Le Infezioni in Medicina, n. 1, 70-78, 2021
ORIGINAL ARTICLES
Diagnostic and infection control strategies for Clostridioides difficile infections in a setting of high antimicrobial resistance prevalence
Lorenzo Bertolino1, Fabian Patauner1, Massimo Gagliardi1, Fabiana D’Amico1, Valeria Crivaro2, Mariano Bernardo2, Isabella Scherillo3, Filomena Bellitti3, Caterina Cusano4, Rita Greco4, Vittorio Panetta4, Adriana Durante4, Alfonsina Di Caterino5, Angelo Frieri6, Grazia Cioffi7, Maria Nappo7, Mariano Corrado8, Michele Lanzieri8, Paola Sabatini8, Roberto Bettelli9, Rita dello Russo9, Maria Luisa Taddeo9, Rosalba Petrone10, Maria Giovanna Di Sevo10, Mariateresa Iannuzzo11, Mario Iervolino12, Raffaella Buonocore12, Federica D’Agostino12, Michele Gambardella13, Antonio De Martino14, Silvano Spagnuolo14, Marina Savarese14, Sabina Sole15, Carmela Russo16, Erminia Agozzino17, Massimiliano Galdiero17, Rosa Martino18, Rosa Calemma18, Antonio Sciambra19, Cristina Aprea19, Diego Colaccio20, Pasquale Di Guida21, Michele Venditti22, Emma Montella23, Francesco Guerriero24, Rita Perrotta24, Umberto Di Filippo25, Angelo Pizza26, Antonietta Di Fronzo27, Anna Lombardi27, Luigi Capuano28, Andrea De Stefano29, Angela Mastropietro30, Matilde Mastro31, Romolo Loffreda31, Luigi Maccarone32, Amelia Di Tora33, Savino Oto34, Carminantonio Tammaro34, Antonio Claudio Mondelli35, Maria Ruocco36, Biagio Ferraro36, Alfonso Petrosino37, Silvia S. A. Presta38, Emanuele Durante Mangoni1,39
1Department of Precision Medicine, University of Campania “L. Vanvitelli”, Naples, Italy;
2“Monaldi” Hospital, AORN Ospedali dei Colli, Naples, Italy;
3“Santa Maria delle Grazie” Hospital, Pozzuoli, Naples, Italy;
4A.O.U. “Sant’Anna e San Sebastiano”, Caserta, Italy;
5“San Giuseppe Moscati” Hospital, Aversa, Italy;
6“Sant’Angelo dei Lombardi” Hospital, Avellino, Italy;
7A.O.U.S. Giovanni di Dio e Ruggi d’Aragona, Salerno, Italy;
8“Umberto I” Hospital, Nocera, & DEA Nocera-Pagani-Scafati, Italy;
9“San Giuseppe Moscati” Hospital, Avellino, Italy;
10“Luigi Curto” Hospital, Polla, Italy;
11Fatebenefratelli Hospital, Naples, Italy;
12A.O. S. Pio, Benevento, Italy;
13“San Luca” Hospital, Vallo della Lucania, Italy;
14“San Paolo” Hospital, Naples, Italy;
15A.O. “Santobono Pausilipon”, Naples, Italy;
16A.O. Cardarelli, Naples, Italy;
17Dipartimento di Medicina Sperimentale, Università della Campania “L. Vanvitelli”, AOU della Campania “L. Vanvitelli”, Naples, Italy;
18Istituto NazionaleTumori-IRCCS “Fondazione G. Pascale”, Naples, Italy;
19Ospedale Evangelico Betania, Naples, Italy;
20“S. Giuseppe Melorio” Hospital, S. Maria Capua Vetere, Italy;
21“S. Alfonso Maria de Liguori” Hospital, S. Agata dei Goti, Italy;
22Fatebenefratelli Hospital, Benevento, Italy;
23A.O.U. “Federico II”, Naples, Italy;
24“Landolfi Solofra” Hospital, Solofra, Italy;
25“S. Francesco d’Assisi Hospital”, Oliveto Citra, Italy;
26Agropoli Hospital, Italy;
27“S. Giovanni di Dio” Hospital, Frattamaggiore, Italy;
28Rizzoli Hospital, Ischia, Italy;
29“Santa Maria della Pietà” Hospital, Casoria, Italy;
30Maddaloni Hospital, Italy;
31Piedimonte Matese Hospital, Italy;
32Marcianise Hospital, Italy;
33“San Rocco” Hospital, Sessa Aurunca, Italy;
34Ariano Irpino Hospital, Italy
35Roccadaspide Hospital, Italy
36“Dell’Immacolata” Hospital, Sapri, Italy
37“Maria SS. Addolorata” Hospital, Eboli, Italy
38“Santa Maria della Speranza” Hospital, Battipaglia, Italy
39Unit of Infectious & Transplant Medicine, AORN Ospedali dei Colli - Monaldi Hospital, Naples, Italy
Corresponding author
Emanuele Durante Mangoni
E-mail: emanuele.durante@unicampania.it
SummaRY
Clostridioides difficile (CD) is a major nosocomial pathogen and the leading cause of antibiotic-associated diarrhoea. In light of the strong association between antimicrobial use and CD infections (CDI), it may be hypothesised that areas at higher prevalence of antimicrobial resistance, like the region of Campania in southern Italy, could also have a higher rate of CDI. In this multicentre, region-based, prospective study, we analysed such issues, exploiting CDI incidence data collected from local hospitals. In 2016, the Italian National Centre for Disease Control supported a project involving three Italian regions: Friuli Venezia Giulia, Lazio and Campania. In Campania, a network of 49 hospitals willing to participate in the project was