Le Infezioni in Medicina, n. 2 , 294-296, 2021
LETTERS TO THE EDITOR
Universal screening for SARS-CoV-2 in pregnant women using a combination of antigen and RT-PCR testing
Anil Kumar1, Radhamany Kunjukutty2, Ameena Thaha1, Saranya Srikumar2, Haritha Madhusoodanan2, Sachin David3, Lalitha Biswas4, Dipu Sathyapalan5
1Department of Microbiology, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Ponekkara, Kochi, India;
2 Department of Obstetrics and Gynecology, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Ponekkara, Kochi, India;
3Department of Molecular Biology, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Ponekkara, Kochi, India;
4Center for Nanosciences and Molecular Medicine, Amrita Vishwa Vidyapeetham, Ponekkara, Kochi, India;
5Department of Infectious Disease, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Ponekkara, Kochi, India
Corresponding author
Anil Kumar
E-mail: vanilkumar@aims.amrita.edu
Dear Editor,
It has now become apparent that viral dissemination in COVID-19 occurs from asymptomatic individuals, who are often young and healthy, a demographic profile similar to most obstetrical population [1-4]. On admission of such patients to shared antepartum or post-partum units, there is high risk of transmission to neonates, other patients and health care workers (HCW). COVID-19 in obstetrical population presents a unique challenge during this pandemic as they fall under the high risk category and are advised to continue shielding to minimise the risk of infection. Regardless of the COVID-19 pandemic, the obstetrical population cannot safely avoid or delay follow-up hospital visits for antenatal care, when compared to other patients. Viral transmission can be minimised by screening for symptoms of SARS-CoV-2 prior to hospital visits, teleconsultations, rationalising scans and implementing universal screening for SARS-CoV-2. Our study aimed to determine the utility of universal screening protocol using combination of antigen and RT-PCR testing in identifying SARS-CoV-2 infection rate among pregnant women requiring admission and thereby preventing transmission to health care workers.
We conducted a retrospective cohort study of all pregnant women admitted between March to April 2020. Universal screening for SARS-CoV-2 was implemented for all antenatal women who required admission. All patients were required to fill a sample request form documenting their demographic details and presence of COVID-19 symptoms. All patients presenting in the casualty were initially screened for SARS-CoV-2 antigen followed by RT-PCR, while all planned admission were screened only using RT-PCR. All neonates born to positive mothers were also tested for SARS-CoV-2 by RT-PCR only. SARS-CoV-2 antigen was performed on nasopharyngeal (NP) swabs using STANDARD Q COVID-19 Ag (SD Biosensor, Gurgaon, India) which is a rapid chromatographic immunoassay for the qualitative detection of specific antigens to SARS-CoV-2 present in human nasopharynx. A separate NP swab in viral transport medium was used for reverse transcriptase polymerase chain reaction (RT-PCR) for SARS CoV-2 targeting RdRP and E-gene regions (ViroQ SARS-CoV-2 Kit, BAG Diagnostics, GmbH, Germany). The test results were used to guide PPE use, triaging patients, isolating infected patients and appropriate maternal and neonatal care.
