Le Infezioni in Medicina, n. 2 , 252-258, 2021
ORIGINAL ARTICLES
Lesson learned from the 2017 measles outbreak in Italy: report from an emergency department
Ornella Spagnolello1,2, Alessandro Russo3,4, Cristian Borrazzo2, Gabriella d’Ettorre2, Giancarlo Ceccarelli2
1Emergency Department, University of Rome Sapienza, Rome, Italy;
2Department of Public Health and Infectious Diseases, University of Rome Sapienza, Rome, Italy;
3Department of Public Health and Infectious Diseases, University of Pisa, Pisa, Italy;
4Department of Public Health and Infectious Diseases, Policlinico Casilino Hospital, Rome, Italy
Corresponding author
Ornella Spagnolello
E-mail: spagnolello.ornella@gmail.com
SummaRY
Measles is a preventable disease still responsible for a number of outbreaks worldwide. Although most adults with measles recover uneventfully, measles-related complications may occur. However, as to whether every complicated case requires hospital management is still a point of debate. In this study we described the rate, clinical features and severity of measles complications in patients admitted to the ED of a tertiary-care teaching hospital during the outbreak that took place in 2017. Some insights into the impact on the health care system are reported as well. A retrospective cohort study was performed. Medical records of adults discharged from January to December 2017 with diagnosis of “measles” were collected and analyzed. Out of 58,579 of ED admissions, 162 measles cases were enrolled. Acute measles infection was laboratory confirmed in 71.6% and deemed as possible/probable in 24.0% of cases. Three percent of patients were immunocompromised while 1.2% of cases occurred in pregnant women. Of all complications reported (37%), hepatitis was the most frequent (29%) followed by pneumonia (10.4%), keratitis (3.8%), thrombocytopenia (3.8%) and otitis media (0.6%). No significant clinical and laboratory difference emerged between complicated and non-complicated cases besides antibiotic prescription (80.0% vs 66.3%; p=0.039). The course of the disease was mild, and no life-threatening measles-related complications or critical care support were reported. One out of three measles cases may experience at least one measles-related complication. However, the course of the disease seems to be rather benign in young adults, and the widespread use of the ED and hospitalization observed seem an inappropriate approach to the issue.
Keywords: Measles outbreak, measles-related complications, emergency department, public health.
INTRODUCTION
Measles is a highly infectious disease recently emerged as a worldwide public health issue. It has been estimated that the chance of contracting the disease in exposed not immune people add up to 90%, and that each case of measles may in turn infect up to 9 to 18 susceptible individuals [1].
In 2017, the World Health Organization (WHO) European Region experienced a dramatic resurgence of measles which involved particularly unvaccinated young adults [2]. Among European countries, Italy ranked second in terms of number of cases reported (5,098), right behind Romania (5,608) and followed by Greece and Germany (967 and 929, respectively). In accordance with the National Integrated Measles-Rubella Surveillance Report of 2017 (published by the Italian National Health Institute), although 35.8% of measles cases were affected by at list one complication, only 4 deaths were eventually notified [3].
Currently, a number of studies have reported a wide and often unjustified access to the emergency care facility over measles outbreaks, frequently leading to prolonged hospitalisation weighing considerably on the health care system [4-6].
Despite in the large majority of adult patients the course of the disease is favorable, measles may occur in various clinical manifestations and is potentially responsible of a high burden of complication (such as pneumonia, encephalitis, elevated serum transaminases, creatinine or amylase and lipase), the risk of which partially explains the frequent recourse of the emergency facility and hospitalisation [7].
The aim of this study is to retrospectively assess the rate, the clinical features and the severity of measles complications in patients admitted to the ED of the larger Teaching Hospital in Rome (Italy) during the outbreak of 2017, and to provide some insight into the impact on the health care system.
PATIENTS AND METHODS
Study design and population
From January to December 2017 a retrospective cohort study was performed. Clinical records of all adult (≥18 years) discharged with final diagnosis comprehensive of measles were retrospectively collected. Only clinical records properly provided by clinical, laboratory and radiological examinations were analysed. Patients subsequently deemed to be measles-free in accordance with IgM/IgG assessment results and patients with duplicate records were excluded from the study.
