Le Infezioni in Medicina, n. 2 , 263-267, 2021
CASE REPORTS
Cutaneous tuberculosis on the scalp: a case report
Bruno Hassunuma Carneiro1, André Gama Palone1, Carine Andrade Celeira Zanlorenzi1, João Guilherme Bochnia Küster1, Marcelo Abreu Ducroquet2, João Adriano de Barros1
¹Department of Internal Medicine, Hospital de Clínicas da Universidade Federal do Paraná, Curitiba, Brazil;
²Department of Infectious Diseases, Hospital de Clínicas da Universidade Federal do Paraná, Curitiba, Brazil
Corresponding author
Bruno Hassunuma Carneiro
E-mail: brunohcarneiro2@gmail.com
SummaRY
Tuberculosis is a disease that usually affects the lungs, although other systems may also be infected, resulting in atypical clinical presentations. We report the case of a 76-year-old man who was admitted to the hospital in Brazil with a 3-week history of a painful, enlarging ulcer on the scalp and cough. His medical history was notable for non-metastatic prostatic adenocarcinoma and esophageal squamous cell carcinoma. On physical examination, the ulcer measured 10 cm in diameter and was tender, with a firm border and yellow crusts. A punch-biopsy specimen of the edge of the ulcer showed acute and chronic non-specific inflammation and neutrophilic infiltrates. Acid-fast bacilli were seen on microscopic examination, molecular testing detected Mycobacterium tuberculosis DNA and pan-sensitive M. tuberculosis was cultured. Computed tomography (CT) scan of the head showed a frontoparietal osteolytic lesion under the ulcer, chest CT revealed areas of consolidation in the lower lobes and M. tuberculosis was also identified in a bronchoalveolar lavage specimen. After one month of combination therapy with rifampin, isoniazid, pyrazinamide and ethambutol his symptoms were found to be improving and the size of the ulcer was markedly reduced.
Keywords: Tuberculosis, cutaneous tuberculosis, skeletal tuberculosis, pulmonary tuberculosis.
INTRODUCTION
Tuberculosis (TB) is one of the top 10 causes of death worldwide and the leading cause of death from a single infectious agent. It is estimated that about 2 billion people have latent tuberculosis infection (LTBI), which means that they are infected by Mycobacterium tuberculosis but have not developed signs and symptoms of the disease and cannot spread the bacilli [1].
In the past 10 years, an average of 71,000 new cases of TB were diagnosed per year in Brazil. The incidence rate of TB varies across the states from 10 to 75 cases per 100,000 habitants per year [2, 3].
Extra-pulmonary tuberculosis accounts for 16% of all TB cases worldwide, and cutaneous disease is a very uncommon presentation, occurring only in less than 2% of all extra-pulmonary cases [1, 4].
We describe a unique case of concomitant pulmonary, skeletal and cutaneous TB presenting as an atypical, large scalp ulcer.
CASE REPORT
A 76-year-old man from Southern Brazil was admitted to the hospital complaining of a painful ulcer on his scalp. He noticed the onset of the lesion approximately three weeks before presentation, with significant enlargement and worsening of symptoms in the last week. He also reported daily chills, cough and weight loss. He denied nausea, vomiting, changes in urine or stool or any other symptoms.
His past medical history was remarkable for non-metastatic prostatic adenocarcinoma, treated with radiotherapy and chemotherapy 10 years from presentation, esophageal squamous cell carcinoma, treated with neoadjuvant chemotherapy, esophagectomy with esophagogastric anastomosis and radiotherapy in the previous year, chronic osteomyelitis of the right humerus and a smoking load of 30 pack-years.
On physical examination, his skin and conjunctivae were pale and dry. The ulcer on his scalp measured 10 cm in diameter and was found to be tender, with a firm border and yellow crusts (Figure 1). His blood pressure was 90/60 mmHg, respiratory rate 22 bpm, heart rate 112 bpm, Sat.O2 94% (FiO2 0.21), axillary temperature 37.6 ºC, body weight 58kg, BMI 18kg/m². He had reduced right shoulder mobility. Respiratory, cardiovascular, gastrointestinal and neurological systems examination were unremarkable. An electrocardiogram revealed sinus tachycardia.

Figure 1 - Cutaneous ulcer on the scalp caused by Mycobacterium tuberculosis.
Laboratory evaluation showed normocytic normochromic anemia, mild hyponatremia, hypoalbuminemia and mild elevation in high-sensitivity C-reactive protein level. He tested negative for HIV (fourth-generation HIV-1/2 immunoassay) and syphilis (treponemal chemiluminescence immunoassay).
