Le Infezioni in Medicina, n. 2, 191-198, 2021
REVIEWS
Clinical and epidemiological aspects of sporotrichosis: an overview of the cases reported in Europe and in Italy
Rosa Monno1, Giorgia Giannelli2, Luciana Fumarola1
1Department of Basic Medical Science, Neuroscience and Sense Organs, University of Bari “Aldo Moro”, Bari, Italy;
2U.O.C. Radiodiagnostica, San Paolo Hospital, Bari, Italy
Corresponding author
Rosa Monno
E-mail: rosa.monno@uniba.it
SummaRY
Sporotrichosis is a fungal infection occurring worldwide, especially in tropical and sub-tropical areas. We present a brief review of clinical and epidemiological aspects of sporotrichosis, as well as its treatment. Sporotrichosis is rarely reported in Europe and the European Centre of Disease Control does not track its infection rate. To fill this gap, we report a survey of clinical cases described over the past forty years in Europe and in Italy.
Keywords: Sporotrichosis, lymphocutaneous lesions, voriconazole, Sporothrix epidemiology.
INTRODUCTION
The genus Sporothrix comprises over 50 fungal species of which only four (S. schenckii, S. brasiliensis, S. globosa and S. luriei) are pathogenic and have been recently grouped in a distinct “pathogenic clade”. There is the possibility that environmental species could lead, under certain conditions, to clinical forms. However, remarkable differences in the epidemiology, antifungal susceptibility, genetics and pathogenicity exist for the members of this pathogenic clade [1, 2-4]. They are able to cause infections in humans and in a variety of other vertebrates including horses, dogs, birds, pigs, cats and armadillos [5-7]. These fungi exhibit a temperature-dependent dimorphic switch and therefore are able to convert between two different morphologies (mould and yeast) in response to thermal stimuli. In the environment, or in vitro at 25°C, they grow as septate hyphae producing conidia whereas in the host or at 37°C they can convert into pathogenic yeasts causing sporotrichosis [8]. Among the members of the pathogenic clade, Sporothrix schenckii, now named the S. schenckii species complex, is the most common cause of human sporotrichosis which generally occurs after traumatic acquisition of the fungus from the environment. In fact, S. schenckii can easily be isolated from soil and plant matter such as straw, wood, Sphagnum moss, thorny plants and rose bushes. In humans, the disease is also known as “rose-gardener’s disease”, and has a worldwide distribution even if the majority of cases are reported from tropical and subtropical regions of the Americas [9-11].
Although S. schenckii has a worldwide distribution and it is ubiquitous in nature, most of the sporotrichosis cases are reported from Mexico, South Africa and North and South American countries [9]. In contrast, S. brasiliensis, and S. globosa appear restricted to specific geographical areas such as Brazil and East Asia, respectively, where the incidence of these species is exceptionally high [3, 4]. However, although S. schenckii is not the most pathogenic species of the group, it causes disease in a wide variety of warm-blooded animals including cats, dogs, armadillos, birds and parrots. It has also been isolated from fishes and dolphins [9, 12].
Sporotrichosis is acquired after a traumatic implantation of conidia from an environmental source. Sporothrix, the fungus that causes sporotrichosis most commonly enters the body through minor trauma that compromises the skin barrier. Infection through inhalation of conidia has been described in the case of pulmonary sporotrichosis [13]. Depending on the exposure, the disease can affect anyone regardless age or gender. Sporotrichosis has been regarded as an occupational disease because is most prevalent among people who handle soil or plant materials, such as gardeners, farmers, florists, mineworkers, carpenters and forestry workers. In addition, vocational exposure to the reservoir of this fungus, such as working in tree nurseries or handling hay-bales, represents a risk factor for this infection. Recently only sporadic (autochthonous or not) cases of sporotrichosis have been described such as those in returning travellers, aid workers, archaeologists and human immigrants [11].
Interestingly there is the possibility that sporotrichosis could be also considered a zoonosis. In fact, cases of sporotrichosis have been described in 83% of patients reporting to have contact with cats or being bitten or scratched by an infected cat on the skin, nose or oral cavities [14, 15].
