Le Infezioni in Medicina, n. 2 , 272-277, 2021
CASE REPORTS
Elbasvir/Grazoprevir combination therapy in a B-NHL patient with HCV genotype 1 infection
Antonello Sica1, Alessandro Spada1, Caterina Sagnelli2, Pasquale Verolino3, Annalisa Mazzocca4, Evangelista Sagnelli2, Giuseppe Colella5, Salvatore Guastafierro1, Aldo Marrone4
1Department of Precision Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy;
2Department of Mental Health and Public Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy;
3Plastic Surgery Unit, Multidisciplinary Department of Medical-Surgical and Dental Specialties, University of Campania “Luigi Vanvitelli”, Naples, Italy;
4Department of Advanced Medical and Surgical Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy;
5Multidisciplinary Department of Medical Surgery and Dental Specialties, University of Campania “Luigi Vanvitelli”, Naples, Italy
Corresponding author
Caterina Sagnelli
E-mail: caterina.sagnelli@unicampania.it
SummaRY
Patients with indolent non-Hodgkin lymphomas (NHL) may often be followed up only with observation, reserving chemotherapy in case of spread. Patients with chronic HCV infection and B cell NHL frequently undergo regression of lymphoproliferative disease once HCV infection is eradicated by treatment. Interferon (IFN)-based therapy has been the treatment of choice for years, remaining unclear whether it is effective in B cell NHL directly or through HCV eradication, since IFN is effective in both HCV infection and B cell NHL. IFN therapy for HCV infection became obsolete with the advent of the well tolerated direct-acting antiviral agents (DAAs), whose excellent efficacy in treating patients with chronic HCV infection and B cell NHL has been recently highlighted. We treated a 53-year-old woman with chronic HCV infection and marginal zone lymphoma (MZL) with elbasvir plus grazoprevir in 2018, with complete remission and persisting excellent results: sustained virological response 24 weeks after treatment (SVR24). The exclusive role of HCV eradication in B cell NHL regression is also underlined.
Keywords: IFN-free, DAA, non-Hodgkin lymphomas.
INTRODUCTION
As well as being responsible of an acute hepatitis evolving into chronicity in about 70% of cases, with possible evolution into cirrhosis and hepatocellular carcinoma, Hepatitis C Virus (HCV) is a lymphotropic virus which may induce proliferation of B lymphocytes with possible development of lymphoproliferative diseases such as mixed cryoglobulinemia and B cell Non-Hodgkin Lymphoma (B-NHL) [1, 2]. The relationship between HCV and B-NHL has been highlighted in numerous epidemiological and biological studies, but a crucial evidence has been also given by the capability of the anti HCV treatment with pegylated Interferon (peg-IFN), given alone or with ribavirin, to lead to the remission indolent B-NHL lymphomas, especially those of marginal-zone origin [3-5]. Indeed, the complete stable remission of lymphoma once an SVR to anti HCV therapy has been achieved is a concrete strong evidence of such relationship [6-8].
The pathogenetic link between HCV infection and development of certain lymphoma subtypes, mainly Marginal-Zone Lymphomas (MZL), has become even more evident when patients with chronic HCV infection and indolent B-NHL were treated with the Direct Antiviral Agents (DAAs) which induce HCV eradication and B-NHL remission in 95% and 67% of treated patients, respectively [9-12]. Further information in this field is however necessary because new DAAs, potentially more effective than those used previously, have become available over time and others are expected shortly, which are or will be differently associated in treating patients with HCV Chronic Hepatitis (HCV-CH), in relation to viral genotype and subtype and stage of the liver disease [5-8, 13]. Besides, it cannot be excluded that some new DAAs might result more effective on B-NHL than those used to date.
Combination therapy with elbasvir (EBR; HCV-NS5A inhibitor) and grazoprevir (GZR; HCV-S3/4A protease inhibitor) in DAA-naïve patients achieves SVR12 in 96.5% of patients with HCV-related liver cirrhosis and in 97.1% if these are in the compensation phase. This therapeutic combination is also very effective in patients with baseline NS5A mutations, for which SVR12 is achieved in 93.1% of treated cases [14]. This therapy is safe and well tolerated even in patients with advanced kidney disease [14].
