Le Infezioni in Medicina, n. 2, 199-208, 2021
REVIEWS
Human visceral leishmaniasis prevalence by different diagnostic methods in Latin America: a systematic review and meta-analysis
Estefanía Gutiérrez-Ocampo1, Rhuvi Villamizar-Peña1, Isabella Cortes-Bonilla1, Luisa M. García-Zuluaga1, Yeimer Holguin-Rivera1, Harrison D. Ospina-Arzuaga1, Maria Camila Cardona-Trujllo1, Adrián E. Trejos-Mendoza2, Soffia Perez-Vargas2, Kovy Arteaga-Livias3,4, Lysien I. Zambrano5, D. Katterine Bonilla-Aldana1,2, Luis A. Perez-Garcia6, Carlos E. Hernandez-Pereira6, Alfonso J. Rodriguez-Morales1,2,3,7,8, Alberto Paniz-Mondolfi6,9,10,11, Olinda M. Delgado12
1Grupo Colaborativo de Investigación en Enfermedades Transmitidas por vectores, Zoonóticas y tropicales de Risaralda, Pereira, Risaralda, Colombia;
2Semillero de Investigación en Zoonosis (SIZOO), Grupo de Investigación BIOECOS, Fundación Universitaria Autónoma de las Américas, Sede Pereira, Pereira, Risaralda, Colombia;
3Master in Clinical Epidemiology and Biostatistics, Universidad Cientifica del Sur, Lima, Peru;
4Faculty of Medicine, Universidad Nacional Hermilio Valdizán, Huánuco, Peru;
5Unit of Scientific Research, School of Medicine, Faculty of Medical Sciences, Universidad Nacional Autónoma de Honduras (UNAH), Tegucigalpa 11101, Honduras;
6Instituto de Investigaciones Biomédicas IDB/Incubadora Venezolana de la Ciencia, Cabudare, Edo. Lara, Venezuela;
7Grupo de Investigación Biomedicina, Faculty of Medicine, Fundación Universitaria Autónoma de las Américas, Pereira, Risaralda, Colombia;
8Universidad Privada Franz Tamayo (UNIFRANZ), Cochabamba, Bolivia;
9Laboratory of Medical Microbiology, Department of Pathology, Molecular and Cell-based Medicine, The Mount Sinai Hospital-Icahn School of Medicine at Mount Sinai, New York, USA;
10Laboratorio de Señalización Celular y Bioquímica de Parásitos, Instituto de Estudios Avanzados (IDEA), Caracas, Caracas, Venezuela;
11Academia Nacional de Medicina, Caracas, Venezuela;
12Immunoparasitology Section, Tropical Medicine Institute, Universidad Central de Venezuela, Caracas, Venezuela
Corresponding author
Alfonso Rodriguez-Morales
E-mail: alfonso.rodriguez@uam.edu.co
arodriguezmo@cientifica.edu.pe
SummaRY
Visceral leishmaniasis is a neglected zoonotic disease that affects animals and humans in different tropical and subtropical regions and even beyond, with variable prevalence among infected hosts. To date, there have been no systematic reviews on human visceral leishmaniasis prevalence in Latin America. We therefore performed a systematic literature review with meta-analysis, using six databases to assess prevalence of visceral leishmaniasis in human patients in Latin American countries. Observational studies were included but analyzed separately. We performed a random-effects model meta-analysis to calculate the pooled prevalence and 95% confidence interval (95%CI). In all, 10,435 articles were retrieved for the time frame (1950-2019). After initial screening, 120 articles were selected for full-text assessment, 97 being finally included for qualitative and quantitative analyses. Overall, VL pooled prevalence was estimated at 38.8% (95% CI 33.8-43.8%), derived from 97 studies, including 44,986 individuals. Many aspects of the transmission dynamics of Leishmania and the exact burden of this parasitosis on public health remain largely unknown. Although the elimination of zoonotic VL in the Americas appears an unrealistic goal, additional efforts need to be put in place to achieve better diagnosis, treatment, and prevention of VL.
Keywords: Visceral leishmaniasis, Leishmania, prevalence, epidemiology, Latin America.
INTRODUCTION
The leishmaniases are a group of cutaneous and visceral vector-borne diseases caused by intracellular protozoan parasites of the genus Leishmania, which comprises two subgenera: Leishmania and Viannia [1, 2]. The infecting Leishmania species determine clinical manifestations, treatment and prognosis. Visceral Leishmaniasis (VL), also known as “kala azar” (black fever in Hindi), is the most devastating form of the disease, with a high Case Fatality Rate (CFR), and the median of 7% of cases with a fatal outcome, although higher in different series [3]. The main etiological agents of VL are L. donovani and L. infantum (syn. Leishmania chagasi in Latin America). Both transmitted through female hematophagous sandflies of the Phlebotomus genus in the Old World and Lutzomyia in the New World [4-6]. Every year, approximately 2 million new cases of leishmaniases are reported worldwide, with VL accounting for more than 500,000, mainly located in developing countries, and resulting in 50,000 deaths per year [7, 8].
In the Americas, VL is endemic in 12 countries, with 59,769 new cases reported from 2001 to 2017, with an average of 3,516 cases per year. About 96% (57,582) reported Brazilian cases, but other South American countries, such as Argentina, Colombia, Paraguay, and Venezuela, have also contributed a significant number of annual cases [9-12]. In 2017, VL incidence rates in the Americas were estimated at 5.23 cases per 100,000 inhabitants in high-risk areas for transmission, which was higher than reports from previous years. In 2018, 3,562 new VL cases were reported for an incidence rate of 4.80, which, compared to 2017, represented a significant decrease of about 16%. This reduction only occurred in Brazil, Colombia, Argentina and Paraguay. However, in El Salvador, Guatemala and Venezuela, VL cases continued to rise [13].