created. The project consisted of two phases: a survey on practice patterns concerning CDI and an epidemiological surveillance study. We identified a stringent need to improve awareness about CDI among the regional health-care community, as a widespread lack of surveillance programmes for CDI control was observed observed (existing in only 40% of participating facilities). Moreover, almost half of the participating hospitals (n=16, 43%) had no standardised procedures or protocols to control and prevent CDI. In the second phase of the study, we collected data of CDI cases during a six-month surveillance programme. In all, 87 CDI cases were observed, for a total of 903,334 patient bed-days and 122,988 admissions. According to the above data, CDI incidence was 0.96 cases/10000 patient bed-days, much lower than expected based on prior studies conducted elsewhere. The results of our study suggest CDI remains a rather neglected clinical issue in Campania. Despite a high burden of antimicrobial resistance and antimicrobial use in our geographic setting, we observed a very low incidence of CDI. Such a low incidence could be explained by underdiagnosis, but could also be related to actual diet, the lower patient age or the specific genetic background. However, further studies are warranted to either confirm or rebut the above hypotheses.
Keywords: Clostridioides difficile, antimicrobial resistance.
INTRODUCTION
Clostridioides difficile (CD) is a gram-positive, spore-forming, anaerobic enteric bacterium, present in an asymptomatic carrier state in a considerable share of the population (~7% in adults and 50% in children) [1]. Prevalence rates increase substantially among patients treated with antibiotics [1]. Indeed, CD is the leading cause of antibiotic-associated diarrhoea and is the causative agent of pseudomembranous colitis [2]. Although considered a major nosocomial pathogen, CD is also increasingly recognized as an important diarrheal agent in the community, not invariably associated with antibiotic therapy [3-5].
Symptomatic CD Infections (CDI) are caused by toxigenic strains, and show an extremely wide clinical spectrum, ranging from very mild forms of diarrhoea to moderate, severe, complicated or life-threatening disease [6]. The most common clinical features of CDI are diarrhoea (from minimal, self-limited disease to profuse, up to 20 movs/day), fever, abdominal pain, tenesmus, leukocytosis (up to leukemoid reactions with white blood cell counts >25.000-50.000/mm3) and acute kidney injury [2, 7].
In light of the potentially severe prognosis of the disease, clinicians have to adopt an active surveillance programme in order to promptly identify a CDI case. To achieve this task, it is important to systematically test patients with antibiotic-associated or healthcare-associated diarrhoea for C. difficile, paying additional attention to patients with specific risk factors, such as a close contact with a CDI case, frailty, disability or dependency [8, 9].
Microbiology laboratories should consider performing tests for CDI on all unformed stool samples (i.e. those that take the shape of the container) received from acute care hospitals, irrespective of the physician request [10]. Intuitively, solid stool samples should not be tested, as the absence of diarrhoea raises the possibility to detect asymptomatic C. difficile carriage. For patients with ileus, rectal swabs can be used for CDI testing [10]. Furthermore, there’s no test-of-cure assay recommended, as prolonged carriage of C. difficile may occur after clinical resolution of the diarrhoea [10].
The European Society of Clinical Microbiology and Infectious Diseases recommends combining two tests in a single algorithm in order to optimize the diagnosis of CDI. This is because there are no stand-alone tests whose reliability justifies use without a confirmation test. The algorithm includes a first step using a highly sensitive test, like Nucleic Acid Amplification Tests (NAATs) or Glutamate Dehydrogenase Enzyme Immune-Assay (GDH-EIA), both showing a high negative predictive value. In case of a positive result on one of these assays, CDI diagnosis needs to be confirmed by highly specific, second step test, such as the enzyme immune-assay detecting toxin A and B or the labor-intensive and complex cell cytotoxicity neutralization assay [10].