The measles case definition was based on the Italian Ministerial Criteria and the European Commission case definition [8, 9]. A possible case was identified as any patients meeting clinical criteria including fever, maculopapular rash and at list one of the following minor criteria: conjunctivitis, coryza or cough. A probable case was defined as patients meeting both clinical criteria and an epidemiological link to a laboratory-confirmed case. A confirmed case was any case with laboratory evidence of measles virus acute infection.
All procedures were performed at the request of the ED, in accordance with internal health management protocol. The study was carried out in accordance with the Helsinki Declaration and data were gathered and analysed following informed consent. Since the study was based on a retrospective analysis of data routinely collected and stored according to the Italian law on privacy [General authorisation to process personal data for scientific research purposes granted by the Italian Data Protection Authority (1 March 2012 as published in Italy’s Official Journal no. 72 dated 26 March 2012)] ethical approval was not required. The study complies with the indications of STROBE Statement - checklist.
Study procedures
Each clinical record covered demographic and anamnestic data, along with clinical, laboratory and radiological examinations performed during ED staying.
Laboratory assessment included both routine blood analysis and specific IgM/IgG antibodies detection by enzyme linked immuneassorbent (ELISA) assay from venous blood sample. Each patient underwent chest X-ray and special visit by infectious diseases specialist consultant.
Quick Sequential Organ Failure Assessment (qSOFA) and Charlson Co-morbidity Index (CCI) scores were calculated according to international criteria and analysed.
Complications related to acute measles infection considered were, namely: pneumonia, hepatitis, keratitis, otitis media, myocarditis, thrombocytopenia and neurologic complications. In accordance with previously published international guidelines, pneumonia was defined as the presence of new infiltrates on chest X-rays together with clinically compatible signs and symptoms [10-12]. Hepatitis complicating measles was defined as a rise of liver enzymes at least up to 5-fold the normal range. Thrombocytopenia was defined as a platelet count below 100 x 109/L. Acute neurologic complications included encephalitis and acute disseminate encephalomyelitis.
Statistical analysis
Description of median with interquartile range (IQR: 25%-75%), Mean ± Standard Deviation (SD), simple frequencies (n), proportions and rates of the given data on each variable was calculated.
The demographic characteristics of subjects were compared using Mann-Whitney test or two-tailed student t-test after acceptance of normal distribution with the Kolmogorov-Smirnov test. Categorical variables were compared using Fisher’s exact tests or chi-square test statistics.
The Positive Predictive values (PPV) and Confidence Interval (CI) 95% was calculated to evaluate the proportions of a true positive results.
A p-value of less than 0.05 was considered statistically significant. The statistical Package for the Social Science (SPSS) version 22 was used for statistical analysis.
RESULTS
Description of the study population
In the study period, out of 58,579 ED admissions, 218 medical records with final diagnosis code of either “measles” or “measles suspicion” were collected. Of them, along with 5 incomplete clinical records, 56 patients were subsequently deemed to be measles-free and consequently excluded from our analysis.
Of the 162 measles cases finally enrolled, acute measles infection was laboratory confirmed in 71.6% (n=116) of cases and eventually deemed as either possible or probable in 24.0% (n=39) of patients. During the study period, the highest incidence of measles cases was reported in July (29.7%; n=46) whereas the lowest in October (17%; n=26).
Demographic characteristics of the study population are reported in Table 1. Median age was 31.5 years (IQR: 25.9-38.6) and 55.5% (n=86) were female. Almost all cases (98.7%; n=153) were under 65 years of age. The co-morbidities weight among the study population was rather low (CCI 0.5±0.6 points). In particular, only 2.4% (n=4) were affected by chronic respiratory diseases including both Chronic Obstructive Pulmonary Disease (COPD) and asthma, whereas 3.0% (n=5) were immunocompromised [1.8% (n=3) reported active cancer and 1.2% (n=2) HIV infection]. 1.2% (n=2) of measles cases occurred in pregnancy.
Table 1 - Demographic characteristics of the study population.
|
Study Population, n (%) |
162 |
|
Age, median (IQ) |
31.5 (25.9-38.6) |
|
Sex, female, n (%) |
86 (55.5%) |
|
Co-morbidities: |
|
|
COPD, n (%) |
4 (2.4%) |
|
Asthma, n (%) |
5 (3%) |
|
Active Cancer, n (%) |
3 (1.8%) |
|
HIV infection, n (%) |
2 (1.3%) |
|
CKD, n (%) |
-- |
|
Ictus/TIA, n (%) |
-- |
|
CHF/IM, n (%) |
-- |
|
DM, n (%) |
4 (2.6%) |
|
CCI, mean (SD) |
0.5±0.6 points |
|
Smoke, n (%) |
2 (1.3%) |
|
Pregnancy, n (%) |
2 (1.3%) |
COPD = Chronic Obstructive Pulmonary Disease; HIV = Human immunodeficiency virus; CKD = Chronic Kidney Disease; TIA = Transient Ischemic Attack; CHF/MI = Chronic Heart Failure/Myocardial Ischemia; DM = Diabetes Mellitus; CCI = Charlson Comorbidity Index.