CLINICAL ASPECTS, DIAGNOSIS AND TREATMENT
Sporotrichosis in humans can be classified in four different clinical forms: lymphocutaneous, fixed cutaneous, disseminated cutaneous, and extra-cutaneous with the first two being the most common clinical presentation. Cutaneous sporotrichosis is observed both in immunocompetent and immunocompromised subjects [16].
Cutaneous presentation is the most common clinical manifestation ranging from a fixed presentation characterized by a painless nodular lesion to lymphangitic form with ulcerated nodules in a linear distribution along the limbs (Figure 1). Unusual presentation of disseminated cutaneous sporotrichosis on the face and limbs in an immunocompetent patient has been also described [17].

Figure 1 - Lymphocutaneous sporotrichosis: purplish and ulcerated nodular lesions on the right hand and forearm.
The extracutaneous manifestation may involve bones, joints with periostitis, central nervous system and eye. Patients with advanced HIV infection or induced immunosuppression are at risk for these forms of sporotrichosis [16, 18]. The pulmonary manifestation is rare with cough and haemoptysis, resembling tuberculosis. In immunosuppressed patients (AIDS, diabetes, alcoholism, drug abusers) a systemic sporotrichosis has been described [16]. Disseminated sporotrichosis in a 26-year-old male who underwent a liver transplant has also been described with S. schenckii being isolated from the cerebrospinal fluid and ascites [19]. Chronic sporotrichosis injury may have caused the development of an epidermoid carcinoma as a late complication on a sporotrichosis scar of long evolution [20].
In the case of lymphocutaneous lesions, a differential diagnosis with nocardiosis, leishmaniasis and non-tuberculous mycobacteria infection, such as those caused by Mycobacterium marinum, must be carried out [11]. In Apulia, southern Italy, fifteen cases of nodular sporotrichoid clinical patterns due to M. marinum have been described [21]. Fungi such as Cryptococcus neoformans are also present in this area and may be responsible for infection characterized by nodular lesions resembling nodular lymphangitis and must be differentiated from those caused by other fungi. Other non-infectious causes could be represented by sarcoidosis, erythema nodosum, epithelioid sarcoma and metastatic nodular neoplastic lesions, which can also exhibit linearly arranged lesions [11]. The microbiological diagnosis is based on a direct examination of a clinical sample that shows the presence of typical ovoid or cigar shaped cells, though this direct examination is often disappointing because the microorganism is seldom abundant. Direct microscopy performed with potassium hydroxide preparations, whether or not in dimethyl sulfoxide, exhibits fungal elements. The material may be cultured on Sabouraud agar incubated at 30°C. The colonies are identified phenotypically by the membranous appearance of the surface which appear in a timescale of 5-7 days are cream or light to dark brown becoming black with age. Microscopic examination of the colonies showed the presence of delicate branching septate hyphae with short conidiophores surrounding pyriform conidia in a flower-like arrangement. The dimorphism of the Sporothrix schenckii is confirmed by reverting the mycelium-to-yeast form in Brain Heart Infusion medium, after incubation at 37ºC [22].
The histological section of the biopsy sample also shows the fungus that appears as characteristic cigar shaped forms of about 1-3 µm x 3-10 µm when Gomori-Grocott or PAS stains are used (Figure 2). It is extremely important that the examination of multiple (up to 20) sections may be required in order to detect the fungus. Hyperkeratosis, parakeratosis and a suppurative or granulomatous reaction can be observed. PCR that amplifies several genes such as chitin sintetase, β-tubuline and calmoduline and, most recently, sequence analysis allows the identification of the several species of Sporothrix [22, 23]. Matrix assisted laser desorption ionization time of flight mass spectrometry (MALDI-TOF MS) has also been used [24].