The correct approach to a patient with CDI also includes several basic infection control measures as employee hand hygiene (C. difficile spores are difficult to remove by washing with soap or disinfectants), gloves and gowns wearing for health care workers, isolation of patient in single bed rooms, use of disposable or dedicated thermometers, sphygmomanometers, stethoscopes, etc [11, 12]. In case of exposure to CD, some post-exposure and patient-directed measures can be taken, as well as a restricted access to specific antimicrobial agents (clindamycin, fluoroquinolones and cephalosporins) [13].
In light of the strong association between antimicrobial use and CDI, it is possible to hypothesise that areas at higher prevalence of antimicrobial resistance due to higher consumption of antibiotics could also be characterized by a higher rate of CDI [14, 15]. In Campania, a southern Italian region, antimicrobial resistance has become an extremely worrying phenomenon. According to the latest official report, the rising rate of MDR pathogen isolation seems caused not only by the absence of efficacious in-hospital infection control plans, but also to the common misuse of antibiotics in general practice and the frequent inappropriate management of antimicrobial therapy in outpatient settings [16].
Many of the factors behind the increasing rate of MDR microorganism, such as inappropriate antimicrobial choice/dosage and in general the lack of well-structured antimicrobial stewardship, play a key role in the promotion of CDI [17]. In the past few years, the epidemiological importance of this microorganism has markedly increased. In fact, the 2010-2011 ECDC point prevalence survey assumed an incidence of 123,997 cases of CDI per year (affecting especially the elderly). Moreover, CD is responsible for 48% of healthcare-associated gastrointestinal infections [18]. Unfortunately, there is a dramatic lack of data regarding the epidemiological impact of CDI in Campania and only some sparse data available in literature [19, 20]. The relationship between CDI incidence and MDR bacteria diffusion also remains unknown.
In this study, we aimed to assess current practice patterns in terms of CDI diagnosis and infection control through a multicenter, region-based survey carried out among local hospitals. Moreover, the study exploited CDI incidence data collected during the 6-month prospective surveillance programme.
METHODS
Study plan
In 2016, the Italian National Center for Disease Control (Centro Controllo delle Malattie, CCM) supported a project involving 3 Italian Regions: Friuli Venezia Giulia, Lazio and Campania, each representing a different geographical area (North, Centre, South Italy, respectively). Southern Italy was, therefore, represented by Campania and the Monaldi hospital was identified as the regional coordinating centre for this project. Accordingly, a network of 49 hospitals willing to participate in the project was created in 2017 (Figure 1). The project consisted of two phases: a survey on practice patterns concerning CDI and an epidemiological surveillance study.
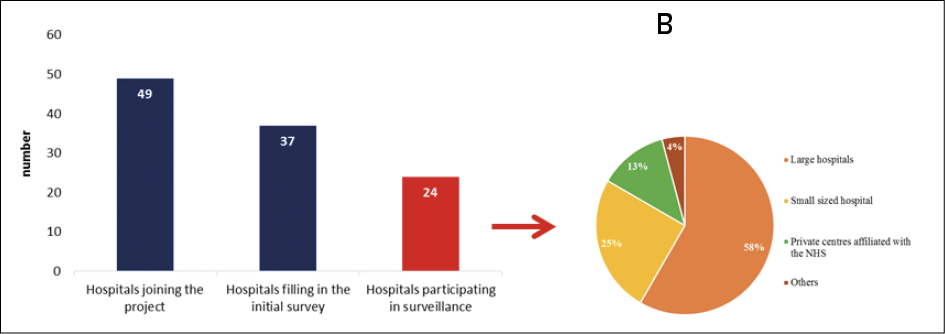
Figure 1 - Health-care facilities participating to the different phases of the CCM2016 CDI project, Campania. Right sided panel details size of hospitals participating in the active surveillance of CDI. NHS: National Health Service.
Survey phase
In the first phase, information was collected from 37 of the 49 (85.5%) facilities initially involved, by means of completing a questionnaire. This survey aimed at understanding current practice patterns on:
- the management of hospital-acquired and C. difficile infections;
- the management of patients with diarrhoea;
- the presence and the relevance of an Antimicrobial Stewardship programme at each facility;
- the implementation of best practice protocols for the correct use of antibiotics, as well as protocols for the microbiological diagnosis of CDI.