Some factors associated with the increase of VL cases in endemic areas include internal (nationwide) displacement, forced migration of susceptible hosts into endemic areas, and disturbance of sandfly habitats (e.g. deforestation, climate change) [14-18].
VL caused by L. infantum is considered a zoonosis with domestic dogs as the primary reservoirs. However, VL has been reported in wild animals such as marsupials, primates, edentates, lagomorphs, bats, rodents, horses, and foxes. These synanthropic animals can be located in endemic areas, representing a risk factor for transmission to humans. On the other hand, VL due to L. donovani displays exclusive circulation among humans with anthroponotic vectorial transmission along with persistent and abundant parasitemia [7-9, 19].
The prevalence of VL in Latin America shows significant variations among countries. To the best of our knowledge, no other systemic reviews or meta-analysis have been published on this topic to date. The objectives of this study were to estimate pooled prevalence of VL in human patients from Latin America based on available public health reports and observational studies, and to determine differences in VL prevalence between countries, age groups, patient sex, and diagnostic methods.
METHODS
Protocol and registration
The protocol of the study followed the recommendations established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [20].
Eligibility criteria
Published peer-reviewed articles that reported cases with confirmed laboratory diagnosis of VL were included. Diagnostic methods included ELISA, IIF/IFAT, PCR, bone marrow cytology, spleen aspiration cytology, rK39-based rapid tests, Montenegro test, Western blot, and parasite culture. Article language limit was not set, and publications from January 1st, 1950 to December 31st, 2019 were included. Reviews, opinion articles, and letters not offering original data and studies reporting cases with incomplete information were excluded.
Information sources and search strategy
We conducted a systematic review using Medline/PubMed, Scopus, and Web of Science. The search terms used included: “visceral leishmaniasis,” “leishmaniasis”, “Leishmania infantum”, “Leishmania chagasi”, “Latin America,” “South America,” and “kala-azar”. The searches ended by December 31st, 2019. Four different researchers independently evaluated the search results.
Study selection
Initial search strategy results were screened by title and abstract. The full texts of relevant articles were examined for inclusion and exclusion criteria (Figure 1). When an article reported the same information from the same patient, the reports were combined to obtain complete data and counted as a single case. Observational studies that reported the proportion of infected patients using different diagnostic methods were included for quantitative synthesis (meta-analysis).
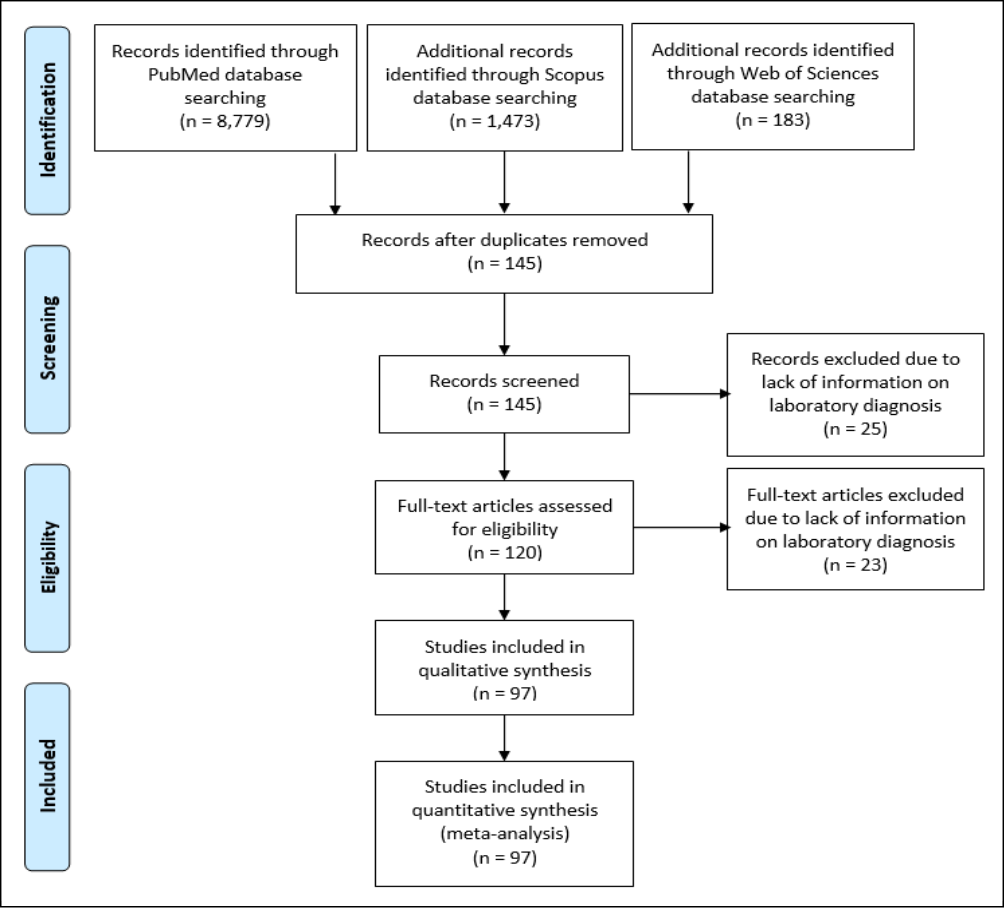
Figure 1 - Study selection and characteristics.