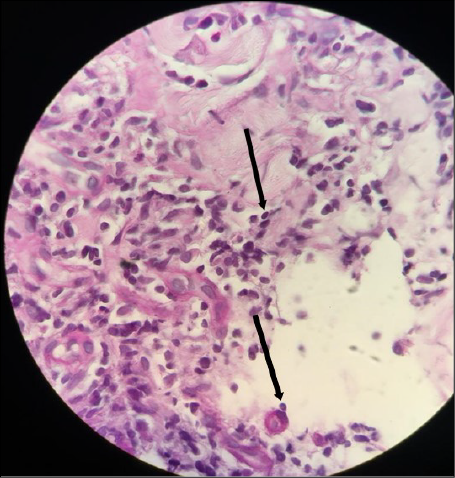
Figure 2 - Histopathology of lesion sample showing a granulomatous infiltrate with few yeast cells (arrow, H-E stain).
Immunoenzymatic tests like ELISA, Western Blot, latex agglutination have been suggested for cutaneous, systemic and atypical presentations of sporotrichosis or when no clinical lesions are observed. They may be useful for monitoring the disease progression and response to treatment [22]. At our knowledge this test are not commercially available in Italy.
Up to now, antifungal breakpoints have not been established for molds. Data on antimicrobial activity are quite different depending on the method used. By E-test, resistance to amphotericin B (MIC=8 mg/L) and susceptibility to itraconazole (MIC=0.5 mg/L) is reported by Wroblewska et al. [25]. The isolate was resistant to all other commonly used antifungal agents. The Clinical and Laboratory Standards Institute (CLSI) proposes a microdilution test for defining Minimum Inhibitory Concentration (MIC) value. By Micro Broth Dilution (MBD) method, MICs to amphotericin B were 8 mg/L and those to itraconazole 4 mg/L [26]. Five species of Sporothrix schenckii complex were tested by MBD. The antifungal drug most effective was amphotericin B (range 0.5-4 mg/L), ketoconazole (range 0.125-4 mg/L) and terbinafine (range 0.06-0.5 mg/L) [27]. By disk diffusion method, a susceptibility of S. globosa to ketoconazole and miconazole as well as a reduced susceptibility to fluconazole, itraconazole, voriconazole was reported [28]. Itraconazole, terbinafine, posaconazole, amphotericin B and voriconazole were effective against S. schenckii and S. globosa, while low efficacy with high MIC was shown with fluconazole [29].
Recently the species-specific Epidemiologic Cutoff Values (ECVs) were established, collecting strains of the different species of Sporothrix (301 for S. schenckii sensu stricto) from 17 laboratories around the world, Europe included. The proposed ECVs for S. schenckii were: amphotericin B 4 mg/L; itraconazole and posaconazole 2 mg/L; voriconazole 64 mg/L. Insufficient data about ECVs for ketoconazole and terbinafine were obtainable for S. schenckii though these ECVs could aid the clinician in identifying isolates less likely to respond to therapy [30].
Biofilm formation is an important virulence factor for pathogenic fungi. One of the defining characteristics of biofilms is their increased resistance to antimicrobial agents. In vitro studies have investigated the ability of several species of Sporothrix to form biofilm. S. schenckii, S. globosa and S. mexicana were strong biofilm producers and amphotericin B and caspofungin (50 x MIC) were the most effective against biofilm [31].
Some cases of sporotrichosis have been recently reported in Europe. In France, there was an autochthonous case of a 35-year-old man working in contact with soil who presented a cutaneous nodule on the right forefinger which had appeared six months previously. The clinical diagnosis was fixed cutaneous sporotrichosis due to S. schenckii and the patient recovered on oral itraconazole treatment [32]. A case of fixed sporotrichosis in a patient of Chinese origin was also diagnosed, and most recently another autochthonous case of sporotrichosis has been reported from Bordeaux in a 55-year-old man presenting with a nodular cutaneous lesion on the left forearm which appeared after a trauma with decaying vegetation [33]. The fungus was identified as S. globosa by MALDI-TOF and by sequencing, and was cured by itraconazole for 6 months [34]. In Corsica and Alsazia S. schenckii has been isolated from soil and stagnant water [35].