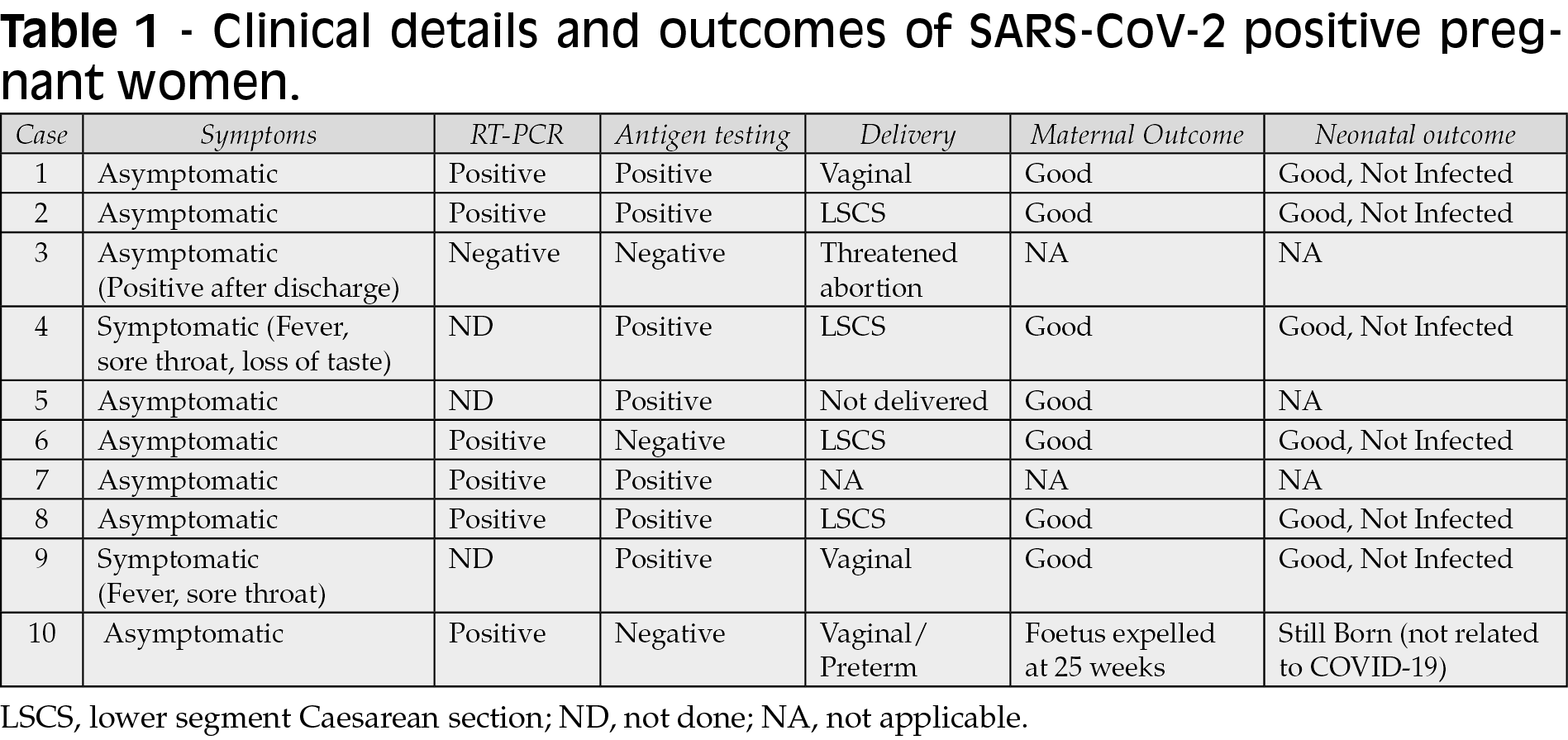
A total of 288 pregnant women were screened for SARS-CoV-2 infection. The estimated prevalence in this sample was 3.47% (10/288). Among the SARS-CoV-2 infected cases, RT-PCR was positive in 85.7% (6/7) and antigen was positive in 70% (7/10) cases. Antigen screening and RT-PCR missed 30% and 14.3% of cases respectively. Among the infected cases only 20% (2/10) were symptomatic and were also positive by antigen test (Table 1). The lone case that was missed by the RT-PCR and antigen assay had become positive three days after discharge. The patient was 11 weeks pregnant and had presented with threatened abortion. She was asymptomatic and developed fever on the second day of admission. Since her urine routine microscopy was positive for bacteria, the fever was attributed to urinary tract infection and the patient discharged on the third day on oral cephalosporin’s. Three days after discharge the patient got tested in a local hospital and was found to be SARS-CoV-2 positive by antigen testing. On epidemiological investigation two HCW who were her primary contacts had been infected. During the study period, the prevalence of positive cases among non-pregnant women aged 20-39 years in our hospital was 2.27% (41/1805). None of the seven neonates that were delivered by infected mothers got infected. There was an increase by 2.7% (8/288) on the use of PPE and isolation precautions for COVID-19 patients on account of universal screening when compared to symptom based screening as most of the patients were asymptomatic.
Due to altered physiology pregnant women who are already susceptible to infections face a high risk of acquiring SARS-CoV-2 due to the need to access healthcare services on a regular basis. Universal screening would enable identification of all symptomatic and asymptomatic carriers at admission and enable the judicious use of PPE and isolation facilities. The prevalence of SARS-CoV-2 in our study was 3.47% which is similar to 3.9% reported by Abeysuriya et al. [1]. However higher prevalence of 19.9%, 15.3%, 12.3% and 6.3% were reported by Vintzileos et al, Sutton et al., Waghmare et al. and Diaz-Corvillon et al. [4-6]. A major concern is that high proportion (80%) of women, who were found to be SARS-CoV-2 positive, was asymptomatic. Similar findings were reported by Waghmare et al. (88.47%), Sutton et al. (87.9%) and Abeysuriya et al. (85.7%) [1, 3, 4]. However a lower prevalence of 66% and 43.2% was reported by Vintzileos et al. and Diaz-Corvillon et al. respectively [5,6]. These findings support the need for universal testing to enable targeted isolation and tracing; since symptomatic screening would have identified only one out of 7 women tested positive for SARS-CoV-2 in our study. With a significant proportion of SARS-CoV-2 infections being asymptomatic, it should be considered in all pregnant women residing in areas with high prevalence.