Data collection process and data items
Data extraction forms, including information on the type of publication, publishing institution, country, year, date of publication, number of reported cases, age, sex, and diagnostic method, were filled independently by four researchers. A fifth investigator checked the article list and data extractions to guarantee duplicate articles or duplicate information and resolved discrepancies in study inclusion.
Assessment of methodological quality and risk of bias
We used the critical appraisal tool of the Quality Appraisal of Case Series Studies Checklist of the IHE to assess the quality of cross-sectional studies (AXIS) [21, 22]. Publication bias was assessed using a funnel-plot. A random-effects model was used to calculate the pooled prevalence and 95% CI given variable degrees of data heterogeneity and given the inherent heterogeneity in any systematic review of studies from the published literature. Egger’s test for publication bias was also performed.
Statistical approach
Unit discordance for variables was resolved by converting all units to a standard measurement for each variable. Percentages and means ± Standard Deviation (SDs) were calculated to describe the distributions of categorical and continuous variables, respectively. Since individual information was not available for all patients, we report weighted means and SDs. The baseline data were analyzed using the Stata version 14.0, licensed for Universidad Tecnológica de Pereira in Colombia.
The meta-analyses were performed using Stata, and the software OpenMeta [Analyst] [23], JASP (Version 0.12.2)®, and Comprehensive Meta-Analysis ve.3.3® licensed for Universidad Tecnológica de Pereira. Pooled prevalences and their 95% confidence intervals (95% CIs) were used to summarize the weighted effect size for each study grouping variable using a binary random-effects model (which takes into consideration sample sizes of individual studies), except for median age, where a continuous random-effect model was applied (DerSimonian-Laird procedure) [24, 25].
Measures of heterogeneity, including Cochran’s Q statistic, I2 index, and tau-squared test, were estimated and reported. We performed subgroup analyses by age groups (adults or children) and meta-analyses for each interest variable. Publication bias was assessed using a funnel-plot.
A supplemental table with the main characteristics of included studies is available upon request.
RESULTS
Study selection and characteristics
A total of 10,435 articles were retrieved using the search strategy. After screening by abstract and title, 120 articles were selected for full-text assessment. Of these, 23 were excluded due to the lack of information on laboratory diagnosis, and 97 were finally included for final qualitative synthesis and meta-analysis (Figure 1).
Our review included 97 studies that were published between January 1st, 1950 until December 31st, 2019, most of them from Brazil (69.3%), Venezuela (11.4%), Colombia (6.8%), Argentina (3.4%), and Honduras (3.4%) (Table S1), including a total of 44,986 individuals assessed by ELISA (19,124), IFI/IFAT (19,761), PCR (3,960), bone marrow cytology (4,584), spleen aspiration cytology (471), rapid tests based on rK39 antigen (3,172), Montenegro test (11,425), Western blot (1,110), and parasite culture (942). All the studies were cross-sectional (Table S1). We analyzed 14 variables for the meta-analyses (Table 1).
Publication bias was assessed with a funnel plot for standard error, with no evidence of bias (Figure 2), but the Egger test suggested possible publication bias (z=0.330; p<0.001). Kendall’s tau test was 0.087 (p=0.207).
Table 1 - Meta-analysis outcomes (random-effects model)*.
|
Technique, countries |
Number of Studies* |
Pool Prevalence (%) |
95%CI |
n |
Q† |
I2 ‡ |
t2 § |
p |
|
All |
97 |
38.8 |
33.8-43.8 |
44,986 |
59,165.025 |
99.838 |
0.063 |
<0.001 |
|
Year 2019 |
4 |
62.6 |
20.80-100.0 |
488 |
440.246 |
99.32 |
0.180 |
<0.001 |
|
Year 2013 |
11 |
55.1 |
33.10-77.00 |
3,049 |
2,657.728 |
99.62 |
0.137 |
<0.001 |
|
Central America and Mexico |
6 |
41.1 |
9.8-72.3 |
1,299 |
1,286.931 |
99.61 |
0.151 |
<0.001 |
|
South America |
61 |
38.7 |
33.5-43.8 |
43,687 |
57,431.025 |
99.84 |
0.062 |
<0.001 |
|
Brazil |
67 |
43.8 |
36.3-51.2 |
36,326 |
44,968.162 |
99.853 |
0.096 |
<0.001 |
|
Bone marrow aspirate cytology |
27 |
63.0 |
46.8-79.2 |
4,584 |
8,284.411 |
99.686 |
0.179 |
<0.001 |
|
Spleen aspirate cytology |
6 |
45.5 |
18.0-73.0 |
471 |
319.118 |
98.433 |
0.107 |
<0.001 |
|
ELISA |
39 |
20.8 |
17.5-24.1 |
19,124 |
3,114.855 |
98.78 |
0.010 |
<0.001 |
|
IFI/IFAT |
46 |
27.6 |
23.5-31.7 |
19,761 |
12,699.444 |
99.646 |
0.018 |
<0.001 |
|
rK39 ICT |
16 |
27.0 |
13.8-40.2 |
3,172 |
4,925.296 |
99.695 |
0.071 |
<0.001 |
|
LST/IDR or Montenegro test |
19 |
39.1 |
24.7-53.5 |
11,425 |
14,206.003 |
99.873 |
0.102 |
<0.001 |
|
NNN culture |
6 |
45.4 |
18.5-72.4 |
942 |
435.432 |
98.852 |
0.110 |
<0.001 |
|
PCR |
15 |
40.2 |
26.7-53.7 |
3,960 |
2,921.752 |
99.521 |
0.069 |
<0.001 |
* 95% CI = 95% confidence interval. † Cochran’s Q statistic for heterogeneity. ‡ I2 index for the degree of heterogeneity. § Tau-squared measure of heterogeneity. ELISA, enzyme-linked immunosorbent assay; IFI, Indirect Immunofluorescence; IFAT, immunofluorescence antibody test; PCR, polymerase chain reaction; rK39 ICT, immunochromatography with the recombinant kinetoplastid 39 antigen; LST, leishmaniasis skin test; IDR, intradermal reaction; NNN, Novy-MacNeal-Nicolle medium. *Some studies assessed simultaneous variables. Multiple studies assessed the prevalence by different methods.