Sporotrichosis has been reported also from Spain with two cases originating in the province of Barcelona and eight of autochthonous cutaneous infection described in immunocompetent subjects in the province of Seville from 2006 to 2010 [36]. All the cases were observed in subjects with a previous trauma suffered during their work (gardeners, farmers) [37]. An autochthonous case of human sporotrichosis caused by S. globosa has also been reported in Lisbon, Portugal, in an immunocompetent patient who developed skin lesions in the right hand after a trauma occurred. The patient had never left Portugal. The fungus was susceptible to ketoconazole and miconazole and showed reduced susceptibility to other antifungal agents [28]. Similarly, another case of autochthonous cutaneous sporotrichosis in a 34 years old immunocompetent patient working at contact with soil caused by S. mexicana has been described in the same country. The patient presented with multiple polymorphous eruptions and ulcers on both feet. Subcutaneous nodules appeared in 2004 in Portugal after travelling in Malaysia one year previously where he had worn open footwear. The nodules had spontaneously healed, but a year later more severe lesions had appeared and become chronic. The fungus was isolated from the skin lesions and identified by molecular methods and sequenced as S. mexicana. The strains were susceptible to terbinafine [38].
Another case in a 71-year-old man of a gardening injury from a rose thorn with nodules appearing on the dorsal of the right hand is reported [39]. A case of imported lymphocutaneous sporotrichosis involving the right lateral region of the neck, has been described in Greece in a 22-year-old who had visited Columbia four months earlier, in order to work on a coffee plantation [40]. In Poland, a case of cutaneous sporotrichosis was detected in a woman immunosuppressed for mastectomy due to breast carcinoma and radiation and chemotherapy. The patient had no history of travel to an endemic area or of local trauma. Interestingly, by E-Test the fungus was susceptible only to itraconazole [25].
In Italy, fifty-eight cases of sporotrichosis have been described including 16 reported in Apulia, Southern Italy. The diagnosis was performed by direct microscopic examination and culture of material collected from the lesions [41]. The number of patients observed suggests an unexpectedly high incidence rate in Italy and Apulia.
A case was described in an 85 years old indigenous Italian man living in the town of Piacenza (Northern Italy). The patient stated he had never travelled outside of Italy. The diagnosis was relied only on histological studies where morphological forms and immunofluorescence test were suggestive for S. schenckii var. luriei. The nodule was surgically excised and sent to histology laboratory. Unfortunately, the patient developed fever (39°C) and died after two days [42].
Another case was described in an immunocompetent 64-year-old male Italian mason living in extreme Southern Italy (Vibo Valentia, Calabria). The affection had started four months previously as a pustular lesion on the right little finger after exposure to stagnant water mixed with senescent vegetation and soil. The lesion evolved into several nodules along the right upper extremity of the hand and in the upper right arm. Fever (38-39°C) was also present. S. schenckii was identified by morphological and cultural features and by PCR of the chitin synthase gene. The strains showed MICs of itraconazole and amphotericin B of 4 mg/L and 8 mg/L, respectively. A treatment with oral itraconazole and methylprednisolone was administered. A good improvement of the clinical picture was seen. After a few weeks later, the lymphadenopathy came back again and the therapy was intensified to increase methylprednisolone for one week while therapy with itraconazole was continued for another five weeks so obtaining a full recovery [26]. Lymphocutaneous sporotrichosis has also been reported in an 82-year-old man in Naples, Southern Italy, successfully treated with itraconazole [43].
A case of lymphocutaneous sporotrichosis in an 82-year-old man living in Naples, South Italy, involving the dorsum of his left hand and forearm was described. S. schenckii was isolated from skin biopsy, whereas the histological examination did not show yeast forms [44].
Sporotrichosis was reported in a 57-year-old male living in Catanzaro, Southern Italy, presenting with multiple nodular lesions arranged in a linear fashion along the left hand and forearm. The patient was affected by ankylosing spondylitis and since 2007 was under treatment with adalimumab therapy (40 mg every two weeks), a monoclonal antibody that binds to TNF-α inhibiting its interaction with TNF receptors. TNF-α exerts several effects on cellular and humoral immunity and plays a role in the host defence against various infectious agents. An unnoticed puncture was hypothesized by a rose thorn, as roses were grown in the patient’s home garden. The patient was treated with oral itraconazole (200 mg daily) and after three months an improvement was observed. After nine months, sequelae of the lesions were still present; risk factor was not detected but this case suggests that TNF-α antagonist might predispose subjects to fungal infections, including sporotrichosis [18]. A case of pulmonary sporotrichosis in a 37-year-old man HIV-positive presented with productive cough has been described. S. schenckii was isolated from sputum [45].
