients and COVID-19 severity: A systematic review and meta-analysis. J Clin Pharm Ther. 2020; 45 (6), 1244-52.
[23] Ferrario CM, Strawn WB. Role of the renin-angiotensin-aldosterone system and proinflammatory mediators in cardiovascular disease. Am J Cardiol. 2006; 98 (1), 121-8.
[24] Huang F, Guo J, Zou Z, et al. Angiotensin II plasma levels are linked to disease severity and predict fatal outcomes in H7N9-infected patients. Nat Commun. 2014; 5 (1), 1-7.
[25] Grasselli G, Zangrillo A, Zanella A, et al. COVID-19 Lombardy ICU Network. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020; 323 (16), 1574-81.
[26] Araujo M, Ossandón P, Abarca AM, et al. Pronóstico de pacientes hospitalizados por COVID-19 en un centro terciario en Chile: estudio de cohorte [Prognosis of patients with COVID-19 admitted to a tertiary center in Chile: A cohort study]. Medwave. 2020; 20 (10), e8066. Spanish.
[27] Working group for the surveillance and control of COVID-19 in Spain; Members of the Working group for the surveillance and control of COVID-19 in Spain. The first wave of the COVID-19 pandemic in Spain: characterisation of cases and risk factors for severe outcomes, as at 27 April 2020. Euro Surveill. 2020; 25 (50), 2001431.
[28] Fang X, Li S, Yu H, et al. Epidemiological, co-morbidity factors with severity and prognosis of COVID-19: a systematic review and meta-analysis. Aging (Albany NY). 2020; 12 (13), 12493-503.
[29] Gupta S, Hayek SS, Wang W, et al. STOP-COVID investigators. factors associated with death in critically ill patients with coronavirus disease 2019 in the US. JAMA Intern Med. 2020; 180 (11), 1-12.
[30] Izurieta HS, Graham DJ, Jiao Y, et al. Natural history of COVID-19: Risk factors for hospitalizations and deaths among >26 million U.S. Medicare beneficiaries. J Infect Dis. 2020; 223 (6), 945-56.
[31] Ryan C, Minc A, Caceres J, et al. Predicting severe outcomes in Covid-19 related illness using only patient demographics, co-morbidities and symptoms. Am J Emerg Med. 2020; S0735-6757(20)30809-3.
[32] Bwire GM. Coronavirus: Why men are more vulnerable to Covid-19 than women? SN Compr Clin Med. 2020; 1-3. doi: 10.1007/s42399-020-00341-w. Epub ahead of print.
[33] Iaccarino G, Grassi G, Borghi C, et al. SARS-RAS Investigators. Age and multimorbidity predict death among COVID-19 patients: results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension. 2020; 76 (2), 366-72.
[34] Sun Y, Guan X, Jia L et al. Independent and combined effects of hypertension and diabetes on clinical outcomes in patients with COVID-19: A retrospective cohort study of Huoshen Mountain Hospital and Guanggu Fangcang Shelter Hospital. J Clin Hypertens (Greenwich). 2021; 23 (2), 218-31.
[35] Huang I, Lim MA, Pranata R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia - A systematic review, meta-analysis, and meta-regression. Diabetes Metab Syndr. 2020; 14 (4), 395-403.
[36] Gok M, Cetinkaya H, Kandemir T, et al. Chronic kidney disease predicts poor outcomes of COVID-19 patients. Int Urol Nephrol. 2021; 1-8. doi: 10.1007/s11255-020-02758-7. Epub ahead of print.
[37] Khorrami Z, Nili S, Sharifi H, et al. Association of cigarette smoking, obesity, and underlying medical conditions with COVID-19 hospitalization and mortality in Iran: A nationwide retrospective ecological study. Med J Islam Repub Iran. 2020; 34, 133.
[38] Liu W, Tao ZW, Wang L, et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin Med J (Engl). 2020; 133 (9), 1032-8.
[39] Khanfar A, Al Qaroot B. Could glutathione depletion be the Trojan horse of COVID-19 mortality? Eur Rev Med Pharmacol Sci. 2020; 24 (23), 12500-9.
[40] Polverino F, Stern DA, Ruocco G, et al. ItaliCO study group. Comorbidities, Cardiovascular Therapies, and COVID-19 Mortality: A Nationwide, Italian Observational Study (ItaliCO). Front Cardiovasc Med. 2020; 7, 585866.
[41] Silverio A, Di Maio M, Citro R, et al. Cardiovascular risk factors and mortality in hospitalized patients with COVID-19: systematic review and meta-analysis of 45 studies and 18,300 patients. BMC Cardiovasc Disord. 2021; 21 (1), 23.
[42] Guan WJ, Ni ZY, Hu Y et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382, 1708-20.
[43] Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 Hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020; 323 (11), 1061-9.
[44] Chen C, Chen C, Yan JT, et al. Analysis of myocardial injury in patients with COVID-19 and association between concomitant cardiovascular diseases and severity of COVID-19. Zhonghua Xin Xue Guan Bing Za Zhi. 2020; 48 (7), 567-71.
[45] Salazar MR. Is hypertension without any other comorbidities an independent predictor for COVID-19 severity and mortality? J Clin Hypertens (Greenwich). 2021; 23 (2), 232-4.
[46] Ramos-Rincon JM, Buonaiuto V, Ricci M, et al. SEMI-COVID-19 Network. Clinical Characteristics and Risk Factors for Mortality in Very Old Patients Hospitalized with COVID-19 in Spain. J Gerontol A Biol Sci Med Sci. 2021; 25; 76 (3), e28-e37.
[47] Rodilla E, Saura A, Jiménez I, et al. Association of hypertension with all-cause mortality among hospitalized patients with COVID-19. J Clin Med. 2020; 9 (10), 3136.
[48] Wendel Garcia PD, Fumeaux T, Guerci P, et al. RISC-19-ICU Investigators. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine. 2020; 25, 100449.
[49] July J, Pranata R. Prevalence of dementia and its impact on mortality in patients with coronavirus disease 2019: A systematic review and meta-analysis. Geriatr Gerontol Int. 2021; 21 (2), 172-7.
[50] Becerra-Muñoz VM, Núñez-Gil IJ, Eid CM, et al. Clinical profile and predictors of in-hospital mortality among older patients admitted for COVID-19. Age Ageing. 2021; 50 (2), 326-34.