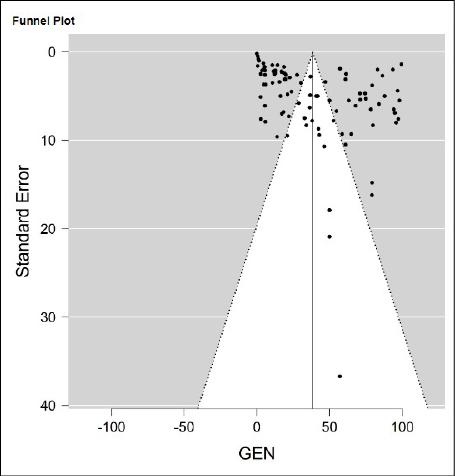
Figure 2 - Funnel-plot for the Standard Error to assess for publication bias.
Individual study characteristics
The median number of individuals per study was 299, with positive rates ranging from 0.1 to 99.5% (Table 1).
Regardless of the diagnostic technique used, the pooled prevalence for VL was 38.8% (95%CI 33.8-43.8%), derived from 97 studies, including 44,986 individuals (Table 1) (Figure 3).
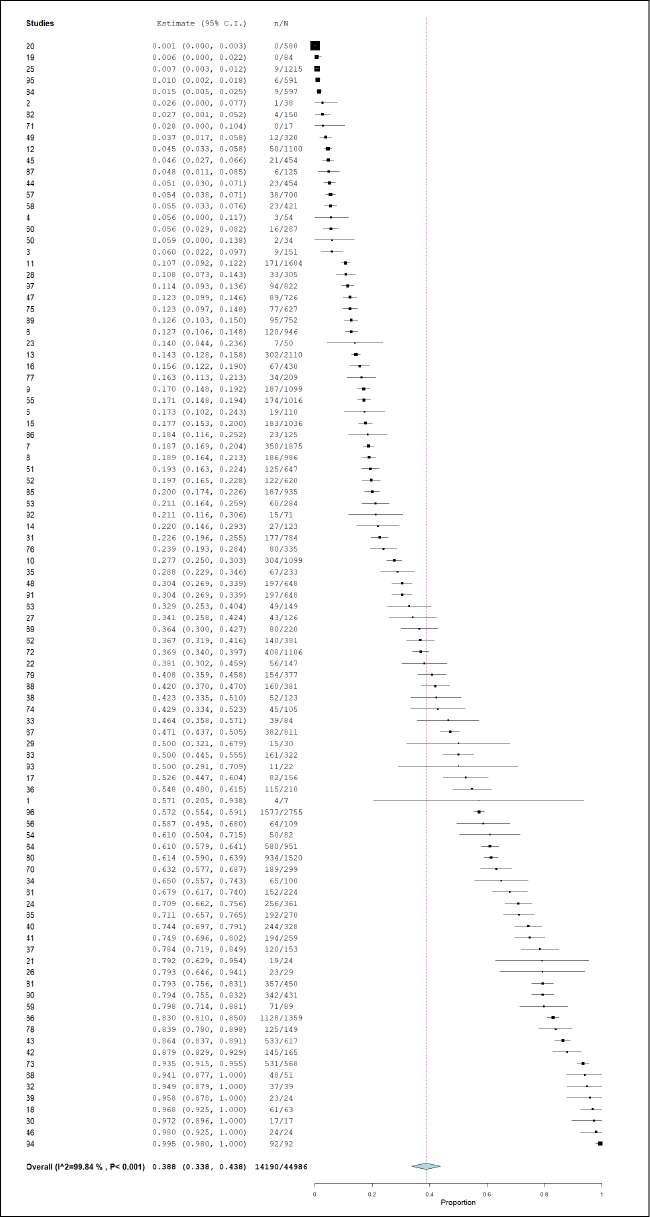
Figure 3 - Pool prevalence forest plot of VL by any diagnostic technique.
Microscopic findings
Regarding bone marrow aspirate cytology, the pooled prevalence for VL was 63.0% (95%CI 46.8-79.2%), derived from 27 studies including 4,584 individuals (Table 1); and in the case of spleen aspirate cytology, with six studies and 471 individuals, the pooled prevalence was estimated at 45.5% (95%CI 18.0-73.0%) (Table 1, Figure 4). By this technique, 2,623 cases were diagnosed.