From 1991 to 2009, cutaneous sporotrichosis was diagnosed in 1 out of 774 renal transplants at the Careggi Hospital, Florence, Italy. The patient was treated with fluconazole with a good remission [46].
A case of lymphocutaneous sporotrichosis in a 29-year-old male agricultural labourer living in Calabria (Southern Italy) was described. Painful nodules started on the distal phalanx of his left thumb and extended to forearm. The lesion appeared after an accidental thorn bite in a hayloft. The infection was diagnosed by microscopic, cultural and histopathological pictures. Complete healing was obtained after a treatment with itraconazole (200 mg b.i.d.) for 7 consecutive days per month for 6 months [47].
In a previous report we have presented an autochthonous case of lymphocutaneous sporotrichosis caused by Sporothrix schenckii in a patient living in Apulia, Southern Italy. The patient developed skin lesions localized along the lymphatics, which appeared after he suffered an injury while collecting wicker canes in marshy water. The diagnosis of fungal infection was based on culture of the lesions; the fungus was identified as Sporothrix schenckii by MALDI-TOF and sequencing. Phylogenetic analysis was also performed. Low MIC values were detected for all tested echinocandins and azoles except for fluconazole (MIC=32 mg/L). The patient was treated with itraconazole without significant improvement after which therapy was changed to voriconazole and the lesions were seen to improve after 3 months of therapy. Our reported case represents the first documented report of lymphocutaneous sporotrichosis regressed by a voriconazole based therapy [48]. A summary of most recently reported cases of Sporothrix infection in Italy is showed in Table 1. In Italy, isolation and genetic characterization of S. schenckii isolated from commercial amended and garden soil have been also described. Sequencing and phylogenetic analysis performed on environmental and clinical isolates revealed a degree of difference sufficient to separate the isolates in environmental and clinical grounds [49].
Table 1 - Summary of most recently reported cases of Sporothrix infection in Italy.
|
Authors, year, (References) |
Country |
Gender |
Underlying condition |
Form |
Diagnosis |
History of trauma |
Treatment |
|
Alberici F. et al. 1989 (42) |
Piacenza, Italy |
M |
NA |
Cutaneous |
Histological picture |
Arised nodule on his lower right leg |
death |
|
Barile F. et al. 1993 (41) |
Bari, Southern Italy |
M 16 pt |
NA |
NA |
NA |
NA |
NA |
|
Gori S. et al. 1997 (45) |
Pisa, Italy |
M |
HIV positive |
Pulmonary |
Culture |
NR |
NA |
|
Baroni A. et al. 2007 (44) |
Naples, Southern Italy |
M |
Hypothyroidism |
Lymphocutaneous |
Histological picture and culture |
NA |
Itraconazole + methylpredni-solone |
|
Criseo G. et al. 2008 (26) |
Vibo Valentia, Southern Italy |
M |
NR |
Lymphocutaneous |
Culture, molecular identification, histological picture |
Injury exposed to stagnant water with vegetation |
Itraconazole + methylpredni-solone |
|
Caroti L. et al. 2010 (46) |
Florence, Italy |
M |
Renal transplant recipient |
Lymphocutaneous |
NA |
NA |
NA |
|
Ursini F. et al. 2015 (18) |
Catanzaro, Southern Italy |
M |
Ankylosing spondylitis, Treatment with adalimubab |
Lymphocutaneous |
Culture |
Unnoticed puncture with rose thorn |
Itraconazole |
|
Lembo S. et al. 2016 (43) |
Naples, Southern Italy |
M |
Diabetes mellitus |
NA |
NA |
Gardening |
Itraconazole (200mg, twice |
|
Giuffrida R. et al. 2020 (47) |
Calabria, Southern Italy |
M |
none |
Cutaneous |
Microscopic, cultural examination, histological picture |
Thorn bite in a hayloft (agricultural laborer) |
Itraconazole pulse therapy |
|
Monno R. et al. 2020 (48) |
Bari, Southern Italy |
M |
none |
Lymphocutaneous |
Microscopic, cultural, histological picture, MALDI TOF, sequencing |
Contact with marshy water |
Itraconazole, voriconazole |
Abbreviations: NA - not available.
