Le Infezioni in Medicina, n. 2 , 299-303, 2021
LETTERS TO THE EDITOR
Valacyclovir for prevention and treatment of fetal CMV infection: inclusion in the Law 648/96 list and launch of the Italian multicentre observational prospective study “MEGAL-ITALI”
Lorenzo Zammarchi1,2,3, Tiziana Lazzarotto4, Mariarosaria Di Tommaso5, Lina Tomasoni6, Lucia Pasquini7, Luisa Galli8, Giuliana Simonazzi9, Francesco Castelli6, Beatrice Borchi2,3, Irene Campolmi2,3, Sara Ornaghi10, Alessandro Bartoloni1,2, Massimo Andreoni11, Immacolata Pagano12, Sandra Petraglia12, Luca Ramenghi13, Pierangelo Clerici14, Marcello Tavio15, Michele Trotta2,3
1Dipartimento di Medicina Sperimentale e Clinica, Università di Firenze, Firenze, Italia;
2SOD Malattie Infettive e Tropicali, Azienda Ospedaliero-Universitaria Careggi, Firenze, Italia;
3Centro di Riferimento per le Malattie Infettive in Gravidanza della Toscana, Firenze, Italia;
4Laboratorio di Virologia, UO di Microbiologia, Dipartimento di Medicina Specialistica, Sperimentale e Diagnostica, IRCCS Policlinico Sant’Orsola, Università di Bologna, Bologna, Italia;
5Dipartimento di Scienze della Salute, Sezione di Ostetricia e Ginecologia, Università degli Studi di Firenze, Firenze, Italia;
6Dipartimento Universitario di Malattie Infettive e Tropicali, Università degli Studi di Brescia e ASST Spedali Civili, Brescia, Italia;
7Unità di Medicina Fetale, Dipartimento per la Salute della Donna e del Bambino, Azienda Ospedaliero Universitaria Careggi, Firenze, Italia;
8Dipartimento di Scienze della Salute, Università di Firenze, Divisione Malattie Infettive Pediatriche, Ospedale Universitario Pediatrico Anna Meyer, Firenze, Italia;
9Divisione di Ostetricia e Medicina Prenatale, Dipartimento di Scienze Medico Chirurgiche, Policlinico Sant’Orsola, Bologna, Italia;
10Dipartimento di Ostetricia e Ginecologia, Scuola di Medicina e Chirurgia, Università di Milano-Bicocca - Fondazione MBBM, Monza, Italia;
11Clinica di Malattie Infettive, Università Tor Vergata, Roma, Italia;
12Agenzia Italiana del Farmaco (AIFA), Roma, Italia;
13UOC Patologia Neonatale, IRCCS Istituto Giannina Gaslini e Università di Genova, Genova;
14Unità di Microbiologia, ASST Ovest Milanese, Ospedale di Legnano, Legnano, Italia;
15Unità di Malattie Infettive Emergenti e Immunosoppresse, Dipartimento di Gastroenterologia e Trapianti, Università Politecnica delle Marche, Ancona, Italia
Corresponding author
Lorenzo Zammarchi
E-mail: lorenzo.zammarchi@unifi.it
To the Editor:
Cytomegalovirus (CMV) is the most common congenital infection, affecting 0.5-2% of all live births and it is the leading non-genetic cause of congenital sensorineural hearing loss and neurological damage [1].
Medical therapies such as CMV hyperimmune immunoglobulins aim to reduce the risk of vertical transmission, but two randomized controlled trials have found no significant benefit [2, 3]. Unlike other diseases of the TORCH group, serological screening for CMV during pregnancy is not routinely performed in Italy, due to the lack of robust data regarding effective therapeutic interventions. However, interesting data have recently emerged in favor of the use of valacyclovir during pregnancy to prevent and treat fetal CMV infection [4, 5].