Measles-related complications rate, clinical features and severity
Complications were reported in 37% (n=60) of cases. Hepatitis was the most frequent complication (29%; n=45) followed by pneumonia (10.4%; n=17), keratitis (3.8%; n=6) and thrombocytopenia (3.8%; n=6) (Figures 1 and 2). Hepatitis and pneumonia, both in mild presentation, were the most common measles-related complications observed in our study population whereas no life-threatening complications, including myocardial and neurologic, were reported.
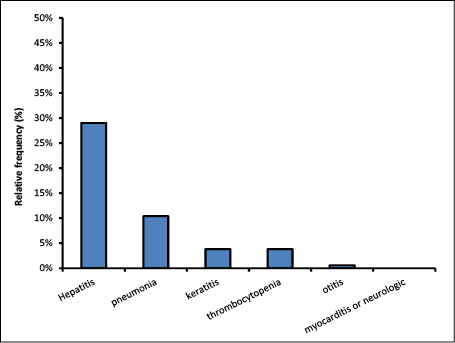
Figure 1 - Measles-related complications rate: listed for type of complication.
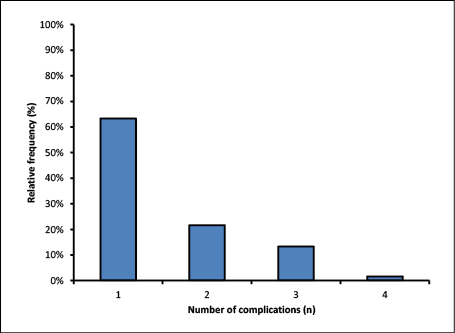
Figure 2 - Measles-related complications rate: listed for number of complications.
We observed only one case of otitis media (0.6%; n=1) and none of myocarditis or neurologic complications. The highest frequency of complications was seen in the age group of median 31 (IQR: 24.8-39.3).
At ED admission, 96.8% (n=150) of patients reported fever and maculopapular rush, 54.9% (n=89) conjunctivitis, 57.4% (n=93) cough and 6.8% (n=11) presented coryza. From a clinical point of view, the majority of patients received a qSOFA score of 0 (80%; n=124) whereas a score of 1 or 2 was assigned in 16.8% (n=26) and 3.2% (n=5) of cases, respectively.
Although only 11.1% (n=18) of complicated cases were consistent with bacterial superinfection (17 pneumonia and 1 otitis media), antibiotic therapy was prescribed in 68.5% of all cases (n=111).
No life-threatening measles-related complications were reported and no patient experiencing at list one measles complication ended up to require critical care support, defined as either ventilation or vasopressor/inotropic support. All cases of hepatitis reported a mild elevation of liver enzymes without any signs of acute hepatic failure. None of measles cases complicated by pneumonia required ventilation support, and only a few of them were given oxygen by nasal canula. Among the six cases of thrombocytopenia, platelets blood count never dropped below 48 x 109/L and no bleeding events were reported at all.
Overall, 57.4% (n=93) of cases were hospitalised but no ICU admission was recorded. Of them only 38.7% (n=36) were measles-related complicated cases.
Comparison between two groups: patients
with measles-related complications versus patients complication-free
No significant differences in terms of either age or sex was observed between the two groups. Similarly, the co-morbidities level, including chronic respiratory diseases or immunosuppression, was equally distributed among the two groups (Table 2). Notably, none of the two persons leaving with HIV included in our analysis experienced any complications. Although the time course from symptoms onset to ED admission was rather comparable, patients without measles-related complications were keener on skipping general practitioner contact in comparison to patients with complications (74% vs 55%; p=0.031). At clinical evaluation, although no difference in terms of qSOFA score was reported among the two groups, more patients with measles-related complications experienced cough than others (70.0% vs 53.7%; p=0.046). Any difference in routine blood analysis (as creatinine, total CPK, WBC, neutrophils, leukocytes, platelets and liver enzymes) including CPR came up among the two groups. Concerning treatment, more patients with measles-related complications were given antibiotic therapy than others (80.0% vs 66.3%; p=0.039). No difference in terms of neither median time of ED staying or admission rate were reported between the two groups.