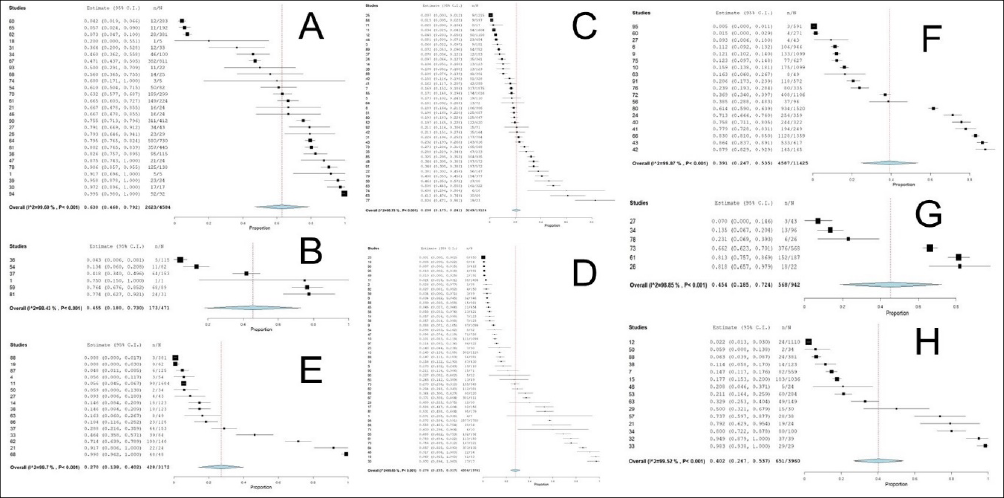
Figure 4 - Pool prevalence forest plot of VL by diagnostic technique. A. Bone marrow aspirate cytology. B. Spleen aspirate cytology. C. ELISA. D. IFI/IFAT. E. rK39 ICT. F. LST/IDR or Montenegro test. G. NNN culture. H. PCR.
Serological or antigenic findings
For enzyme-linked immunosorbent assay (ELISA), VL pooled prevalence derived from 39 studies, including 19,124 individuals, was 20.8% (95%CI 17.5-24.1%) (Table 1, Figure 4). By this technique, 3,249 cases were diagnosed. In the case of IFI/IFAT, with 46 studies and 19,761 individuals, it was 27.6% (95%CI 23.5-31.7%) (Table 1, Figure 4). By this technique, 4,356 cases were diagnosed. For rK39 ICT, with 16 studies including 3,172 individuals, pooled prevalence was 27.0% (95%CI 13.8-40.2%) (Table 1, Figure 4). By this technique, 428 cases were diagnosed. And for LST/IDR or Montenegro test, with 19 studies including 11,425 individuals, it was 39.1% (95%CI 24.7-53.5%) (Table 1, Figure 4). By this technique, 4,587 cases were diagnosed.
Parasite culture
For parasite culture in Novy-MacNeal-Nicolle (NNN) medium, the estimated pooled prevalence derived from 6 studies, including 942 individuals, was 45.4% (95%CI 18.5-72.4%) (Table 1, Figure 4). By this technique, 568 cases were diagnosed.
Molecular techniques
For Polymerase Chain Reaction (PCR), the pool prevalence for VL from 15 studies and 3,960 individuals was 40.2% (95%CI 26.7-53.7%) (Table 1, Figure 4). By this technique, 651 cases were diagnosed.
Comparing the main findings by year, studies from 2019 yielded the highest value, for a pooled prevalence of 62.6% (95%CI 20.80-100.0%), followed by 2013 with 55.1% (95%CI 33.10-77.00%) (Table 1, Figure 5). Comparing sub-regions, Central America and Mexico yielded 41.1% (95%CI 9.8-72.3%) and South America 38.7% (95%CI 33.5-43.8%) (Table 1, Figure 5). Brazil, with 67 studies and 36,326 individuals, yielded a pooled prevalence of 43.8% (95%CI 36.3-51.2%) (Table 1, Figure 5).
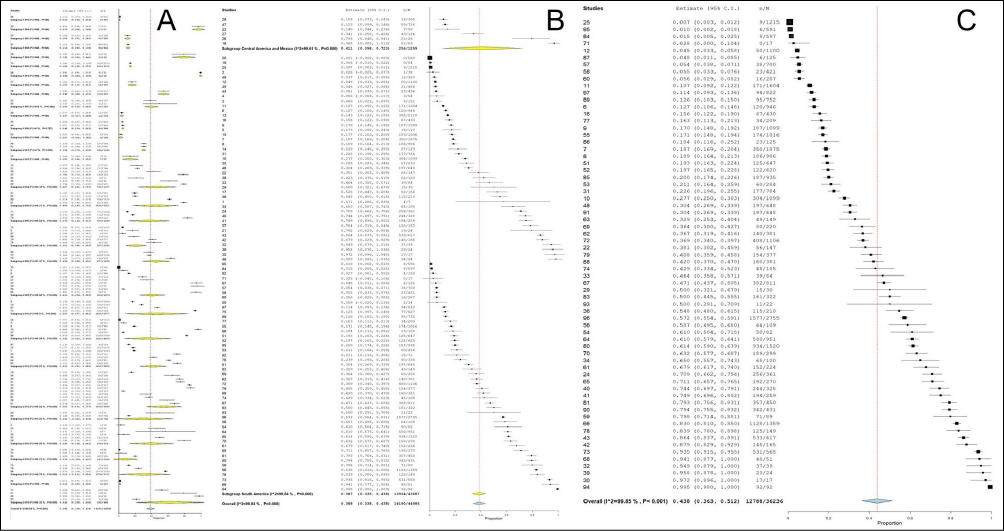
Figure 5 - Pool prevalence forest plot of VL by variables. A. Year. B. Subregions. C. Brazil.