This paper aims to make a further contribution to this topic. We describe the case of a 53-year-old woman affected by HCV-CH from more than 15 years who came to our ward for a primary marginal-zone lymphoma of palate. Treated with elbasvir 50 mg plus grazoprevir 100 mg once daily for 12 weeks 2018, this patient achieved the eradication of HCV infection and the complete remission of B-NHL. Primary lymphoma of palate is extremely rare and, in the literature, we have not found cases treated like ours.
CASE REPORT
Already affected from HCV genotype 1b chronic hepatitis C (HCV-CH) from 15 years, a 53-year-old Caucasian woman came to our ward with an outgrowth on her left half-palate arisen in March 2017. No other abnormality was found at physical examination, the blood count and the biochemical profile were normal, excepting for a slight increase in alanine transferase (ALT) serum value (1.2-fold the highest n.v.). The outgrowth was painless and of soft-elastic consistency (Figure 1), morphologically characterized by two swellings, one anterior, rounded of about 1 cm in diameter and the other posterior with indistinct margins which measured 2x1.5 cm. The microscopic examination of incisional biopsies showed a diffuse pattern of lymphoid population, consisting of small cells with some medium-sized elements, and mainly on the periphery, an infiltration of some lobules of a minor salivary gland. Immunohistochemistry displayed a pattern compatible with the diagnosis of non-Hodgkin lymphoma derived from mature B cells (B-NHL) of the marginal-zone origin: positivity for CD20 and bcl2 and negativity for CD3, CD5, CD10, cyclin D1, CD23, with a minority T cell lymphocyte component CD3+, CD5+; Ki67 was 20%. Facial mass Computed Tomography (CT) (Figure 1) showed only a modest thickening of the soft palate tissues in the left paramedian site without pathological impregnation of contrast medium. The abdominal-pelvic ultrasound (US) did not show frankly pathological signs, except for a 10 mm angioma of the spleen already known to the patient, and for a diffusely fibromatous uterus with a fibroid of 23x20 mm in the intramural anterior site. In the left lateral-cervical site, US examination revealed a lymph node of 26 mm in longitudinal diameter at the mandibular corner with conserved roundness index and identifiable hilus, another lymph node with a longitudinal diameter of 17 mm with a hypoechoic US structure and slight loss of the roundness index and two smaller lymph nodes (9 and 6 mm in diameter, respectively) with hypoechoic structure and loss of roundness and sphericity. In the right latero-cervical site, US examination identified a lymph node of 15 mm in diameter with a conserved roundness index and a well-represented hilus at the mandibular corner and another hypoechoic lymph node of 8 mm, with a conserved roundness index. No axillary nor inguinal lymphadenopathy emerged from US examination performed in April 2017. PET/CT (Positron Emission Tomography/Computed Tomography) scan, performed in April 2017, showed an uptake of fluorodeoxyglucose (FDG) only on the left hemi palate (SUV: 4.0) and on the left retromandibular region (SUV: 3.7). Bone marrow microscopy examination didn’t show lymphocytes or other B cells infiltration, confirmed after immunohistochemistry.
All this considering, the diagnosis we made was primary MZL of palate in stage IE according to Ann Arbor staging with low risk (73% of overall survival and 87% of complete response), according to the MALT-IPI prognostic score. Since immediate chemotherapy was not required, the patient was included in a careful “watch and wait” program in which, if clinical symptoms and / or signs or laboratory abnormalities indicating reactivation of the disease occurred, appropriate therapy would be started. It was also preferable to postpone radiotherapy due to the particular difficulties linked to the presentation site. Considering that she was in quite good clinical condition and non-responder to a previous peg-IFN + ribavirin treatment, and that preliminary literature data have shown the great efficacy of some DAAs in both eradicating HCV and inducing the remission of B-NHL, a treatment with t elbasvir 50 mg plus grazoprevir 100 mg once daily was administered for 12 weeks, from April 2018 to June 2018. Before DAA treatment has started, a Fibro-Scan examination of the liver showed 5.5 kPa (F0-F1) and an abdominal US a low-grade bright liver. The baseline HCV-RNA load was 13,643,500 IU and the ALT normal; serum markers of HBV and HIV infections, ANA, AMA, and SMA were all negative. PET/CT was performed in august 2018 and none uptake of FDG was found. At the end of the treatment, the palatine lesion was no longer visible (Figure 2), Complete Remission (CR), and the HCV infection eradicated (SVR24). She began follow up every three months performing: blood count, ALT, AST, HCV RNA PCR test, SPE (serum electrophoresis), bilirubin, ESR (erythrocyte sedimentation rate), creatinine, LDH (lactate dehydrogenase), oral clinical examination. All tests are normal until the last check performed in September 2019. On this date she performed PET/CT too, that confirmed CR. Thus, we decided to perform laboratory and clinical checks every 6 months. In October 2020, all tests were normal.
