Le Infezioni in Medicina, n. 2 , 268-271, 2021
CASE REPORTS
Oligosymptomatic diphtheria infection in adults: two contacts of the Peruvian index case after 20 years without disease report
Juan José Montenegro-Idrogo1,2, Cristhian Resurrección-Delgado1,3, César Sánchez-Álvarez1,4, Marcelo Villarreal-Zerpa1,4, Freddy Morales-López1,4, Iván Vargas-Matos2,3,5, Alfredo Juan Chiappe-Gonzalez1,6
1Infectious and Tropical Diseases Service, Hospital Nacional Dos de Mayo, Lima, Peru;
2Facultad de Medicina, Universidad Científica del Sur, Lima, Peru;
3Universidad Peruana de Ciencias Aplicadas, Lima, Peru;
4Unidad de Posgrado, Universidad Nacional Mayor de San Marcos, Lima, Peru;
5Clínica Angloamericana, Lima, Peru
6Universidad Católica Santo Toribio de Mogrovejo, Chiclayo, Peru
Corresponding author
Juan José Montenegro-Idrogo
E-mail: montenegroidrogo@gmail.com
SummaRY
In Peru, diphtheria infection was eradicated in the last two decades. However, recently, diphtheria pharyngeal infection was confirmed and reported in a 5-year-old boy (index case). We report two more cases of this outbreak (in the index case parents) with confirmed diphtheria infection and tox gene identified by molecular assay, who were in close contact with the index case and never presented any symptoms. Both parents had a congestive pharynx with erythematous plaques at the back of it. In adults, diphtheria infection can be oligosymptomatic or mimic viral pharyngitis, which could lead to misdiagnosis and, furthermore, an increased risk of transmission in regions with lower immunization rates.
Keywords: Corynebacterium diphtheriae, diphtheria, outbreak, asymptomatic disease, adult.
INTRODUCTION
Corynebacterium diphtheriae is a gram-positive bacillus, capable of producing diphtheria exotoxin (DT) encoded by the tox gene [1]. DT is responsible for inflammation and tissue destruction in the respiratory tract, myocardium, peripheral nerves, and skin [2]. The incubation period varies between 1 and 10 days (average 2 to 5 days) [1]. Transmission generally occurs after inhalation of respiratory droplets or direct contact with skin lesions. Specific antibiotic therapy for two weeks not only destroys bacteria and eliminates toxin production, but also prevents their transmission and limits the burden that can persist after clinical recovery [1, 3]. Likewise, it has been estimated that an infected person can remain contagious for up to 4 weeks, even in the absence of symptoms [3, 4]. Therefore, early isolation of cases and close contacts means urgent containment action.
The global incidence of diphtheria has decreased markedly by around 90%, especially due to the establishment of vaccination programs, with more than 3 doses of DTP determined according to schedules [3,5]. Timely immunization has a great impact on public health [1, 3, 5]. According to WHO, the establishment of the DTP vaccination program has reduced childhood diphtheria in several countries. Despite this, in endemic areas, such as Asia, Africa, and Eastern Mediterranean countries, the incidence of diphtheria remains high, and the mortality rate reaches 31% [1, 3, 5]. In South America, the latest communication from the Pan American Health Organization (PAHO) reported diphtheria cases up to the thirtieth epidemiological week of 2021 in Brazil, Haiti, the Dominican Republic and Venezuela [6]. On the other hand, in Peru, diphtheria was eradicated in the last two decades.
However, recently, a fatal case of respiratory diphtheria was confirmed in a 5-year-old girl, who only received the BCG vaccine at birth [7]. Ten days before her death, the patient’s one-year-old sister developed mild respiratory disease of uncertain etiology. The girl’s close contacts tested positive on the nasopharyngeal swab real-time polymerase chain reaction (PCR) test. In addition, both parents also tested positive for the tox gene in the molecular PCR assay.
Next, we present the clinical characteristics of the two adults with oligosymptomatic diphtheria infection, both contacts of the index case reported in Lima, Peru [8].
INDEX CASE REPORT
A 5-year-old girl, a native of Contamana, Loreto (Peruvian jungle), who has been living in the country’s capital, Lima, for the past year, entered our institution with five days of upper respiratory symptoms. Ten days before the onset of the condition, her one-year-old sister developed respiratory symptoms lasting seven days. On the other hand, fifteen days before the patient’s illness, her uncle, with whom she had contact, also presented seven days of respiratory symptoms.
Case 1
This is a 30-year-old Peruvian male, a native of Contamana, a textile operator, father of the patient in the index case, who has also been living in Lima for the past year. As important antecedents, the patient refers to having completed his childhood vaccination program (diphtheria and yellow fever included). Likewise, he denied having presented symptoms such as runny and stuffy nose, epistaxis, cough or other respiratory discomfort during the last month. During the second day of his daughter’s hospitalization, the patient received boosted immunization against diphtheria/tetanus (DT), as well as intramuscular benzathine penicillin in a contact prophylactic dose. In addition, a nasopharynx swab was performed for molecular PCR assay, which was later positive for diphtheria, with the presence of the tox gene. Likewise, C. diphtheriae was isolated in a special culture medium (tellurite blood agar 5%) from nasopharyngeal swab.