Identifying SARS-CoV-2 infection in obstetrical patients has implications for both maternal and neonatal care. Universal screening ensures that SARS-CoV-2 positive mothers are accurately identified and isolated to prevent transmission. Moreover, the disease progression can be monitored to provide timely intervention like supplemental oxygen and steroids to prevent complications. Transmission to neonate can also be prevented by immediate separation and implementing contact and airborne precautions during feeding. Though universal screening will invariably increase the PPE usage, it will prevent transmission to HCW and other patients.
Strengths of our study include the use of SARS-CoV-2 antigen and RT-PCR combination for screening. Antigen testing, being simple, rapid and cost effective, can be deployed in large numbers to identify symptomatic or patients with high viral loads. The use of RT-PCR can be reserved for antigen negative cases thereby bringing down the cost of screening in high prevalence areas. Antigen screening being rapid leads to immediate isolation of positive patients thereby preventing transmission. One of the advantages of antigen screening is that it identifies patients with high viral load who are more likely to transmit when compared to RT-PCR which mostly identifies patients with low viral loads due to its superior sensitivity. The drawback of antigen testing is its poor sensitivity (50%) and is more likely to be positive in symptomatic patients. The lack of sensitivity of antigen testing can be compensated with the use of RT-PCR for antigen negative cases. Another drawback is collection of two swabs one for antigen testing and the other for RT-PCR testing in cases where antigen testing is negative. Our study was conducted in tertiary care private hospital with limited patient load and good availability of antigen and RT-PCR testing. Extrapolating the results to other public sector hospitals, standalone maternity hospitals which may not have their own RT-PCR testing facility within India should be done with caution. Additionally, the true prevalence of the virus may be underestimated due to false-negative results.
The prevalence of SARS-CoV-2 infection was higher in pregnant women. The universal screening protocol could identify 90% of cases and allowed us to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment. Antigen testing identified only 70% of cases and lead to immediate isolation of patients thereby preventing transmission. Antigen testing is rapid and cheap and can be implemented in resource poor settings. Maternal and neonatal outcomes were good with none of the neonates being infected. Universal screening is still likely to miss a few infected asymptomatic pregnant women.
Ethical approval
The study was approved by the institutional review board of Amrita Institute of Medical Sciences & Research Centre (IRB-AIMS-2020-321).
Conflict of interest
None declared.
Source of funding
None declared.
REFERENCES
[1] Abeysuriya S, Wasif S, Counihan C, et al. Universal screening for SARS-CoV-2 in pregnant women at term admitted to an East London maternity unit. Eur J Obstet Gynecol Reprod Biol. 2020; 252, 444-6.
[2] Maleki Dana P, Kolahdooz F, Sadoughi F, Moazzami B, Chaichian S, Asemi Z. COVID-19 and pregnancy: a review of current knowledge. Infez Med. 2020; 28 (Suppl. 1); 46-51.
[3] Sutton D, Fuchs K, D’Alton M, Goffman D. Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. N Engl J Med. 2020; 382 (22), 2163-4.
[4] Waghmare R, Gajbhiye R, Mahajan NN, Modi D, Mukherjee S, Mahale SD. Universal screening identifies asymptomatic carriers of SARS-CoV-2 among pregnant women in India. Eur J Obstet Gynecol Reprod Biol. 2021; 256, 503-5.
[5] Vintzileos WS, Muscat J, Hoffmann E, et al. Screening all pregnant women admitted to labor and delivery for the virus responsible for coronavirus disease 2019. Am J Obstet Gynecol. 2020; 223 (2), 284-6.
[6] Díaz-Corvillón P, Mönckeberg M, Barros A, Illanes SE, Soldati A, Nien JK, et al. Routine screening for SARS CoV-2 in unselected pregnant women at delivery. PLoS One. 2020; 15(9), e0239887.