Valacyclovir is the L-valine ester of acyclovir which exhibits activity against the CMV DNA polymerase when used at high doses. Several randomized trials have shown that valacyclovir is effective for the prophylaxis of CMV reactivation in transplant recipients [6-8]. Its use is currently approved in patients ≥12 year old for the prophylaxis of CMV reactivation in solid organ transplant patients at a dose of 2 g every six hours for up to 90 days weeks (or longer in high risk patients) [9]. According to the old FDA classification system, valacyclovir is defined as a class B drug, even if there is no evidence of risk in human pregnant women despite the lack of well-controlled studies documenting its safety [10].
An open-label single-arm Phase 2 clinical study published in 2016 demonstrated that valacyclovir, at a dosage of 2 g every 6 hours (8 g per day) administered until delivery to pregnant women with confirmed fetal CMV infection (CMV-DNA detected in the amniotic fluid) and mild to moderate ultrasound and/or bio-humoral fetal changes, significantly increases the percentage of asymptomatic newborns at birth from 43% (20 of 47 fetuses, data obtained from a historical cohort) to 82% (34 of 41 fetuses) [11].
More recently in a randomized double-blind trial involving pregnant women with primary CMV infection, valacyclovir, at the same dosage, was administered from the time of diagnosis of acute primary CMV infection acquired during pregnancy up to the time of amniocentesis resulting in a 70% reduction in the vertical transmission rate, from 30% (14 of 47 amniocentesis) to 11% (5 of 45 amniocentesis, p=0·027; odds ratio 0·29, 95% CI 0·09-0·90) [12, 13]. In this study some newborns, both in the treatment group (four) and in the placebo group (two) resulted to be affected by CMV congenital infection at birth after a negative amniocentesis. Late fetal infection in late second or third trimester after valacyclovir discontinuation was considered the most likely explanation for these findings [13]. These infants with a probable late CMV congenital infection were considered to have a much better prognosis than those infected during early stages of pregnancy [13].
Additional favorable experiences on the use of valacyclovir during pregnancy for prevention and treatment of fetal infection are emerging [14-20].
Despite the growing evidence, valacyclovir was not authorized in Italy for the prevention of infection and treatment of fetal CMV disease in pregnancy, making it difficult to use this therapy which appears to be the only one with proven efficacy for these two conditions [4].
In Italy, the off-label use is governed by Law 648/96 which allows reimbursement by the National Health Service (Sistema Sanitario Nazionale, SSN) for selected medications with a therapeutic indication other than that authorized. This opportunity can be considered when there is no valid therapeutic alternative provided the existence of studies, at least in phase II, that demonstrate adequate efficacy with an acceptable risk profile to support the requested indication [21]. These drugs, once inserted in a special “list”, are administered under the physician’s direct responsibility upon acquisition of written consent and can be reimbursed by the Italian SSN. The inclusion in the list can be considered by the Italian Medicines Agency (Agenzia Italiana del Farmaco, AIFA) following a documented request by patient associations, scientific societies, health authorities, universities, clinicians, or on the recommendation of the AIFA technical-scientific commission.
On March 2020 the Italian Society of Infectious and Tropical Diseases (SIMIT), the Italian Clinical Microbiologists Association (AMCLI) and the Italian Society of Perinatal Medicine (SIMP) decided to jointly submit the request for inclusion of valacyclovir for “prevention of CMV infection and treatment of fetal CMV disease in pregnancy” in the list of law 648/96.
The request has been positively evaluated by the AIFA technical-scientific commission, and on December 2020, valacyclovir has been formally included in the list of reimbursed medicinal products by SSN [21]. The recently approved technical indications are summarized below [21].
Briefly, valacyclovir can be now prescribed to pregnant women for both prevention of congenital CMV infection and to treat confirmed mild to moderate fetal CMV disease. The dosage of valacyclovir is the same for both indications (2g six hourly, total 8g per day) and it does not change in case of multiple pregnancies, while the duration of treatment may vary depending of the single case (see below).