In continuous medical evaluations, the patient remained asymptomatic. However, the physical examination revealed congestive pharynx with erythematous plaques on the posterior wall of the pharynx. (Figure 1A). No cervical or regional lymphadenopathies were found. The rest of the physical evaluation was normal. In the analysis, the biochemical studies revealed: hemoglobin 14.8 g/dL; white blood cells (WBC) 6260 cells/ml; platelets 308,000/mL; CRP<5 mg/dL (negative); CPK-MB 13.8 U/L; creatinine 0.84 mg/dL; serum troponins in normal ranges; coagulation profile without alteration. Finally, a treatment with erythromycin 500mg 4 times a day for 14 days was established. The patient did not report any symptoms during follow-up and was discharged without complications at the end of antibiotic therapy.
Case 2
This is a 20-year-old Peruvian woman, a native of Contamana, mother of the index case patient, with a history of chronic anemia of probably deficiency etiology, and an obstetric record of two pregnancies at 15 and 18 years of age, whose prenatal controls were irregular, and it was not possible to specify whether or not she received boosted immunization with DT in any gestational control. She had been living in Lima with her husband and her daughters for the last year, where she was a homemaker. The patient reported having completed her childhood vaccination schedule (diphtheria and yellow fever included). She denied experiencing a runny and stuffy nose, epistaxis, cough or other respiratory symptoms in the past month. Likewise, she also received intramuscular benzathine penicillin as a contact prophylactic dose during her daughter’s second hospital day, as well as boosted vaccination with DT. In addition, a pharyngeal swab was performed, which was later positive for diphtheria with the same presence of the tox gene by molecular assay by PCR. The culture of the pharyngeal smear was negative in this case.
During the medical follow-up, the patient remained asymptomatic. However, like her husband, the physical examination revealed a congestive pharynx with erythematous plaques on the posterior wall of the pharynx. (Figure 1B). Her vital functions remained stable, although with a body temperature of 37.5°C. Multiple painless posterior cervical and submandibular lymph adenomegalies, 0.5-1 cm in diameter, mobile were identified. The rest of the physical evaluation was normal. In the analysis, the biochemical studies revealed: hemoglobin 12.2 g/dL; WBC 7910 cells/mL; platelets 359000/mL; CRP<5 mg/dL (negative); CPK-MB 23.5 U/L; creatinine 0.63 mg/dl; normal levels of troponins; coagulation profile without alteration. Treatment with erythromycin 500 mg 4 times a day for 14 days was established. The patient did not report any symptoms during follow-up, being discharged without complications at the end of antibiotic therapy.
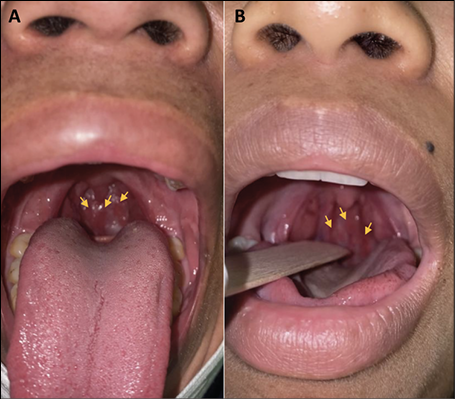
Figure 1 - Oral and pharynx with erythematous plaques. (A). Case 1 (B) Case 2.
DISCUSSION
Diphtheria is decreasing and even being eliminated in many countries; however, it is still present especially in settings of extreme poverty and poor vaccination strategy and coverage [1, 3, 5]. In Peru, during the years 2016-2019, the DPT vaccination coverage achieved was around 72%. Likewise, in 2020, the coverage of the DPT vaccine (first booster) was 24.6% and in the pregnancy controls the DTaP was 31.2%. Therefore, Peru currently has around 683,081 unvaccinated children under 5 years of age at high risk of contracting diphtheria, particularly those in congested urban areas [7].
In the two cases presented in this report, there was an identifiable source of infection, their daughter, who was diagnosed with diphtheria before them. Neither of them had a medical history and did not take any medication regularly. Although both parents were asymptomatic during the anamnesis, the physical examination revealed congestive pharynx with hypertrophy of the right tonsil in the father, and congestive pharynx with multiple cervical lymph nodes in the mother, without evidence of a thick gray layer in the pharynx or tonsils in both cases. The clinical presentations of oligo-asymptomatic diphtheria that could mimic viral pharyngitis are unusually described [3,9-12]. These isolated outbreaks in the world regions described, of poor strategic implementation of vaccination, without being able to administer DT vaccine booster in adolescents or adults, could allow the resurgence of this immune preventable disease.