Chest Computed Tomography (CT) scan showed a small left-sided pleural effusion, centrilobular and paraseptal emphysema, peribronchovascular and periferic bilateral reticular opacities associated with dilated bronchi, ground-glass opacities and consolidation in the lower lobes with bronchial thickening (Figures 2A and 2B). He underwent bronchoscopy and a bronchoalveolar lavage was obtained. Molecular testing (GeneXpert MTB/RIF assay) detected rifampin-sensitive Mycobacterium tuberculosis DNA.
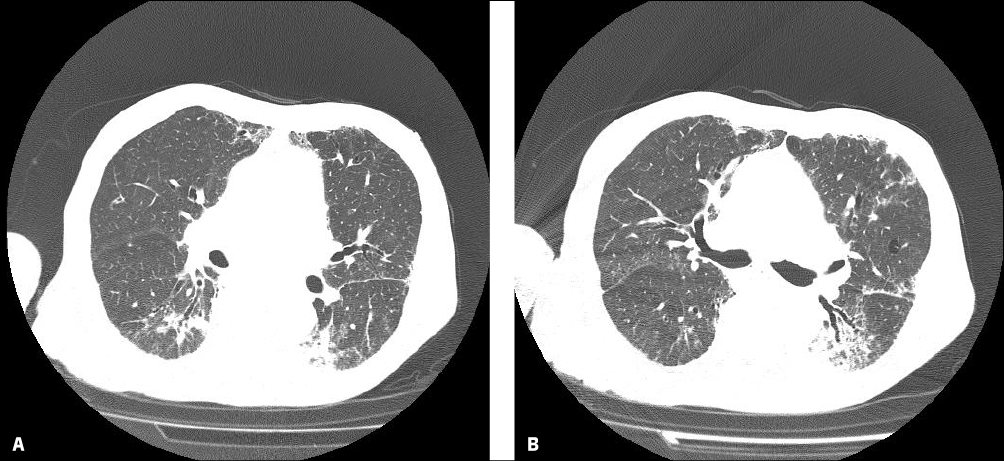
Figure 2 - Chest CT showing pulmonary opacities and consolidation in the lower lobes.
A punch-biopsy specimen of the edge of the scalp ulcer was obtained and sent to the histology and microbiology laboratories. Histopathological tissue analysis revealed acute and chronic non-specific inflammation and neutrophilic infiltrates. Upon microbiological evaluation, acid-fast bacilli were identified using the Ziehl-Neelsen method of staining, molecular testing detected rifampin-sensitive Mycobacterium tuberculosis DNA and pan-sensitive M. tuberculosis was cultured on Löwenstein–Jensen medium. A head CT was obtained and it revealed a right-sided frontoparietal osteolytic lesion under the cutaneous ulcer (Figures 3A, 3B and 3C).
Combination therapy with rifampin, isoniazid, pyrazinamide and ethambutol was initiated, and the patient was discharged. On follow-up, after one month of treatment, his symptoms were found to be improving and the size of the ulcer was markedly reduced. Unfortunately, a few months later, the patient died from cancer-related complications.
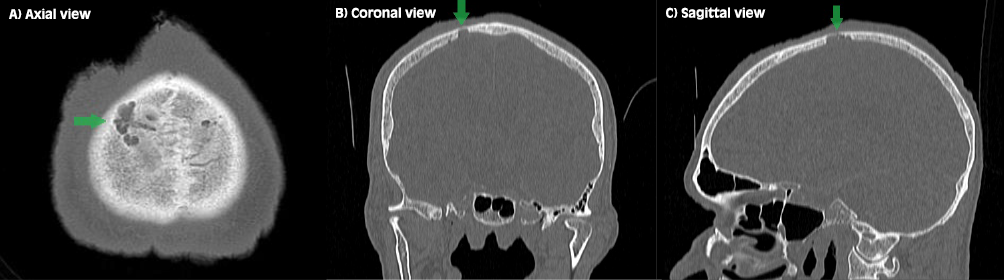
Figure 3 - Head CT showing a right-sided frontoparietal osteolytic lesion (green arrows).