Pregnant women eligible for treatment aimed to prevent maternal-fetal transmission are those diagnosed with primary CMV infection during the periconceptional period or in the first twenty-four weeks of pregnancy. Maternal CMV primary infection is defined in presence of at least one of the following:
a) seroconversion for CMV during pregnancy;
b) serology performed during pregnancy demonstrating the presence of specific CMV IgG and IgM associated with low IgG avidity index;
c) serology performed during pregnancy showing specific CMV IgG and IgM, intermediate IgG avidity index associated with the detection of CMV DNA in maternal whole blood and/or urine and/or saliva.
Eligible pregnant women should start the treatment as soon as possible after diagnosis of primary CMV infection. Treatment can be suspended if the pregnant woman undergoes amniocentesis and Polymerase Chain Reaction (PCR) for CMV-DNA is negative on amniotic fluid. Where the DNA research of the CMV with PCR on amniotic fluid should be positive, the treatment is suspended and a possible further treatment would be restarted in the presence of signs of mild to moderate CMV fetal disease (see below). The amniocentesis has to be scheduled at least eight weeks after the onset of primary maternal infection and not before the twentieth week +1 day of gestation. If the pregnant woman does not undergo amniocentesis, the therapy is scheduled until the twenty-sixth week of gestation.
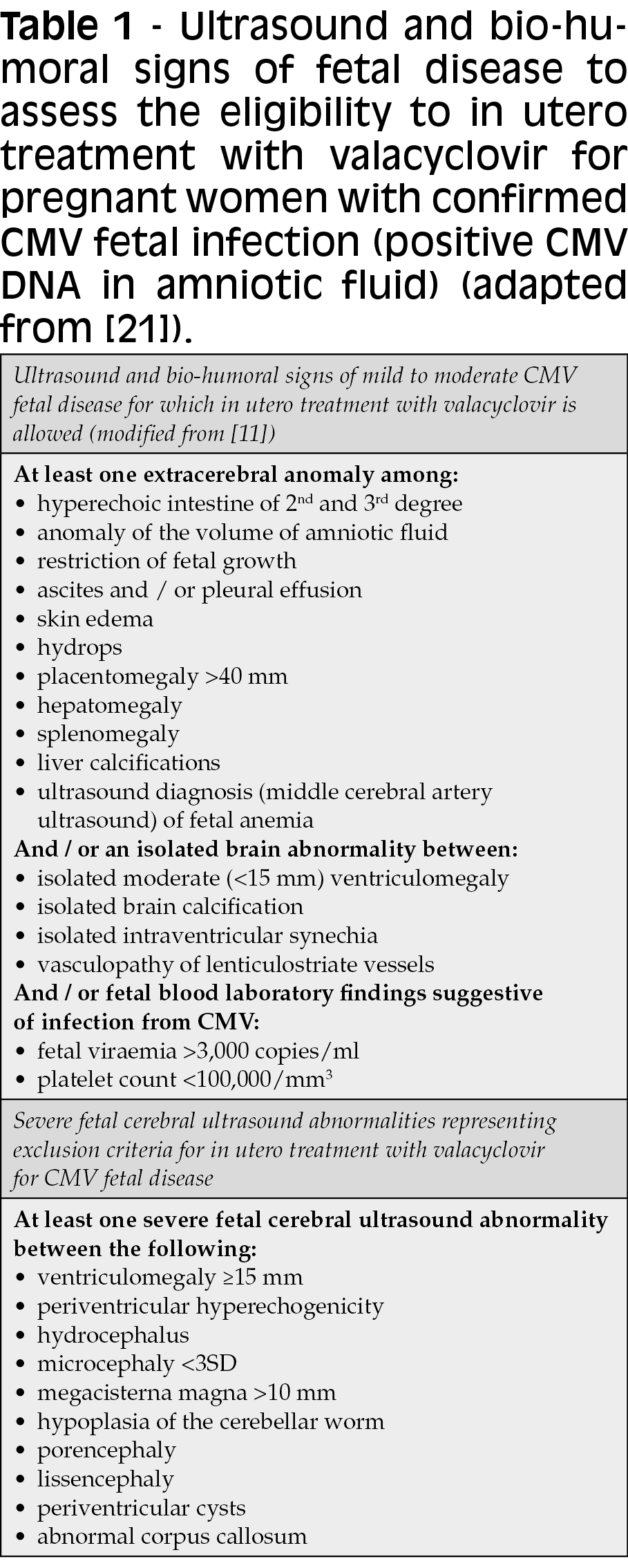
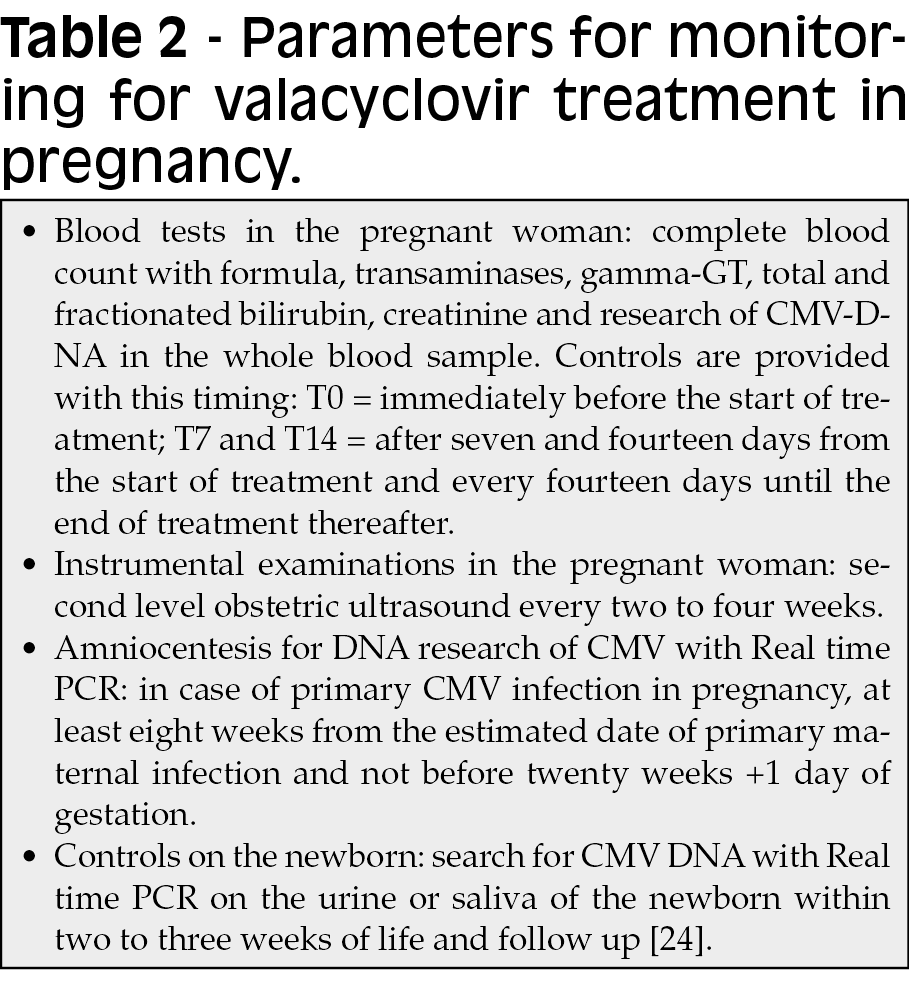
Pregnant women eligible for in utero treatment of mild to moderate fetal CMV disease are those who have been diagnosed with fetal CMV infection by searching for CMV DNA in amniotic fluid (both as a result of primary maternal infection and as a result of non-primary infection) in presence of ultrasound or bio-humoral signs of mild to moderate fetal disease related to CMV (see Table 1 for definition). In this case, the treatment continues until the end of the gestation. This treatment can be additional to a previous one in cases where the pregnant woman has already taken the drug for prevention of maternal-fetal transmission. Exclusion criteria for valacyclovir treatment during pregnancy are age below 12 years, creatinine values >1.1 and glomerular filtration <90 mL/minute. Additional exclusion criteria in case of confirmed CMV fetal infection (positive amniocentesis) are severe fetal cerebral ultrasound abnormalities (see Table 1) or absence of any ultrasound signs suggestive of fetal disease or laboratory abnormalities in fetal blood. Indication for monitoring during valacyclovir treatment are reported in Table 2.