DISCUSSION
Visceral leishmaniasis due to different infecting Leishmania species shares similar clinical manifestations, including fever, weight loss, lymphadenopathy, hyperpigmentation, hepatosplenomegaly, and pancytopenia. In endemic areas, the proportion of asymptomatic infections is 5 to 10 times higher than symptomatic cases on immunocompetent hosts [6, 10, 19, 26, 27]. Additionally, VL has been recognized as a significant health threat to co-infected HIV/AIDS patients [28].
To achieve control over VL in the Americas, surveillance programs must be reinforced in endemic countries focusing heavily on detection, prevention and prompt treatment. One of the greatest challenges to overcome the LV is resource constrains, which prevent direct and indirect costs associated with wide-spread epidemiological programs. Poor health care in these low-income countries is also associated with increasing poverty, affecting the most vulnerable populations disproportionately [4, 12, 27, 29-32].
We estimated an overall pooled prevalence for VL at over 38%. As expected, Brazil provided most of the studies and individuals assessed; prevalence in this country was also high, with a pooled result of more than 43% [33-36]. That is consistent because Brazil has been responsible for more than 96% of VL cases in the region during 2012-2018 (23,545 out of 24,515 cases). In 2018, out of 3,562 reported cases in the region, 3,466 (97.3%) were from Brazil, representing an incidence rate of 5.05 cases per 100,000 inhabitants [9,12]. However, higher rates have been reported in Honduras, wherein 2018 incidence rates reached 8.35 cases per 100,000 inhabitants [12]. It is important to note that even though VL’s persistence and expansion have been reported in Colombia, Venezuela, and Brazil, it is still not regularly considered in the differential diagnosis of febrile syndromes and pediatric anaemia in endemic areas [37-46].
All diagnostic techniques yielded a VL pool prevalence higher than 20%, with bone marrow aspirate cytology displaying the highest (63%); coincidentally, bone marrow aspirate is still one of VL’s most common techniques diagnosis in humans and animals [47, 48]. Results were similar among serological tests, ranging from 20.8% (ELISA) to 39.1% (IDR), while PCR diagnosis yielded 40%.
Since early treatment is crucial for the appropriate clinical management of VL, molecular diagnostic techniques have become relevant due to their remarkable sensitivity, specificity, and possible application to various types of clinical samples [49]. Among them, real-time PCR (qPCR)-based approaches have become increasingly popular in recent years to detect, quantify, and identify Leishmania species; the latter is critical because serological techniques and NNN culture can only report parasite detection and quantification [49]. However, despite its efficacy, currently there is no a standardized qPCR-based method of VL diagnosis [49].
There is still much to understand about the transmission dynamics of Leishmania in human, canine and vector populations. The exact burden of this parasite on public health remains mostly unknown. However, the increasing trend of VL cases observed in Brazil and their spillover to previously unaffected areas raise doubts about the effectiveness of current control measures. Additionally, except for nutritional status in young children, severity determinants in human infection remain poorly understood [50]. Other immunocompromising conditions have also been a matter of concern, as is the case of HIV or cancer. In that way, VL and its growing importance as an opportunistic disease, particularly among populations of HIV individuals in some countries of Europe and Latin America, is of concern [51-53]. Despite the decreased incidence of Leishmania/HIV co-infections after the introduction of the high active antiretroviral therapy, the endemic areas for Leishmania spp. are characterized to overlap with those with a high prevalence of HIV, which means that the risk of developing VL is 100–2300 times greater in HIV infected people [51-53].
Limitations
There is significant heterogeneity of the prevalence studies available and published in Latin America. The selected works include cases of VL confirmed with heterogeneous diagnostic methodology on subjects included in the different studies about specific health structures belonging to particular population groups (immunosuppressed, blood donors) based on symptoms compatible with VL. The subjects on whom the parasitological diagnosis of VL have been carried out do not constitute a sample of the general reference population or special populations. Nevertheless, it reflects the prevalence in screened subjects of the 97 selected works of the region.
In conclusion, although the elimination of zoonotic VL in the Americas may be an unrealistic goal – given the lack of political commitment, gaps in scientific knowledge, and critical weaknesses in case management and surveillance systems –, additional efforts need to be put in place. Research priorities and current strategies should be reviewed to achieve better diagnosis, treatment, and prevention of VL.
Conflict of interest
None declared.
Funding
None.
REFERENCES
[1] Paniz-Mondolfi AE, Talhari C, Garcia Bustos MF, et al. American cutaneous leishmaniasis in infancy and childhood. Int J Dermatol. 2017; 56 (12), 1328-41.
[2] Perilla-Gonzalez Y, Gomez-Suta D, Delgado-Osorio N, et al. Study of the scientific production on Leishmaniasis in Latin America. Recent Pat Antiinfect Drug Discov. 2014; 9 (3), 216-22.
[3] Villamil-Gomez WE, Calderon-Gomezcaseres A, and Rodriguez-Morales AJ. Visceral Leishmaniasis in a patient with systemic lupus erythematosus from Colombia, Latin America. Infez Med. 2019; 27 (1), 106-8.
[4] Hailu T, Yimer M, Mulu W, and Abera B. Challenges in Visceral Leishmaniasis control and elimination in the developing countries: A Review. J Vector Borne Dis. 2016; 53 (3), 193-8.
