Le Infezioni in Medicina, n. 2 , 259-262, 2021
CASE REPORTS
Severe systemic thrombosis in a young COVID-19 patient with a rare homozygous prothrombin G20210A mutation
Jose Ramon Fiore1, Marianna Ciarallo1, Mariantonietta Di Stefano1,3, Salvatore Sica1, Mariagrazia Scarale2, Maria D’Errico1, Fabio Corallo2, Sergio Lo Caputo1, Maurizio Margaglione3, Teresa Santantonio1
1Department of Clinical and Experimental Medicine, Infectious Diseases Unit, University of Foggia, Foggia, Italy;
2”Ospedali Riuniti” University Hospital, Section of Radiology, Foggia, Italy;
3Department of Clinical and Experimental Medicine, Section of Genetics, University of Foggia, Foggia, Italy
Corresponding author
Jose Ramon Fiore
E-mail: jose.fiore@unifg.it
SummaRY
COVID-19 patients may experience a hypercoagulable condition, leading to thrombotic events. We describe a patient with COVID-19, carrying a rare homozygous mutation of the prothrombin gene, who developed a severe systemic vein thrombosis. In COVID-19 patients with hypercoagulability disorders the most common inherited and acquired risk factors should be investigated.
Keywords: COVID -19, thrombosis, mutation.
INTRODUCTION
COVID-19 is a systemic illness that involves several systems beyond the respiratory tract [1, 2]. This wide range of clinical manifestations is explained by the presence of angiotensin converting enzyme 2 (ACE2) in various organs. Moreover, infection and activation of endothelial cells is thought to be the primary driver for the increasingly recognized complication of thrombosis [3,4]. According to many reports, in fact, COVID-19 exposes patients to a particularly high risk for venous thromboembolism. Hence, hospitalized COVID-19 patients are generally treated with low-molecular-weight heparin for thromboprophylaxis.
No information is still available regarding the possible role of preexisting inherited prothrombotic conditions in influencing thrombosis during COVID 19 infection.
Herein, we report for the first time a case of severe systemic thrombosis in a young COVID-19 patient with a rare homozygous prothrombin G20210A mutation.
CASE PRESENTATION
The patient, a 31-year-old Caucasian, went to the Emergency Room in October 2020 for suffering of fever and dry cough for ten days and abdominal and back pain for five days. The chest X-ray showed small opacities in the left lower lobe. A nasopharyngeal swab for SARS-CoV-2 RT PCR yielded a positive result and the patient was admitted to the Infectious Disease Clinic with a diagnosis of COVID-19. On admission, the patient presented fever (38.5°C), heart rate of 98 beats per minute, respiratory rate of 25 breaths per minute and 92% oxygen saturation in ambient air. Chest auscultation revealed basal crackles in both lungs. No relevant signs were observed at the abdominal level.
Baseline laboratory tests showed increased levels of serum fibrinogen (536 mg/dl; normal values: 200-450 mg/dl), D-dimers (31,700 ng/ml; normal values: 0-500 ng/ml), C-reactive protein (96 mg/L; normal values: 0-2 mg/L), prothrombin time (a-PTT) was of 40 seconds (normal values: 25.6 to 38.4 seconds and International normalized ratio (INR) was 1.4 (normal values: 0.80-1.20)
The patient received ceftriaxone (2 g, daily), dexamethasone (6 mg, daily), enoxaparin (4000 UI, daily), remdesivir (200 mg initial dose and 100 mg/die for 4 days thereafter) and supplemental oxygenation (FiO2 31% at 8 l/min, with Venturi mask).
Due to the persistence of the abdominal and back pain, the next day the patient underwent a thoraco-abdominal computed tomographic (CT) scan with iodine contrast. An opacification defect, attributable to thromboembolism, was evidenced in the main branches of the pulmonary artery and in particular of the tributary branch for the lower left lobe and for the lower and middle right lobes and common left iliac vein thrombosis (Figure 1). Heparin dose was then increased to 8.000 U.I. bid and hypercoagulability tests for acquired and inherited conditions were requested.
The presence of mutations in Factor V Leiden (FVL G1691A), in the prothrombin gene (PTR G20210A) along with the presence of anti-phospholipid antibodies (aPL) in plasma, conditions associated with an increased tendency to thrombosis, were evaluated.