While additional therapeutic interventions such anti-CMV immunoglobulins at higher dose than previously used and newer antiviral drugs such as letermovir seem to be future promising options for prevention and treatment of CMV fetal infection during pregnancy, valacyclovir is now the first proven effective drug that can be prescribed and supplied by the SSN in Italy for these indications [22, 23].
Thus, given the current availability of an effective pharmacological intervention, it becomes imperative to re-evaluate the opportunity to introduce serological screening for CMV in pregnancy.
In order to monitoring the effectiveness and the safety in the clinical practice of valacyclovir for the recently approved indication SIMIT, AMCLI and SIMP are launching a national observational study (MEGAL-ITALI) which is open to every health-care provider and institution in Italy willing to collaborate.
Conflict of interest
All authors report no potential conflicts.
Acknowledgments
We want to thank Alessandra Ipponi, Manuela Angileri and Michele Cecchi of the Farmaceutica ospedaliera e politiche del farmaco – AOU Careggi, Florence, Italy for supporting the initiative.
REFERENCES
[1] Leruez-Ville M, Foulon I, Pass R, Ville Y. Cytomegalovirus infection during pregnancy: state of the science. Am J Obstet Gynecol. 2020; 223, 330-49.
[2] Revello MG, Lazzarotto T, Guerra B, et al. A randomized trial of hyperimmune globulin to prevent congenital cytomegalovirus. N Engl J Med. 2014; 370, 1316-26.
[3] Hughes B. LB17. A randomized trial to prevent congenital cytomegalovirus (CMV). Open Forum Infect Dis. 2019; 6 (Suppl 2), S1000-1.
[4] Zammarchi L, Lazzarotto T, Andreoni M, et al. Management of cytomegalovirus infection in pregnancy: is it time for valacyclovir? Clin Microbiol Infect. 2020; 26 (9), 1151-4.
[5] Zammarchi L, Lazzarotto T, Andreoni M, et al. Valacyclovir for cytomegalovirus infection in pregnancy: additional evidences, additional questions. Clin Microbiol Infect. 2021; 27 (4), 644-5.
[6] Lowance D, Neumayer HH, Legendre CM, et al. Valacyclovir for the prevention of cytomegalovirus disease after renal transplantation. International Valacyclovir Cytomegalovirus Prophylaxis Transplantation Study Group. N Engl J Med. 1999; 340 (19), 1462-70.
[7] Kalil AC, Levitsky J, Lyden E, Stoner J, Freifeld AG. Meta-analysis: the efficacy of strategies to prevent organ disease by cytomegalovirus in solid organ transplant recipients. Ann Intern Med. 2005; 143 (12), 870-80.
[8] Reischig T, Jindra P, Hes O, Svecova M, Klaboch J, Treska V. Valacyclovir prophylaxis versus preemptive valganciclovir therapy to prevent cytomegalovirus disease after renal transplantation. Am J Transplant. 2008; 8 (1), 69-77.
[9] Glaxo Wellcome Inc. Valtrex (valacyclovir hydrochloride). Prescribing information. 2013.
[10] Pasternak B, Hviid A. Use of acyclovir, valacyclovir, and famciclovir in the first trimester of pregnancy and the risk of birth defects. JAMA. 2010; 304 (8), 859-66.