Considering only patients with measles-related pneumonia, no difference in terms of age, sex and co-morbidities level still stood out. In particular, pneumonia cases occurred in patients free from any chronic respiratory diseases. Time course from symptoms onset to ED admission and the rate of patients skipping general practitioner contact did not differ between the two groups. From a clinical point of view, the qSOFA score did not point out any difference as well. Despite no difference in terms of CPR levels, the mean level of both WBC (6.32±2.71 vs 4.65±1.71; p=0.033) and neutrophils (5.22±2.37 vs 3.63±1.53; p=0.022) was significantly higher in patients with measles-related pneumonia. Antibiotic therapy was given in more patients with measles-related complications in comparison to others (9% vs 68.8%; p<0.001). However, no difference in terms of neither median time of ED staying or admission rate came up between the two groups.
Table 2 - Comparison among groups: patients with measles-related complications and patients complication-free.
|
Patients with measles-related complications |
Patients complication-free |
p-value |
|
|
No (%) |
60 (37.0) |
102 (63.0) |
-- |
|
Age, median (IQ) |
32.0 (27.0-38.0) |
34.5 (26.8-49.5) |
0.111 |
|
Sex, female, n (%) |
23 (38.3) |
63 (61.7) |
0.003 |
|
Co-morbidities: |
|||
|
COPD, n (%) |
3 (5%) |
1 (1%) |
0.115 |
|
Asthma, n (%) |
1 (1.6%) |
4 (3.9%) |
0.412 |
|
Active cancer, n (%) |
1 (1.6%) |
2 (1.9%) |
0.890 |
|
HIV infection, n (%) |
0 (0%) |
2 (1.9%) |
0.284 |
|
CKD, n (%) |
0 (0%) |
0 (%) |
1.000 |
|
Ictus/TIA, n (%) |
0 (0%) |
0 (%) |
1.000 |
|
CHF/MI, n (%) |
0 (0%) |
0 (%) |
1.000 |
|
DM, n (%) |
3 (5%) |
1 (1%) |
0.115 |
|
CCI, mean (SD) |
0.4±0.68 |
0.14±0.39 |
0.117 |
|
Smoke, n (%) |
1 (1.6%) |
1 (1%) |
0.738 |
|
Pregnancy, n (%) |
1 (1.6%) |
1 (1%) |
0.738 |
|
Laboratory findings: |
|||
|
WBC, mean (SD) |
6.32±2.7 |
4.65±1.71 |
0.033 |
|
Neutrophils, mean (SD) |
5.22±2.37 |
3.63±1.53 |
0.022 |
|
Lymphocytes, median (IQ) |
0.5 (0.3-0.6) |
0.6 (0.4-0.8) |
0.777 |
|
Platelets, median (IQ) |
141 (111.5-172) |
159 (126.5-187.5) |
0.345 |
|
Creatinine, median (IQ) |
0.8 (0.6-0.9) |
0.7 (0.6-0.9) |
0.208 |
|
Total CPK, median (IQ) |
161.5 (83.5-342.5) |
118 (66-395) |
0.469 |
|
ALT, median (IQ) |
81 (34.5-217.5) |
136 (103.5-215) |
0.810 |
|
qSOFA, median (IQ) |
0 (0-2) |
0 (0-2) |
0.465 |
|
Antibiotic Therapy, n (%) |
56 (94.1%) |
70 (68.8%) |
<0.001 |
|
Out-of-hospital medical contact, n (%) |
6 (10%) |
40 (39.2%) |
<0.001 |
|
Hospitalisation, n (%) |
12 (20%) |
81 (78.4%) |
0.250 |
|
Return to the ED, n (%) |
5 (8.3%) |
30 (29.4) |
0.001 |
COPD = Chronic Obstructive Pulmonary Disease; HIV = Human immunodeficiency virus; CKD = Chronic Kidney Disease; TIA = Transient Ischemic Attack; CHF/MI = Chronic Heart Failure/Myocardial Ischemia; DM = Diabetes Mellitus; CCI = Charlson Comorbidity Index; WBC = White Blood Cells; CRP = C-Reactive Protein; CPK = Creatinine Phosphokinase; ALT = Alanine Aminotransferase.