DISCUSSION
The risk of developing TB is higher among individuals with an impaired immune system, diabetes mellitus, malnutrition, smoking, alcoholism and other risk factors [1]. Patients with solid and hematological malignancies are also believed to have an increased risk [5]. In addition, chemotherapy often promotes transient neutropenia and other immunological deficiencies that may increase the risk of infection, and reactivation of TB during cancer treatment has been reported [6, 7]. Screening for LTBI has been proposed for persons at increased risk using the Tuberculin Skin Test (TST) or Interferon Gamma Release Assays (IGRAs) [8]. IGRAs appear to be more sensitive and to perform better than TST in immune-compromised patients [8, 9]. Brazilian guidelines recommend treating high-risk individuals after a diagnosis of LTBI with isoniazid [3].
Cutaneous TB comprises a wide spectrum of clinical presentations, with different physiopathological mechanisms, which depend on factors related to the host’s individual immunological aspects and the mechanism of transmission involved. The mechanisms previously reported are: exogenous inoculation, which may originate tuberculous chancre and tuberculosis verrucosa cutis; continuity or autoinoculation, which may present as scrofuloderma, orificial tuberculosis, and lupus vulgaris; hematogenic and lymphatic dissemination from a primary focus of infection, which may lead to tuberculous gumma, acute miliary TB and lupus vulgaris. There are also tuberculids, a category of skin disorders associated with TB that represents, most likely, immune hypersensitivity reactions to M. tuberculosis antigens [4, 10, 11].
The clinical appearance of cutaneous TB is quite varied; inflammatory papules, verrucous plaques, suppurative nodules, ulcers and other lesions can be identified [12, 13]. Besides a suggestive clinical presentation, histologic criteria can aid in the diagnosis. The characteristic histopathological finding is the tuberculoid granuloma with caseous necrosis [11]. Although tuberculoid granulomas are a common finding, their detection does not confirm the presence of TB, and their absence does not exclude the diagnosis, as other disorders may also present with tuberculoid granulomas [14-16]. The diagnosis is confirmed by identification of M. tuberculosis DNA by nucleic acid amplification tests and mycobacterial culture [4, 11]. In difficult cases, a therapeutic trial of anti-TB medications may be used to confirm the diagnosis of cutaneous TB and the response to multidrug therapy is usually evident within six weeks [17, 18]. In Brazil, the preferred regimen for treating pan-sensitive M. tuberculosis infection is combination therapy with rifampin, isoniazid, pyrazinamide and ethambutol in a 2-month intensive phase, followed by a 4-month maintenance phase of rifampin and isoniazid, which is extended to 10 months if there is evidence of skeletal and/or central nervous system involvement [3].
The patient had a quite remarkable past medical history. He was a 76-year-old undernourished, heavy smoker who had been previously diagnosed and treated for two different malignancies. These conditions are known to be risk factors for developing tuberculosis [1,5]. Rare cases of TB on the scalp have been previously reported in medical literature and most of them presented as scalp swelling associated with calvarial disease or verrucous lesions [19-22]. The clinical presentation and histological finding in this case were atypical. The presence of acid-fast bacilli on microscopic examination, concomitant pulmonary tuberculosis and the response to multidrug therapy corroborated the diagnosis, which was confirmed by molecular testing and culture. He also had an osteolytic skull lesion located under the skin ulcer. Considering its location, it is reasonable to affirm it was very likely to be calvarial involvement of TB by contiguous spread, and the plan was to treat him for 12 months with combination therapy. An important differential diagnosis would be a cancer-related metastatic osteolytic lesion [23].
In conclusion, this case highlights the importance of tuberculosis as a differential diagnosis in dermatological, respiratory and skeletal conditions, especially considering its high prevalence around the world. Its potential to cause a wide variety of clinical presentations imposes a real diagnostic challenge.
Conflicts of interest
None
Funding
None
Consent for publication
The patient’s written consent for publication was obtained prior to data collection.
REFERENCES
[1] World Health Organization. Global Tuberculosis Report 2020. Retrieved from https://www.who.int/teams/global-tuberculosis-programme/tb-reports [Last accessed Mar 08, 2020].
[2] Oliveira SP, Silveira JTPD, Beraldi-Magalhães F, Oliveira RR, Andrade L, Cardoso RF. Early death by tuberculosis as the underlying cause in a state of Southern Brazil: Profile, comorbidities and associated vulnerabilities. Int J Infect Dis. 2019; 80S, S50-7.
[3] Ministry of Health of Brazil. Manual de recomendações para o controle da tuberculose no Brasil 2ª edição atualizada - 2019. Retrieved from http://www.aids.gov.br/pt-br/pub/2019/manual-de-recomendacoes-para-o- controle-da-tuberculose-no-brasil [Last accessed Mar 08, 2020].