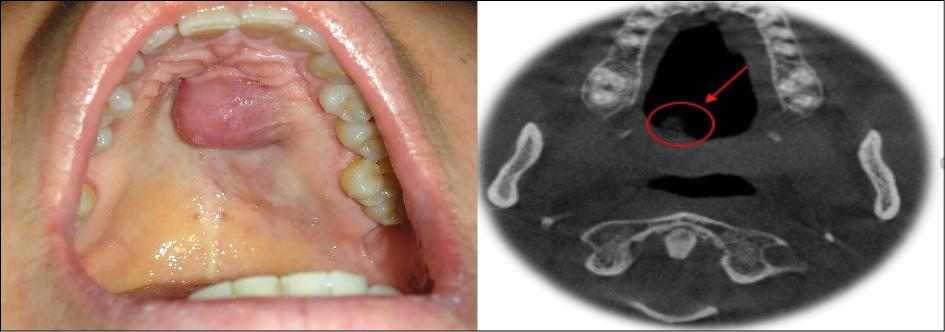
Figure 1 - Swelling of the left hemi palate (picture and massive facial CT, taken before treatment on March 2017.

Figure 2 - The palatine swelling after a 12-week treatment with 50 mg of elbasvir and 100 mg of grazoprevir (picture taken on June 2018).
DISCUSSION
Extranodal MZL represents 9% of all NHL, are more frequent in middle and advanced age with predominance in women, and usually show an indolent course [15, 16]. Indeed, non-gastric MALT lymphomas are scarcely susceptible to systemic spread and need of treatment should be assessed on a case-by-case basis. It is therefore possible for asymptomatic patients to be followed up untreated for varying periods only with observation (watch and wait). HCV, although not strictly lymphotropic, is strongly associated with the onset of indolent NHL, mainly with MZL, this being more evident in geographic areas where the prevalence of subjects with HCV infection is high. The close relationship between HCV infection and MZL is also proven by the favorable effect of both IFN-based and DAAs anti HCV treatments on B-NHL. First observed by Hermine et al. in 2002 in 9 patients with splenic MZL (SMZL) with hairy lymphocytes, subsequent literature data confirmed the favorable influence of anti HCV therapy on B-NHL, therapeutic strategy that has become over time a first-line therapeutic approach for patients with HCV-associated indolent lymphoma not requiring immediate chemotherapy [17, 18]. Recent studies have strongly supported the validity of this approach for all histological typologies of indolent B-NHL associated with HCV infection [19]. A systematic review on the efficacy of IFN-based treatment in lymphoproliferative disorders published in 2005, analyzing 16 studies with 65 patients with HCV chronic infection and lymphoproliferative disorders, reported a complete remission of lymphoproliferative illness in 75% of cases. Accordingly, the Italian Lymphoma Foundation found a strong correlation between the anti-viral and anti-lymphoma response in patients with indolent lymphoma and HCV chronic infection treated with IFN-based therapy [38]. The high regression rates of indolent NHL lymphomas in HCV positive patients obtained with IFN-based therapy, disregarding the histologic subtype, has been unequivocally confirmed in recent studies, B-NHL lymphomas of the marginal area being the most frequent subtype involved. It remained unclear, however, whether the good results obtained were attributable to either the eradication of HCV, or to a direct action of IFN on lymphoma, or to both actions. This question became of fundamental importance in 2014/2015 when the need to replace IFN-based therapy with the more active DAAs became crucial for HCV treatment.
As expected, treatment of chronic hepatitis C has changed in recent years, with the progressive increased use of IFN-free DAA treatment and the progressive abandonment of IFN-based therapy, decidedly less effective and burdened with frequent severe adverse reactions. Already from its first applications, DAA therapy provided very encouraging results and opened new horizons in the management of HCV related lymphoproliferative syndromes. A review article by Arcaini et al. reported the effect of IFN-free DAA regimens in 45 patients with HCV chronic infection and indolent NHL: SVR and regression of lymphoproliferative disease were achieved by 98% and 67% of treated patients, respectively [20]. Elbasvir/grazoprevir combination is strongly indicated to treat patients chronically infected with HCV genotypes 1 or 4, including those with cirrhosis or comorbidities, such as HIV infection or chronic kidney disease [14]. The elbasvir/grazoprevir combination is also very effective in the retreatment of patients with prior therapeutic failures with interferon-based treatments. Furthermore, worthy of mention is the observation that the combination of elbasvir/grazoprevir /sofosbury ± ribavirin is effective and safe for difficult-to-cure patients who had relapsed after a first line DAA treatment [21].