NR - not reported.
CONCLUSIONS
Italy, and Southern Italy in particular, because of the number of reported cases, may be considered as an emerging area for this fungal infection. Microbiologists and clinicians need to be more aware of this so called rare fungal infection and of the potential for this disease also in immunocompromised hosts, especially as currently only a limited number of laboratories are able to perform the diagnosis of this infection. Further environmental investigations need to be performed in Italy as it could be an ideal environment for Sporothrix spp.
Conflict of interest
The authors declare that they do not have any conflicts of interest. There are no other authors to acknowledge.
Funding
None.
Acknowledgements
The Authors wish to thanks Mr. Michelangelo Ferri for his technical assistance.
REFERENCES
[1] de Beer ZW, Duong TA, Wingfield MJ. The divorce of Sporothrix and Ophiostoma: solution to a problematic relationship. Stud Mycol. 2016; 83, 165-91.
[2] Romeo O, Scordino F, Criseo G. New insight into molecular phylogeny and epidemiology of Sporothrix schenckii species complex based on calmodulin encoding gene analysis of Italian isolates. Mycopathologia. 2011; 172 (3), 179-86.
[3] Zhang Y, Hagen F, Stielow B, et al. Phylogeography and evolutionary patterns in Sporothrix spanning more than 14,000 human and animal case reports. Persoonia. 2015; 35, 1-20.
[4] Ferreira BH, Ramírez-Prado JH, Neves GWP, et al. Ploidy Determination in the Pathogenic Fungus Sporothrix spp. Front Microbiol. 2019; 10, 284.
[5] Cafarchia C, Sasanelli M, Lia RP, de Caprariis D, Guillot J, Otranto D. Lymphocutaneous and nasal sporotrichosis in a dog from southern Italy: case report. Mycopathologia. 2007; 163 (2), 75-9.
[6] Duangkaew L, Yurayart C, Limsivilai O, Chen C, Kasorndorkbua C. Cutaneous sporotrichosis in a stray cat from Thailand. Med Mycol Case Rep. 2018; 23, 46-9.
[7] Kaplan W, Broderson JR, Pacific JN. Spontaneous systemic sporotrichosis in nine-banded armadillos (Dasypus novemcinctus). Sabouraudia. 1982; 20 (4), 289-94.
[8] Giosa D, Felice MR, Giuffrè L, et al. Transcriptome-wide expression profiling of Sporothrix schenckii yeast and mycelial forms and the establishment of the Sporothrix Genome DataBase. Microb Genom. 2020; 6 (10), mgen000445.
[9] Chakrabarti A, Bonifaz A, Gutierrez-Galhardo MC, Mochizuki T, Li S. Global epidemiology of sporotrichosis. Med Mycol. 2015; 53 (1), 3-14.
[10] Mora-Montes HM. Special Issue “Sporothrix and Sporotrichosis”. J Fungi (Basel). 2018; 4 (4), 116.
[11] Barros MB, de Almeida Paes R, Schubach AO. Sporothrix schenckii and Sporotrichosis. Clin Microbiol Rev. 2011; 24 (4), 633-54.
[12] Rodrigues AM, de Hoog GS, de Camargo ZP. Sporothrix Species Causing Outbreaks in Animals and Humans Driven by Animal-Animal Transmission. PLoS Pathog. 2016; 12 (7), e1005638.
[13] Aung AK, Teh BM, McGrath C, Thompson PJ. Pulmonary sporotrichosis: case series and systematic analysis of literature on clinico-radiological patterns and management outcomes. Med Mycol. 2013; 51 (5), 534-44.