[4] Tirado-Sánchez A, Bonifaz A. Cutaneous tuberculosis: A Review of the Current Literature. Curr Trop Med Rep. 2018; 5, 67l-6.
[5] Dobler CC, Cheung K, Nguyen J, Martin A. Risk of tuberculosis in patients with solid cancers and haematological malignancies: a systematic review and meta-analysis. Eur Respir J. 2017; 50 (2), 1700157.
[6] Schlesinger A, Paul M, Gafter-Gvili A, Rubinovitch B, Leibovici L. Infection-control interventions for cancer patients after chemotherapy: a systematic review and meta-analysis. Lancet Infect Dis. 2009; 9 (2), 97-107.
[7] Jacobs RE, Gu P, Chachoua A. Reactivation of pulmonary tuberculosis during cancer treatment. Int J Mycobacteriol. 2015; 4 (4), 337-40.
[8] Mazurek GH, Jereb J, Vernon A, et. al. Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection - United States, 2010. MMWR Recomm Rep. 2010; 25; 59 (RR-5), 1-25.
[9] Bruzzese E, Bocchino M, Assante LR, et al. Gamma interferon release assays for diagnosis of tuberculosis infection in immune-compromised children in a country in which the prevalence of tuberculosis is low. J Clin Microbiol. 2009; 47 (7), 2355-7.
[10] Santos JB, Figueiredo AR, Ferraz CE, Oliveira MH, Silva PG, Medeiros VL Cutaneous tuberculosis: epidemiologic, etiopathogenic and clinical aspects - Part I. An. Bras. Dermatol. 2014; 89 (2), 219-28.
[11] Dias MFRG, Bernardes FF, Quaresma MV, Nascimento LV, Costa Nery JA, Azulay DR. Update on cutaneous tuberculosis. An. Bras. Dermatol. 2014; 89 (6), 925-38.
[12] Lai-Cheong JE, Perez A, Tang V, Martinez A, Hill V, Menagé H du P. Cutaneous manifestations of tuberculosis. Clin Exp Dermatol. 2007; 32 (4), 461-6.
[13] Handog EB, Gabriel TG, Pineda RT. Management of cutaneous tuberculosis. Dermatol Ther. 2008; 21 (3), 154-61.
[14] Sethi A. Tuberculosis and infections with atypical mycobacteria. In: Fiztpatrick’s Dermatology, 9th ed, (Kang S, Amagai M, Bruckner AL, et al., Eds). McGraw-Hill Education; 2019: 2858.
[15] Handog EB, Ramam M, Gabriel MT, et al. Skin tuberculosis in South Asia, In: Asian Skin and Skin Diseases (Eun HC, Kim SC, Lee WS, Eds). MEDrang Inc, Korea; 2011: 349.
[16] Weedon D. Cutaneous infections and infestations - histological patterns. In: Weedon’s Skin Pathology, 3rd ed. Elsevier Limited; 2010: 544.
[17] Ramam M. How soon does cutaneous tuberculosis respond to treatment? Implications for a therapeutic test of diagnosis. Int J Dermatol. 2005; 44 (2), 121.
[18] Ramam M. What is the appropriate duration of a therapeutic trial in cutaneous tuberculosis? Further observations. Indian J Dermatol Venereol Leprol. 2007; 73 (4), 243.
[19] Zegmout A, Souhi H. Tuberculosis of the scalp: the tubercle bacilli has not ceased to surprise us. Pan Afr Med J. 2017; 28, 28.
[20] Dawar P, Satyarthee GD, Sharma BS. Total resolution of large scalp swelling due to calvarial tuberculosis with medical management only: case report and review of the literature. Turk Neurosurg. 2015; 25 (2), 313-6.
[21] Raut AA, Nagar AM, Muzumdar D, et al. Imaging features of calvarial tuberculosis: a study of 42 cases. AJNR Am J Neuroradiol. 2004; 25 (3), 409-14.
[22] Akpınar A, Erdoğan U, Koçyiğit M. Primary Calvarial Tuberculosis Presenting with Scalp Swelling and Lytic Bone Lesion: A Case Report. Med Bull Haseki. 2018; 56, 240-3.
[23] Subramanian S, Viswanathan VK. Lytic Bone Lesions. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. Available at: https://www.ncbi.nlm.nih.gov/books/NBK539837/ [Last accessed 09 March 2021].