Impact on public health system
Overall, only 29% (n=47) of cases reported a previous contact with the general practitioner and the median time from symptoms onset to ED admission was 5 days (4.3-6.5). Of them, 55.3% (n=26) subsequently reported at list one measles complication. No remarkable difference in terms of age, sex or co-morbidities was observed among patients reporting a previous general practitioner contact. On the other hand, the time course from symptoms onset to ED admission was significantly longer in this group in comparison to others (5.8±1.69 vs 5.11±2.38; p=0.049). Any significant difference in either routine blood analysis or complication rate turned out among the two groups. Concerning treatment, patients reporting a previous general practitioner contact were significantly more likely to be given antibiotic therapy than others (80.8% vs 65.7%; p=0.004). No difference in terms of neither median time of ED staying or admission rate were reported between the two groups.
Only 2.4% of cases (n=4) occurred among healthcare workers (HCW) and all of them concerned young medical or nursing staff involved into a training program.
Although vaccination status was mostly unknown (88.2%; n=143), 3.7% (n=6) were fully vaccinated whereas 1.8% (n=3) had received only one dose of measles containing vaccine.
DISCUSSION
Although the rate of complications occurred in the nationwide measles outbreak of 2017 has been properly reported by the Italian National Institute of Health, to the best of our knowledge no study addressed the issue from the ED point of view, with the purpose of running through the overrated severity of measles-related complications. This study aimed to assess the rate, the clinical features and the severity of measles complications in patients admitted to the ED of our Teaching Hospital during the outbreak of 2017.
In tune with the National Integrated Measles-Rubella Surveillance Report of 2017, the number of measles-related complicated cases among all patients enrolled in our study added up to 37.0% [2]. Hepatitis ranked as the most frequent complication reported (29%), followed by pneumonia (10.4%), keratitis (3.8%) and thrombocytopenia (3.8%). Moreover, we observed only one case of otitis media and none of myocarditis or neurologic complications.
Despite the high rate of complication observed, the most striking data outlined by our study regards the favorable outcome of measles-related complicated cases. As a matter of fact, the course of disease was fairly mild and no life-threatening complications occurred and none of all patients enrolled required neither critical care support or ICU admission. From a clinical point of view, no difference in terms of clinical or laboratory features came out between complicated and uncomplicated measles cases.
According to our data, measles cases admitted to our ED during the outbreak of 2017 were rather young and free from remarkable co-morbidities. Despite the concern of potential severe measles complication might have been advocated in immunocompromised individuals, in patients with chronic respiratory disease or in pregnant women, less than 9% of measles cases enrolled in our study were eventually deemed to be at high risk. This can be explained by the evidence that people with pathophysiological situations at risk for developing severe measles complications are generally target of awareness and preventive vaccination campaigns by caregivers: therefore, it is relatively rare that they are lacking in immune protection. Nevertheless, a special attention should be given to immunosuppressed people and pregnant women who are known to be exposed to the greatest risk of both severe and atypical measles complication.
Taken all together, this data underlines how even patients suffering from measles-related complication are fairly unsuitable to be managed into the hospital setting. Moreover, in accordance with the British Measles Guidelines published in 2017, our results suggested that, apart from immunocompromised individuals and pregnant women, the co-morbidities background should not necessarily point as to whether admit measles cases to ED [13].
In accordance with data previously published, we observed an over prescription of antibiotics (68.5% of the population enrolled) despite the low frequency of bacterial superinfection. This trend was particularly noticeable in patients reporting a previous general practitioner contact. However, some factors should be taken on board in a bid to explain this poor attitude: firstly, the lack of national guidelines in measles management had been drafted in advance with the purpose of reducing the impact on public facilities; secondly, the lack of familiarity with the disease of many general practitioners, because of its previous low rate of occurrence.
Surprisingly, despite vaccination program has recently been a great point of debate in Italy, vaccination status was largely unknown among measles cases. The knowledge of one’s vaccination history, on the contrary, might have driven susceptible people to fulfil the gaps during the 1-year long outbreak and would have supported physicians in differential diagnosis. This interesting data outline the crucial role of the general practitioner in providing health education to patients along with promoting vaccination coverage.