Lupus anticoagulant (LAC) activity was measured using a dilute Russell’s Viper Venom Time test (dRVVT), while a Genexpert Assay (Genexpert, HemosIL FII&FV Cepheid), was used for FVLG169A and PTR G20021A nucleotide polymorphisms [5].
Our results for thrombophilia revealed the presence of a homozygous prothrombin G20210A (G20210A/G20210A) mutation and an associated antiphospholipid syndrome. No mutations in FVL were found. All the other thrombophilic parameters analyzed in plasma sample, as antithrombin, protein C, protein S were in the normal level range.
The presence of the G20210A mutation is a rare condition (especially in homozygosis). It is due to a single missense mutation (guanine to adenine, G >A) in nucleotide position 20210. It does not affect molecular conformation or functional activity of prothrombin but increases its levels in blood, that may lead to an imbalance between the procoagulant, anticoagulant and fibrinolytic system, resulting in a hypercoagulability and an increased risk of thrombosis [6]. The patient clinically improved after three days from admission and fever disappeared after one week. D-dimer levels progressively decreased to normal levels in 15 days (9.000 ng/ml, 1100 ng/ml and 420 ng/ml at 5, 10 and 15 days) and CRP decreased at 53 mg/l, 12 mg/L and 6.5 mg/L at 5, 10 and 15 days.
Now the patient is followed in the out-patient section and treated with oral anticoagulants (Warfarin); this treatment will be kept for life (INR target required 2.5-3.5).
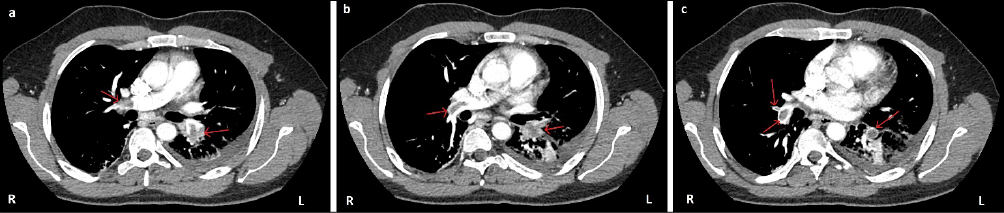
Figure 1 - Axial CTPA (computed tomography pulmonary angiogram). Filling defects in the pulmonary arteries bilaterally with a triangular shaped peripheral consolidation of lung parenchyma in the left inferior lobe as a result of lung infarction secondary to pulmonary embolism. The large embolus draped over the right pulmonary artery bifurcation is non-occlusive.
Pulmonary emboli in the right main pulmonary artery (left arrows in a and b);
Pulmonary emboli in the right middle (left superior arrow in c) and lower lobar branches (left inferior arrow in c);
Pulmonary emboli in the left lower lobe branch (right arrows in a, b and c).

Figure 2 - Coronal CTPA (computed tomography pulmonary angiogram).
Pulmonary emboli in the right lower lobar branches (left arrow in a);
Pulmonary emboli in the left lower lobe branch (right arrows in b).
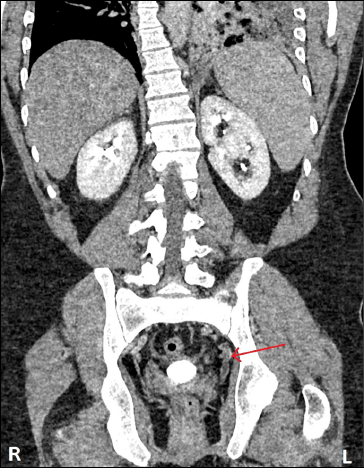
Figure 3 - Coronal CECT (contrast-enhanced CT), portal venous phase. CT image shows thrombus expanding in the left internal iliac vein.
DISCUSSION
This is, at the best of our knowledge, the first report of a case of severe systemic thrombosis in a young COVID-19 patient carrying a rare mutation associated with increased risk of thrombotic events.
The prevalence of homozygous PRT G20210A varies between different ethnic groups between 0-0.07% (6) and it is a recognized as an independent risk factor for thrombotic events [7]. Moreover, lupus anticoagulants and anticardiolipin antibodies have been associated with the risk of thrombosis in infected patients [8-10].