Similar results were seen in two patients with B-NHL and chronic HCV infection treated within the FIL BArT study [EudraCT number: 2015-004830-81] with IFN-free DAA regimens:
a) a 42-year-old male patient with HCV genotype 1 infection and SMZL with lymphocytosis, treated with a combination of faldaprevir, deleobuvir and ribavirin for 16 weeks, showed a rapid virological response (HCV-RNA become undetectable within the 4th week of treatment) and a concomitant resolution of splenomegaly and lymphocytosis;
b) a 57-year-old female patient with HCV genotype 3a infection and MALT-MZL in stage IV (Ann Arbor classification) involving breast, humeral tree and cervical lymph nodes, treated with sofosbuvir and ribavirin for 4 weeks and then with sofosbuvir and daclatasvir for additional 12 weeks, achieved SVR and a complete regression of lymphoma locations as shown by CT scan.
The favorable results from these studies led us to treat our patient with a combination of the highly effective latest generation DAAs available at the time of treatment, elbasvir 50 mg plus 100 mg grazoprevir daily for 12 weeks. The result of treatment should be considered excellent since both a SVR24 and the complete regression of lymphomatous disease were obtained [5, 16, 22]. The excellent results obtained with IFN-free DAA treatment suggest that the regression of indolent NHL may be attributable to the eradication of HCV infection and that IFN-based therapy should no longer be used in this clinical context [23-25]. However, prospective data from large, prospective, controlled studies are needed for an accurate comparative evaluation of the efficacy of possible combinations of the available DAAs in different histologic type of NHL variously associations with different genotypes and subtypes of HCV.
Conflict of interest
The authors have no conflicts of interest (political, personal, religious, ideological, academic, intellectual, commercial or any other) to declare in relation to this manuscript.
Funding
None
Statement of ethics
All procedures performed were in accordance with the Helsinki declarations and the roles of the Italian lows of privacy. Patient signed an anonymous informed consent for the use of his data for anonymous clinical investigations and scientific publications.
Author Contributions
Conceptualization, methodology, visualization, validation, formal analysis; data curation, investigation, writing, original draft preparation A Sica, A Spada, CS, and A Marrone.
Data curation, and visualization, PV, A Mazzocca, GC, SG; writing, review and editing, and visualization, ES; supervision, A Marrone.
REFERENCES
[1] Paydas S, Kilic B, Yavuz S, et al. Anti-HCV and HCV-RNA prevalence and clinical correlations in cases with non-hodgkin’s lymphoma. Am J Hematol. 2003; 74 (2), 89-93.
[2] Sica A, Casale B, Spada A, et al. Differential Diagnosis: Retroperitoneal Fibrosis and Oncological Diseases. Open Med (Wars). 2019; 15, 22-6.
[3] Merli M, Frigeni M, Alric L, et al. Direct-Acting Antivirals in hepatitis C virus-associated diffuse large b-cell lymphomas. Oncologist. 2019; 24 (8), e720-9.
[4] Sica A, Casale B, Dato MTD, et al. Cancer- and Non-cancer Related Chronic Pain: From the Physiopathological Basics to Management. Open Med (Wars). 2019; 14, 761-6.
[5] Merli M, Defrancesco I, Visco C, Besson C, et al. Direct-acting antivirals in relapsed or refractory hepatitis C virus-associated diffuse large B-cell lymphoma. Leuk Lymphoma. 2020; 61 (9), 2122-8.
[6] Pisaturo M, Guastafierro S, Filippini P, et al. Absence of occult HCV infection in patients experiencing an immunodepression condition. Infez Med. 2013; 21 (4), 296-301.
[7] Coppola N, Pisaturo M, Guastafierro S, et al. Increased hepatitis C viral load and reactivation of liver disease in HCV RNA-positive patients with onco-haematological disease undergoing chemotherapy. Dig Liver Dis. 2012; 44 (1), 49-54.