[14] Brandolt TM, Madrid IM, Poester VR, et al. Human sporotrichosis: A zoonotic outbreak in southern Brazil, 2012-2017. Med Mycol. 2018; doi: 10.1093/mmy/myy082
[15] Schubach TM, de Oliveira Schubach A, dosReis RS, et al. Sporothrix schenckii isolated from domestic cats with and without sporotrichosis in Rio de Janeiro, Brazil. Mycopathologia. 2002; 153 (2), 83-6.
[16] Queiroz-Telles F, Buccheri R, Benard G. Sprorotrichosis in immunocompromised host. J Fungi (Basel). 2019; 5 (1), 8.
[17] Rueda M, Torres N, Bravo F. Disseminated cutaneous sporotrichosis: an unusual case. Dermatol Online J. 2018; 24 (11), 13030/qt2wk6r6w0.
[18] Ursini F, Russo E, Leporini C, et al. Lymphocutaneous Sporotrichosis during Treatment with Anti-TNF-Alpha Monotherapy. Case Rep Rheumatol. 2015; doi: 10.1155/2015/614504.
[19] Arantes Ferreira GS, Watanabe ALC, Trevizoli NC, et al. Disseminated Sporotrichosis in a Liver Transplant Patient: A Case Report. Transplant Proc. 2019; 51 (5), 1621-4.
[20] Aparecida Grazziotin N, Gonçalves IL, Todeschini D, et al. Squamous cell carcinoma subsequent to scarring caused by sporotrichosis: A case report. Rev Iberoam Micol. 2019; 36 (2), 83-5.
[21] Bonamonte D, De Vito D, Vestita M, et al. Aquarium-borne Mycobacterium marinum skin infection. Report of 15 cases and review of the literature. Eur J Dermatol. 2013; 23 (4), 510-6.
[22] Orofino-Costa R, Macedo PM, Rodrigues AM, Bernardes-Engemann AR. Sporotrichosis: an update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics. An Bras Dermatol. 2017; 92 (5), 606-20.
[23] Arenas R, Sánchez-Cardenas CD, Ramirez-Hobak L, Ruíz Arriaga LF, Vega Memije ME. Sporotrichosis: From KOH to Molecular Biology. J Fungi (Basel). 2018; 4 (2), 62.
[24] Oliveira MME, Santos C, Sampaio P, et al. Development and optimization of a new MALDI-TOF protocol for identification of the Sporothrix species complex. Res Microbiol. 2015; 166 (2), 102-10.
[25] Wroblewska M, Swoboda-Kopec E, Kawecki D, Sawicka-Grzelak A, Stelmach E, Luczak M. Infection by a dimorphic fungus Sporothrix schenckii in an immunocompromised patient. Infection. 2005; 33 (4), 289-91.
[26] Criseo G, Malarapiacenza G, Romeo O, Puglisi Guerra A. Lymphocutaneous sporotrichosis in an immunocompetent patient: a case report from extreme southern Italy. Mycopathologia. 2008; 166 (3), 159-62.
[27] Marimon R, Serena C, Gené J, Cano J, Guarro J. In vitro antifungal susceptibilities of five species of Sporothrix. Antimicrob Agents Chemother. 2008; 52 (2), 732-4.
[28] de Oliveira MM, Veríssimo C, Sabino R, et al. First autochthone case of sporotrichosis by Sporothrix globosa in Portugal. Diagn Microbiol Infect Dis. 2014; 78 (4), 388-90.
[29] Li J, Zhan P, Jiang Q, et al. Prevalence and antifungal susceptibility of Sporothrix species in Jiangxi, central China. Med Mycol. 2019; 57 (8), 954-61.
[30] Espinel-Ingroff A, Abreu DPB, Almeida-Paes R, et al. Multicenter, international study of mic/mec distributions for definition of epidemiological cutoff values for Sporothrix species identified by molecular methods. Antimicrob Agents Chemother. 2017; 61 (10), e01057-17.
[31] Brilhante RSN, de Aguiar FRM, da Silva MLQ, et al. Antifungal susceptibility of Sporothrix schenckii complex biofilms. Med Mycol. 2018; 56 (3), 297-306.