[5] Idris M, Farid J, and Gul N. Morphology of bone marrow in Visceral Leishmaniasis. J Ayub Med Coll Abbottabad. 2018; 30 (3), 342-4.
[6] Saporito L, Giammanco GM, De Grazia S, and Colomba C. Visceral Leishmaniasis: host-parasite interactions and clinical presentation in the immunocompetent and in the immunocompromised host. Int J Infect Dis. 2013; 17 (8), e572-6.
[7] Alvar J, Velez ID, Bern C, et al. Leishmaniasis worldwide and global estimates of its incidence. PLoS One. 2012; 7 (5), e35671.
[8] Burza S, Croft SL, and Boelaert M. Leishmaniasis. Lancet. 2018; 392 (10151), 951-70.
[9] WHO. Leishmaniasis: Magnitude of the Problem. 2014.
[10] Brodskyn CI, and Kamhawi S. Biomarkers for zoonotic visceral leishmaniasis in Latin America. Front Cell Infect Microbiol 2018; 8, 245.
[11] Sunyoto T, Potet J, and Boelaert M. Visceral Leishmaniasis in Somalia: a review of epidemiology and access to care. PLoS Negl Trop Dis. 2017; 11 (3), e0005231.
[12] Organization PAH. Leishmaniasis: Epidemiological Report in the Americas. 2019.
[13] Pan American Health Organization. “Leishmaniasis: Epidemiological Report in the Americas.” Washington D.C.: PAHO, 2019.
[14] Cardenas R, Sandoval CM, Rodriguez-Morales AJ, et al. Epidemiology of American tegumentary Leishmaniasis in domestic dogs in an endemic zone of Western Venezuela. Bull Soc Pathol Exot 2006; 99 (5), 355-8.
[15] Cardenas R, Sandoval CM, Rodriguez-Morales AJ, and Franco-Paredes C. Impact of climate variability in the occurrence of Leishmaniasis in Northeastern Colombia. Am J Trop Med Hyg. 2006; 75 (2), 273-7.
[16] Delgado O, Silva S, Coraspe V, et al. Cutaneous Leishmaniasis imported from Colombia to Northcentral Venezuela: implications for travel advice. Travel Med Infect Dis. 2008; 6 (6), 376-9.
[17] Rodriguez-Morales AJ, Pascual-Gonzalez Y, Benitez JA, et al. Association between Cutaneous Leishmaniasis Incidence and the human development index and its components in four endemic states of Venezuela. Rev Peru Med Exp Salud Publica. 2010; 27 (1), 22-30.
[18] Bonilla-Aldana DK, Suarez JA, Franco-Paredes C, et al. Brazil Burning! What Is the potential impact of the amazon wildfires on vector-borne and zoonotic emerging diseases? - a Statement from an International Experts Meeting. Travel Med Infect Dis. 2019; 31, 101474.
[19] Antinori S, Schifanella L, and Corbellino M. Leishmaniasis: new insights from an old and neglected disease. Eur J Clin Microbiol Infect Dis. 2012; 31 (2), 109-18.
[20] Moher D, Liberati A, Tetzlaff J, Altman DG, and Group P. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. PLoS Med. 2009; 6 (7), e1000097.
[21] Institute of Health Economics (IHE). “Quality appraisal of case series studies checklist.” Institute of Health Economics, http://www.ihe.ca/research-programs/rmd/cssqac/cssqac-about.
[22] Downes MJ, Brennan ML, Williams HC, and Dean RS. Development of a Critical Appraisal Tool to Assess the Quality of Cross-Sectional Studies (Axis). BMJ Open. 2016; 6 (12), e011458.
[23] Wallace BC, Dahabreh IJ, Trikalinos TA, Lau J, Trow P, and Schmid CH. Closing the gap between methodologists and end-users: R as a computational back-end. J Stat Softw. 2012; 49 (5), 1-15.
[24] Viechtbauer W. Conducting Meta-Analyses in R with the Metafor Package. J Stat Soft. 2010; doi:10.18637/jss.v036.i03
[25] Kontopantelis E, and Reeves D. Performance of statistical methods for meta-analysis when true study effects are non-normally distributed: a comparison between dersimonian-laird and restricted maximum likelihood. Stat Methods Med Res. 2012; 21 (6), 657-9.
[26] Souza TD, Turchetti AP, Fujiwara RT, Paixao TA, and Santos RL. Visceral Leishmaniasis in zoo and wildlife. Vet Parasitol. 2014; 200 (3-4), 233-41.
[27] Tabbabi A. Review of Leishmaniasis in the Middle East and North Africa. Afr Health Sci. 2019; 19 (1), 1329-37.
[28] Lindoso JAL, Moreira CHV, Cunha MA, and Queiroz IT. Visceral Leishmaniasis and Hiv coinfection: current perspectives. HIV AIDS (Auckl). 2018; 10, 193-201.
[29] Chappuis F, Sundar S, Hailu A, et al. Visceral Leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol. 2007; 5 (11), 873-82.
[30] Girone G, Mateo C, Gaya V, et al. Admissions for imported and non-imported parasitic diseases at a general hospital in spain: a retrospective analysis. Travel Med Infect Dis. 2015; 13 (4), 322-8.
[31] Dantas-Torres F, and Brandao-Filho SP. Visceral Leishmaniasis in Brazil: revisiting paradigms of epidemiology and control. Rev Inst Med Trop Sao Paulo. 2006; 48 (3), 151-6.