[8] Sica A, Vitiello P, Ronchi A, et al. Primary Cutaneous Anaplastic Large Cell Lymphoma (pcALCL) in the elderly and the importance of sport activity training. Int J Environ Res Public Health. 2020; 17 (3), 839.
[9] Vitiello P, Sica A, Ronchi A, Caccavale S, Franco R, Argenziano G. Primary cutaneous B cell lymphomas: an update. Front. Oncol. 2020; 27, 10, 651.
[10] Sica A, Vitiello P, Papa A, et al. Use of Rituximab in NHL Malt Type Pregnant in I Trimester for Two Times. Open Med (Wars). 2019; 14, 757-60.
[11] Reginelli A, Urraro F, Sangiovanni A, et al. Extranodal Lymphomas: a pictorial review for CT and MRI classification. Acta Biomed. 2020; 91 (8-S), 34-42.
[12] Ronchi A, Zito Marino F, Vitiello P, et al. A case of primary cutaneous B-cell lymphoma with immature features in an old man. Diffuse Large B-cell Lymhpoma with immature features or B-cell Lymhpoblastic Lymphoma? J Cutan Pathol. 2020; 48 (4), 535-40.
[13] Sica A, Vitiello P, Caccavale S, Sagnelli C, et al. Primary Cutaneous DLBCL Non-GCB Type: Challenges of a Rare Case. Open Med (Wars). 2020; 15, 119-25.
[14] Kumada H, Suzuki Y, Karino Y, Chayama K, Kawada N. The combination of elbasvir and grazoprevir for the treatment of chronic HCV infection in Japanese patients: a randomized phase II/III study. J Gastroenterol. 2017; 52 (4), 520-33.
[15] Sica A, Sagnelli C, Papa A, et al. An anecdotal case report of chronic lymphatic leukemia with del(11q) treated with ibrutinib: artificial nourishment and physical activity program. Int J Environ Res Public Health. 2020; 17 (6), 0. doi: 10.3390/ijerph17061929.
[16] Kawamura Y, Ikeda K, Arase Y, et al. Viral elimination reduces incidence of malignant lymphoma in patients with Hepatitis C. Am J Med. 2007; 120 (12), 1034-41.
[17] Hermine O, Lefrère F, Bronowicki JP, et al. Regression of splenic lymphoma with villous lymphocytes after treatment of hepatitis C virus infection. N Engl J Med. 2002; 347 (2), 89-94.
[18] Mele A, Pulsoni A, Bianco E, et al. Hepatitis C virus and B-cell non-Hodgkin lymphomas: an Italian multicenter case-control study. Blood. 2003; 102 (3), 996-9.
[19] Pozzato G, Mazzaro C, Dal Maso L, et al. Hepatitis C virus and non-Hodgkin’s lymphomas: meta-analysis of epidemiology data and therapy options. World J Hepatol. 2016; 8 (2), 107-16.
[20] Arcaini L, Vallisa D, Rattotti S, et al. Antiviral treatment in patients with indolent B-cell lymphomas associated with HCV infection: a study of the Fondazione Italiana Linfomi. Ann Oncol. 2014; 25 (7), 1404-10.
[21] Papaluca T, Sinclair M, Gow P, et al. Retreatment with elbasvir, grazoprevir, sofosbuvir ± ribavirin is effective for GT3 and GT1/4/6 HCV infection after relapse. Liver Int. 2019; 39 (12), 2285-90.
[22] Cascone R, Sica A, Sagnelli C, et al. Endoscopic treatment and pulmonary rehabilitation for management of lung abscess in elderly lymphoma patients. Int J Environ Res Public Health. 2020; 17 (3), 997.
[23] Sica A, Casale B, Sagnelli C, et al. All in One spinal cord stimulation in lymphoproliferative diseases. Front. Neurol. 2020; 11, 550554. doi: 10.3389/fneur.2020.550554.
[24] Visco C, Di Rocco A, Evangelista A, et al. Correction: Outcomes in first relapsed-refractory younger patients with mantle cell lymphoma: results from the MANTLE-FIRST study. Leukemia. 2021; 35 (3), 932
[25] Suarez F, Lortholary O, Hermine O, Lecuit M. Infection-associated lymphomas derived from marginal zone B cells: a model of antigen-driven lymphoproliferation. Blood. 2006; 107 (8), 3034-44.