Finally, our study showed that less than a third of measles cases reported a previous contact with the general practitioner. Despite a number of reasons may explain this stunning data, running from the impact of social media to the lack of trust in primary healthcare professionals, we strongly believe that general practitioners must bridge the gap in health education spreading across the country in order to tackle unnecessary ED admissions. In fact, patients without measles-related complications were keener on skipping general practitioner contact in comparison to patients with complications reflecting a poor confidence in primary healthcare professionals regardless of the course of disease severity.
This study had several limitations: first of all, the present report analysed only short-term complication but no information about long-term complications, such as subacute sclerosing panencephalitis (SSPE), were available. On the other hand, this data does not directly affect the hospitalisation of patients with measles, in fact, the SSPE is an extremely rare event occurring essentially during childhood that may affect fully recovered patients in the long run. Secondly, given the young and rather healthy population nowadays affected by measles, the impact of co-morbidities on measles complications occurrence could not be clearly outlined in our study. The number of immunocompromised individuals and pregnant women enrolled was low as well, possibly because of the special attention to vaccination campaign among this susceptible population.
CONCLUSIONS
One out of three measles cases may experience at least one measles-related complication. However, although special attention must be reserved over immunocompromised individuals and pregnant women, the course of disease seems to be rather benign in young adults, regardless of complication occurrence and the widespread use of the ED and hospitalization observed seem to be an undue approach to the issue.
To date, the vaccination campaign remains the most effective tool to prevent measles outbreak.
Conflict of interest
None declared.
Funding
None
REFERENCES
[1] Moss WJ. Measles. Lancet. 2017; 390 (10111), 2490-502.
[2] European Centre for Disease Prevention and Control. Measles and rubella surveillance - 2017. Stockholm: ECDC; 2018. https://www.ecdc.europa.eu/en/publications-data/annual-measles-and-rubella-monitoring-report-2017https://ecdc.europa.eu/en/publications-data/annual-measles-and-rubella-monitoring-report-2017 [accessed on 20/12/2020].
[3] Epicentro, Italian Institute of Health. Measles in Italy: weekly bulletin, Update as of 12 December 2017. http://www.epicentro.iss.it/problemi/morbillo/bollettino/Measles_WeeklyReport_N35eng.pdf [accessed on 20/12/2020].
[4] Ceccarelli G, Spagnolello O, Borrazzo C, et al. Impact of the 2017 measles outbreak on the emergency care system of a large tertiary-care teaching hospital in Italy: a retrospective analysis. Eur J Public Health. 2019; 29 (5), 966-71.
[5] Pezzotti P, Valle S, Perrelli F, et al. Measles outbreak in the Lazio region of Italy: surveillance and impact on emergency departments and hospitalizations. Ann Ig. 2013; 25 (4), 299-309.
[6] Suardi LR, Filippo Bartalesi F, Fusco FM, et al. Overuse of antimicrobials and over-hospitalization in an adult measles cluster in the Florence area during the ongoing Italian outbreak. Infection. 2018; 46 (6), 891-2.
[7] Stahl JP, Salmon D, Bruneel, F, et al. Adult patients hospitalized for measles in France, in the 21st century. Med Mal Infect. 2013; 43 (10), 410-6.
[8] Ministero della Salute: Piano nazionale per l’eliminazione del morbillo e della rosolia congenita 2010-2015. Approvato con Intesa Stato-Regioni 23 marzo 2011. http://www.salute.gov.it/imgs/C_17_pubblicazioni_1519_allegato.pdf [accessed on 4/11/2018].
[9] European Commission. Commission Implementing Decision of 8 August 2012 amending Decision 2002/253/EC laying down case definitions for reporting communicable diseases to the Community network under Decision No 2119/98/EC of the European Parliament and of the Council. Luxembourg: Publications Office of the European Union. L262 Sep 27, 2012. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32012D0506&from=en [accessed on 20/12/2020].
[10] Mandell LA, Wunderink RG, Anzueto A, et al. Infectious diseases society of America/American thoracic society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007; 44 (Suppl. 2), S27-72.
[11] American Thoracic Society: Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005; 171 (4), 388-416.
[12] Pneumonia in adults: diagnosis and management. NICE guidelines 2014. https://www.nice.org.uk/guidance/cg191 [accessed on 20/12/2020].
[13] PHE national measles guidelines. August 2017. https://www.gov.uk/government/publications/national-measles-guidelines [accessed on 20/12/2020].