It is conceivable that in our patient the presence of homozygous in PRT G20210A as well as the presence of lupus anticoagulant had an important role in inducing and worsening thrombotic events.
Several mechanisms are proposed as responsible for thrombosis in COVID-19 infection: intracellular presence of SARS-CoV-2 may lead to direct endothelial injury causing microthrombotic phenomena. As well, the so termed “cytokine storm” may induce, through increased levels of TNF-a, IL-1 and IL-6, a procoagulant state and the activation of the coagulation cascade. Complement-mediated microvascular injury may also play a role.
Several inherited conditions may cause a hypercoagulable status: Factor V Leiden, deficiencies of natural proteins that prevent clotting (such as antithrombin, protein C and protein S), elevated levels of homocysteine, elevated levels of fibrinogen or dysfunctional fibrinogen dysfibrinogenemia, elevated levels of factor VIII (still being investigated as an inherited condition) and other factors including factor IX and XI, abnormal fibrinolytic system, including hypoplasminogenemia, dysplasminogenemia and elevation in levels of plasminogen activator inhibitor [11-13].
It is, however, not well known whether these pre-existing conditions may eventually trigger thrombotic events in COVID-19 patients.
In the setting of vaccination, in view of the reported cases of thrombosis after vaccine administration, concerns were arisen regarding safety. There is no evidence that individuals with a prior history of thrombosis or known risk factors for thrombosis are more at risk of developing this condition. In addition, for the majority of individuals, the risk of recurrent thrombosis due to COVID19 infection seems far greater than the risk of this syndrome. However, many questions are still unanswered [14].
Our observation, along with these considerations, suggests that the role of the most common inherited and acquired risk factors for hypercoagulability disorders in COVID-19 pathogenesis should be deeply investigated.
REFERENCES
[1] Siordia J.A. Epidemiology and clinical features of COVID-19: A review of current literature. J Clin Virol. 2020; 127, 104357.
[2] Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. 2021; 19 (3), 141-54.
[3] Hanff TC, Mohareb AM, Giri J, Cohen JB, Chirinos JA. Thrombosis in COVID-19. Am J Hematol. 2020; 95, 1578-89.
[4] Nopp, S, Moik, F, Jilma, B, Pabinger, I, Ay, C. Risk of venous thromboembolism in patients with COVID-19: A systematic review and meta-analysis. Res Pract Thromb Haemost. 2020; 4, 1178-91.
[5] Gessoni G, Valverde S, Canistro R, Manoni F. GeneXpert in the diagnosis of risk factors for thrombophilia: evaluation of its use in a small laboratory. Blood Transfus. 2012; 10, 228-9.
[6] Dziadosz M and Baxi LV. Global prevalence of prothrombin gene mutation G20210A and implications in women’s health: a systemic review. Blood Coagul. Fibrinol. 2016; 27, 481-9.
[7] Shemesh A, Hoffman R, Nadir Y. et al. Clinical significance of prothrombin G20210A mutation in homozygous patients. Am J Hematol. 2017; 92, E618-20.
[8] Sandor S. Shapiro, M.D. The lupus anticoagulant/antiphospholipid syndrome. Ann Rev Med. 1996; 47, 533-53.
[9] Harzallah I, Debliquis A, Drénou B. Lupus anticoagulant is frequent in patients with Covid-19. J Thromb Haemost. 2020; 18, 2064-5.
[10] Bowles L, Platton S, Yartey N, et al. Lupus anticoagulant and abnormal coagulation tests in patients with Covid-19. N Engl J Med. 2020; 383, 288-90.
[11] Kichloo A, Dettloff K, Aljadah M. et al. COVID-19 and Hypercoagulability: A Review. Clin Appl Thromb Hemost. 2020 Jan-Dec; 26, 1076029620962853.
[12] Singhania N, Bansal S, Nimmatoori DP, Ejaz AA, McCullough PA, Singhania G. Current overview on hypercoagulability in COVID-19. Am J Cardiovasc Drugs. 2020; 20 (5), 393-403.
[13] Giudice V, Filippelli A, Selleri C. Can we Turn off the “Covid-Biting-Tail” Inflammation? Transl Med UniSa. 2020; 23, 39-41.
[14] Ledford H. COVID vaccines and blood clots: five key questions. Nature. 2021; 592, 495-6.