[32] Magand F, Perrot JL, Cambazard F, Raberin MH, Labeille B. Autochthonous cutaneous sporotrichosis in France. Ann Dermatol Venereol. 2009; 136 (3), 273-5.
[33] Bachmeyer C, Buot G, Binet O, Beltzer-Garelly E, Avram A. Fixed cutaneous sporotrichosis: an unusual diagnosis in West Europe. Clin Exp Dermatol. 2006; 31 (3), 479-81.
[34] Larsabal M, Gabriel F, Pajaniapadeatchy E, et al. Sporotrichosis in France. Med Mal Infect. 2018; 48 (4), 298-300.
[35] De Bièvre C, Mariat F. Ecological and epidemiological relationships between Sporothrix schenckii, a fungus pathogenic for man and the Ceratocystis genus. Bull Soc Pathol Exot Filiales. 1978; 71 (2), 203-10.
[36] Ventin M, Ramírez C, Ribera M, Ferrandiz C, Savall R, Peyri J. A significant geographical area for the study of the epidemiological and ecological aspect of Mediterranean sporothricosis. Mycopathologia. 1987; 99 (1), 41-3.
[37] Ojeda T, Rodríguez-Pichardo A, Suárez AI, Camacho FM. [Sporotrichosis in Seville (Spain)]. Enferm Infecc Microbiol Clin. 2011; 29 (3), 233-4.
[38] Dias NM, Oliveira MM, Santos C, Zancope-Oliveira RM, Lima N. Sporotrichosis caused by Sporothrix mexicana, Portugal. Emerg Infect Dis. 2011; 17 (10), 1975-6.
[39] Kieselova K, Santiago F, Henrique M. Rose thorn injury. BMJ Case Rep. 2017; doi: 10.1136/bcr-2017-221757.[40] Xirotagaros G, Drogari-Apiranthitou M, Panayiotides IG, et al. Imported lymphocutaneous sporotrichosis in Greece. Br J Dermatol. 2015; 173 (1), 291-3.
[41] Barile F, Mastrolonardo M, Loconsole F, Rantuccio F. Cutaneous sporotrichosis in the period 1978-1992 in the province of Bari, Apulia, Southern Italy. Mycoses. 1993; 36 (5-6), 181-5.
[42] Alberici F, Paties CT, Lombardi G, Ajello L, Kaufman L, Chandler F. Sporothrix schenckii var. luriei as the cause of sporotrichosis in Italy. Eur J Epidemiol. 1989; 5 (2),173-7.
[43] Lembo S, Cirillo T, Marasca C, et al. Sporotrichosis: long-term treatment and follow-up in a diabetic patient from Southern Italy. G Ital Dermatol Venereol. 2016; 51 (5), 576-8.
[44] Baroni A, Palla M, Iovene MR, et al. Sporotrichosis: success of itraconazole treatment. Skin Med. 2007; 6 (1), 41-4.
[45] Gori S, Lupetti A, Moscato G, Parenti M, Lofaro A. Pulmonary sporotrichosis with hyphae in a human immunodeficiency virus-infected patient. A case report. Acta Cytol. 1997; 41 (2), 519-21.
[46] Caroti L, Zanazzi M, Rogasi P, et al. Subcutaneous nodules and infectious complications in renal allograft recipients. Transplant Proc. 2010; 42 (4), 1146-7.
[47] Giuffrida R, Caradonna E, Borgia F, Bartolotta A, Cannavò SP. Pulse itraconazole in the treatment of lymphocutaneous sporotrichosis: A case report from Southern Italy and review of the literature. Dermatol Ther. 2020; 33 (4), e13716.
[48] Monno R, Brindicci G, Romeo O. Infection caused by Sporothrix schenckii: an autochthonous case in Bari, Southern Italy. Eur J Clin Microbiol Infect Dis. 2020; 39 (12), 2457-60.
[49] Criseo G, Romeo O. Ribosomal DNA sequencing and phylogenetic analysis of environmental Sporothrix schenckii strains: comparison with clinical isolates. Mycopathologia. 2010; 169 (5), 351-8.