[11] Leruez-Ville M, Ghout I, Bussieres L, et al. In utero treatment of congenital cytomegalovirus infection with valacyclovir in a multicenter, open-label, phase II study. Am J Obstet Gynecol. 2016; 215 (4), 462 e1- e10.
[12] Shahar-Nissan K, Pardo J, Peled O, et al. Valacyclovir to Prevent Vertical Transmission of Cytomegalovirus After Maternal Primary Infection During Pregnancy. Open Forum Infect Dis. 2019; 6 (Suppl. 2), S1002.
[13] Shahar-Nissan K, Pardo J, Peled O, et al. Valaciclovir to prevent vertical transmission of cytomegalovirus after maternal primary infection during pregnancy: a randomised, double-blind, placebo-controlled trial. Lancet. 2020; 396 (10253), 779-85.
[14] De la Calle M, Baquero-Artigao F, Rodríguez-Molino P, et al. Combined treatment with immunoglobulin and valaciclovir in pregnant women with cytomegalovirus infection and high risk of symptomatic fetal disease. J Matern Fetal Neonatal Med. 2020, 1-5. doi: 10.1080/14767058.2020.1815188.
[15] De Santis M, Apicella M, De Luca C, et al. Valacyclovir in primary maternal CMV infection for prevention of vertical transmission: A case-series. J Clin Virol. 2020; 127, 104351.
[16] De Santis M, De Luca C, Apicella M, et al. Prenatal valacyclovir treatment of fetal citomegalovirus infection: A case series. J Infect. 2019; 79 (5), 462-70.
[17] Goncé A, Hawkins-Villarreal A, Salazar L, et al. Maternal high-dose valacyclovir and its correlation with newborn blood viral load and outcome in congenital cytomegalovirus infection. J Matern Fetal Neonatal Med. 2020, 1-5. doi: 10.1080/14767058.2020.1843016.
[18] Jacquemard F, Yamamoto M, Costa JM, et al. Maternal administration of valaciclovir in symptomatic intrauterine cytomegalovirus infection. BJOG. 2007; 114 (9), 1113-21.
[19] Codaccioni C, Vauloup-Fellous C, Letamendia E, Saada J, Benachi A, Vivanti AJ. Case report on early treatment with valaciclovir after maternal primary cytomegalovirus infection. J Gynecol Obstet Hum Reprod. 2019; 48 (4), 287-9.
[20] Hold PM, Wong CF, Dhanda RK, Walkinshaw SA, Bakran A. Successful renal transplantation during pregnancy. Am J Transplant. 2005; 5 (9), 2315-7.
[21] Inserimento del medicinale «Valaciclovir» (originatore o biosimilare) nell’elenco dei medicinali erogabili a totale carico del Servizio sanitario nazionale, per la prevenzione dell’infezione fetale e il trattamento della malattia fetale da citomegalovirus. (Determina n. 142618/2020). (20A07138) Gazzetta Ufficiale - Serie Generale; n.322 del 30-12-2020.
[22] Kagan KO, Enders M, Schampera MS, et al. Prevention of maternal-fetal transmission of cytomegalovirus after primary maternal infection in the first trimester by biweekly hyperimmunoglobulin administration. Ultrasound Obstet Gynecol. 2019; 53 (3), 383-9.
[23] Faure Bardon V, Peytavin G, Lê MP, et al. Placental transfer of Letermovir & Maribavir in the ex vivo human cotyledon perfusion model. New perspectives for in utero treatment of congenital cytomegalovirus infection. PLoS One. 2020; 15 (4), e0232140.
[24] Lazzarotto T, Gabrielli L, Guerra B, et al. Diagnosis and prognosis of congenital CMV infection: a case report and review of the literature. Scand J Clin Lab Invest. Suppl 2014; 244, 34-40; discussion 39.