Among the immediate measures to be implemented in the close contacts of a patient positive for diphtheria are the culture of pharyngeal smears for C. diphtheriae, the investigation of the completion of the vaccination program against C. diphtheriae in the history, the administration of a booster dose of the vaccine according to age in case the last dose had not been administered in the last five years, and medical surveillance for seven days in order to detect evidence of active disease. The data regarding the benefit of diphtheria antitoxin (DAT) as post-exposure prophylaxis between close contacts is very limited, so it was not implemented in either of the two cases presented [3, 5, 11].
Both parents obtained positive results for C. diphtheriae and tox gene in the molecular PCR assay, for which they were finally diagnosed with oligosymptomatic mild diphtheria pharyngitis and received specific antibiotic treatment with oral erythromycin 500 mg every 6 hours for 14 days. Antibiotic therapy has three main benefits. The first consists of directly destroying the bacteria, avoiding the formation of new toxins; second, it decreases and limits the extent of tissue damage; finally, it reduces the risk of transmission of the agent [1,3,4]. Another therapeutic option consists of the application of 50,000 units/day of intravenous penicillin G divided every 12 hours when oral intake is not possible. Then, rotate to 250 mg of oral VK penicillin (fasting) every 6 hours for 14 days, as long as oral intake is possible. Shorter courses of antibiotic treatment are not recommended due to the higher probability of recurrence [1-3, 5].
This outbreak is of great importance and epidemiological alert, demonstrating that the resurgence of this rare disease could be explained by a decrease in vaccination coverage in children, deficient national immunization programs in adults, recent migration of the population, late recognition of a epidemic and irregular supply of vaccines [3, 5, 11].
In conclusion, these cases describe that oligosymptomatic diphtheria infection can occur in adults and can be underdiagnosed due to the similarity of pharyngeal infections of viral etiology. In addition, in regions with a lower childhood immunization rate and without adequate immunization booster compliance rates as established in the national adult vaccination schedule, could allow the resurgence of immune preventable diseases that were eradicated several years ago.
Authorship Statement
All authors meet the ICMJE authorship criteria. JMI was responsible for the organization and coordination of the report. JMI, CRD, CSA, MVZ, FML, and ACG developed the case report. All authors contributed to the writing of the final manuscript. All members approved final manuscript.
Conflicts of interest
All authors report no conflicts of interest.
Funding
None
REFERENCES
[1] Sharma NC, Efstratiou A, Mokrousov I, Mutreja A, Das B, Ramamurthy T. Diphtheria. Nat Rev Dis Primers. 2019; 5; 5 (1), 81.
[2] Hadfield TL, McEvoy P, Polotsky Y, Tzinserling VA, Yakovlev AA. The pathology of diphtheria. J Infect Dis. 2000; 181 (Suppl. 1), S116-S120.
[3] Truelove SA, Keegan LT, Moss WJ, et al. Clinical and epidemiological aspects of diphtheria: a systematic review and pooled analysis. Clin Infect Dis. 2020; 71 (1), 89-97.
[4] WHO. 2017. Operational protocol for clinical management of diphtheria. Bangladesh, Cox’s Bazar (version 10th Dec 2017). [cited 31 Oct 2020]. Available on:
[5] Clarke KEN, MacNeil A, Hadler S, Scott C, Tiwari TSP, Cherian T. Global Epidemiology of Diphtheria, 2000-2017. Emerg Infect Dis. 2019; 25 (10), 1834-42.
[6] OPS/OMS. 2020. Boletín epidemiológico. Actualización Epidemiológica Difteria 22 septiembre 2020. [cited 31 Oct 2020] Available on: https://www.paho.org/es/documentos/actualizacion-epidemiologica-difteria-22-septiembre-2020
[7] CDC-MINSA. 2020. Riesgo de transmisión de Difteria ante la confirmación de un caso en el Perú. Alerta epidemiológica N. 24. [cited 31 Oct 2020] Available on: https://cdn.www.gob.pe/uploads/document/file/1409915/Alerta%20epidemiol%C3%B3gica%20N%C2%B0%2024.pdf
[8] OPS/OMS. 2020. Alerta Difteria [cited 01 Feb 2021] Available on: https://www.paho.org/es/noticias/ 5-11-2020-alerta-difteria
[9] Habib H, Kurniawaty H. Triage in the time of diphtheria. West J Emerg Med. 2020; 21 (5), 1156-9.
[10] Okamoto K, Hatakeyama S, Sugita C, et al. Nasal diphtheria (chronic carriage) caused by nontoxigenic Corynebacterium diphtheriae. J Infect Chemother. 2018; 24 (9), 759-62.
[11] Jané M, Vidal MJ, Camps N, et al. A case of respiratory toxigenic diphtheria: contact tracing results and considerations following a 30-year disease-free interval, Catalonia, Spain, 2015. Euro Surveill. 2018; 23 (13), 17-00183.
[12] Loganathan T, Mohamed PY. Adult diphtheria in Malaysia: a case report. Med J Malaysia. 2018; 73 (5), 340-1.