[32] van Griensven J, and Diro E. Visceral Leishmaniasis. Infect Dis Clin North Am. 2012; 26 (2), 309-22.
[33] Crescente JA, Silveira FT, Lainson R, Gomes CM, Laurenti MD, and Corbett CE. A Cross-Sectional study on the clinical and immunological spectrum of human Leishmania (L.) Infantum Chagasi infection in the Brazilian Amazon region. Trans R Soc Trop Med Hyg. 2009; 103 (12), 1250-6.
[34] dos Santos Marques LH, Gomes LI, da Rocha IC, et al. Low parasite load estimated by Qpcr in a cohort of children living in urban area endemic for Visceral Leishmaniasis in Brazil. PLoS Negl Trop Dis. 2012; 6 (12), e1955.
[35] Felipe IM, Aquino DM, Kuppinger O, et al. Leishmania Infection in humans, dogs and sandflies in a Visceral Leishmaniasis endemic area in Maranhao, Brazil. Mem Inst Oswaldo Cruz. 2011; 106 (2), 207-11.
[36] Franca Ade O, de Castro VL, Lima MS, Jr., Pontes ER, and Dorval ME. Anti-Leishmania Antibodies in blood donors from the midwest region of Brazil. Transfus Apher Sci. 2013; 49 (3), 627-30.
[37] Arbelaez N, Moreno J, Murillo J, et al. First report of an urban case of canine Visceral Leishmaniasis in the municipality of Cali, Colombia. Am J Trop Med Hyg. 2020; 102 (2), 289-93.
[38] Lyra MR, Pimentel MI, Madeira Mde F, et al. First Report of cutaneous Leishmaniasis Caused by Leishmania (Leishmania) Infantum Chagasi in an urban area of Rio De Janeiro, Brazil. Rev Inst Med Trop Sao Paulo. 2015; 57 (5), 451-4.
[39] Silva GA, Boechat Tde O, Ferry FR, et al. First case of autochthonous human Visceral Leishmaniasis in the urban center of Rio De Janeiro: Case Report. Rev Inst Med Trop Sao Paulo. 2014; 56 (1), 81-4.
[40] González-Colonia LV, Bonilla-Aldana DK, Álvarez-Serrano MP, Granados-Hincapie LY, Pinilla-Ticora LC, and Rodríguez-Morales AJ. An urban case of canine visceral leishmaniasis in the municipality of Pereira, Colombia. World Vet J. 2021; 11 (1), 115-8.
[41] Brustoloni YM, Cunha RV, Dorval ME, et al. Comparison of conventional methods for diagnosis of Visceral Leishmaniasis in children of the Center-West region of Brazil. Braz J Infect Dis. 2007; 11 (1), 106-9.
[42] Brustoloni YM, Lima RB, da Cunha RV, et al. Sensitivity and Specificity of Polymerase Chain Reaction in Giemsa-Stained Slides for Diagnosis of Visceral Leishmaniasis in Children. Mem Inst Oswaldo Cruz. 2007; 102 (4), 497-500.
[43] Burnatseva VV. On the diagnosis of visceral leishmaniasis in children. Pediatriia. 1960; 38, 74-6.
[44] Cascio A, Calattini S, Colomba C, et al. Polymerase Chain Reaction in the diagnosis and prognosis of mediterranean visceral leishmaniasis in immunocompetent children. Pediatrics. 2002; 109 (2), E27.
[45] Fraga TL, Brustoloni YM, Lima RB, et al. Polymerase chain reaction of peripheral blood as a tool for the diagnosis of visceral leishmaniasis in children. Mem Inst Oswaldo Cruz. 2010; 105 (3), 310-3.
[46] Mironova VG, Plakhuta TG, Soskov GI, and Petrov V. The characteristics of the course and diagnosis of visceral leishmaniasis in children. Klin Lab Diagn. 1999; (8), 38-9.
[47] Chandra H, Chandra S, and Kaushik RM. Visceral Leishmaniasis with associated common, uncommon, and atypical morphological features on bone marrow aspirate cytology in nonendemic region. J Trop Med. 2013; 2013, 861032.
[48] Pamnani R, Rajab JA, Githang’a J, and Kasmani R. Disseminated histoplasmosis diagnosed on bone marrow aspirate cytology: report of four cases. East Afr Med J. 2009; 86 (12 Suppl), S102-5.
[49] Galluzzi L, Ceccarelli M, Diotallevi A, Menotta M, and Magnani M. Real-Time Pcr applications for diagnosis of Leishmaniasis. Parasit Vectors. 2018; 11 (1), 273.
[50] Romero GA, and Boelaert M. Control of Visceral Leishmaniasis in Latin America-a systematic review. PLoS Negl Trop Dis. 2010; 4 (1), e584.
[51] Pagliano P, Carannante N, Gramiccia M, et al. Visceral Leishmaniasis causes fever and decompensation in patients with cirrhosis. Gut. 2007; 56 (6), 893-4.
[52] Pagliano P, Ascione T, Di Flumeri G, Boccia G, and De Caro F. Visceral Leishmaniasis in immunocompromised: diagnostic and therapeutic approach and evaluation of the recently released IDSA guidelines. Infez Med. 2016; 24 (4), 265-71.
[53] Pagliano P, and Esposito S. Visceral Leishmaniosis in immunocompromised host: an update and literature review. J Chemother. 2017; 29 (5), 261-6.