Active surveillance study
After this first observational and descriptive phase of the project, an active 6-month surveillance programme was carried out, aimed at obtaining contemporary data on the incidence of CDI in our region. Only hospitals where the diagnostic algorithm was compliant with current recommendations participated in this active surveillance. Therefore, from February 1st to July 31st 2018, 24 of the 49 centres took part to this second phase (25% large hospitals, 58% small-sized hospital, 13% private hospitals affiliated with the National Health Service) (Figure 1).
In brief, each centre had a standard single case report form and a summary form to complete, in order to evaluate admissions, total patient bed-days and total CDI cases in the six-month surveillance period. The coordinating centre collected data obtained and assessed the relation between total CDI cases and number of patient bed-days in the 24 regional facilities involved.
RESULTS
Regarding the management of hospital-acquired and C. difficile infections, we detected a diffuse lack of surveillance programmes for the control of CDI. In fact, only 15 (40%) of the participating facilities declared that a surveillance programme able to detect the impact of CDI was already in place. Most of these 15 hospitals (n=9, 60%) had an active surveillance plan, whereas 3 (20%) and 1 (6.6%) hospitals owned a surveillance programme based on detecting only the prevalence and incidence of CDI, respectively (Figure 2). No further details were given by the remaining 2 hospitals. Moreover, almost half of the participating hospitals (n=16, 43%) did not have standardized procedures and protocols to control and prevent CDI, such as hand hygiene, glove usage or standardized procedures to disinfect surfaces, etc. A structured protocol to isolate infected or colonized patients as well as measures to control C. difficile diffusion were in place in only 13 (35%) hospitals. These results clearly showed there was a stringent need to improve the awareness about CDI among the Regional health-care community. Despite of that, training events aimed at health-care personnel and focusing on the management of CDI infections had actually taken place in only 23% of the participating facilities in 2016-2017. Notwithstanding, a microbiology laboratory and a health-care related infection group existed in most facilities (89% for both).
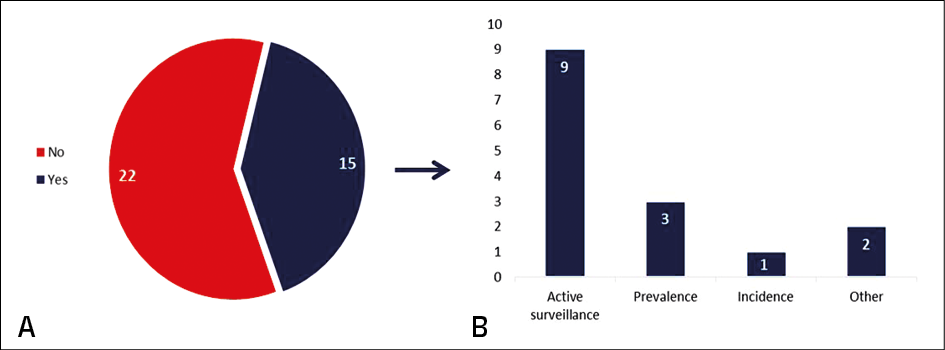
Figure 2 - Prevalence and characteristics of CDI surveillance programs in the health-care facilities participating to the CCM2016 CDI project, Campania.
Panel A: presence of a dedicated CDI surveillance program in the Hospital.
Panel B: type of CDI surveillance program in place.
Regarding the management of patients with diarrhoea without laboratory-confirmed CDI, 65% of the involved hospitals declared they were carrying out contact isolation. However, none performed contact isolation in single rooms with dedicated toilets, but mostly choose multiple rooms with dedicated toilets (27%) or single rooms without a dedicated toilet (27%). Likely, this is related to a lack of dedicated spaces where managing suspected patients, due to overcrowded health-care facilities and overloaded health-care personnel. Indeed, even after CDI confirmation, contact isolation was mostly obtained using multiple rooms with dedicated toilets (81%) or isolation occurred in CDI cohorts when single rooms were not available. Moreover, in 50% of the hospitals, isolation was discontinued when diarrhoea resolved and a repeated CDI test resulted negative. In particular, only 13% discontinued isolation 48 hours after the last liquid stool emission, as recommended by guidelines [10].
As far as Antimicrobial Stewardship is concerned, a formal, active operating group was effectively present in 59% of the hospitals, mostly made up of physicians, microbiologists and pharmacists. However, only 13 (35%) of them had drawn up a formal antimicrobial stewardship plan adapted to the hospital own features (Figure 3). By contrast, 64% of the hospitals declared to have adopted rules and recommendations on the correct use of antibiotics such as antibiotic therapy planning, antibiotic association and/or class restriction.
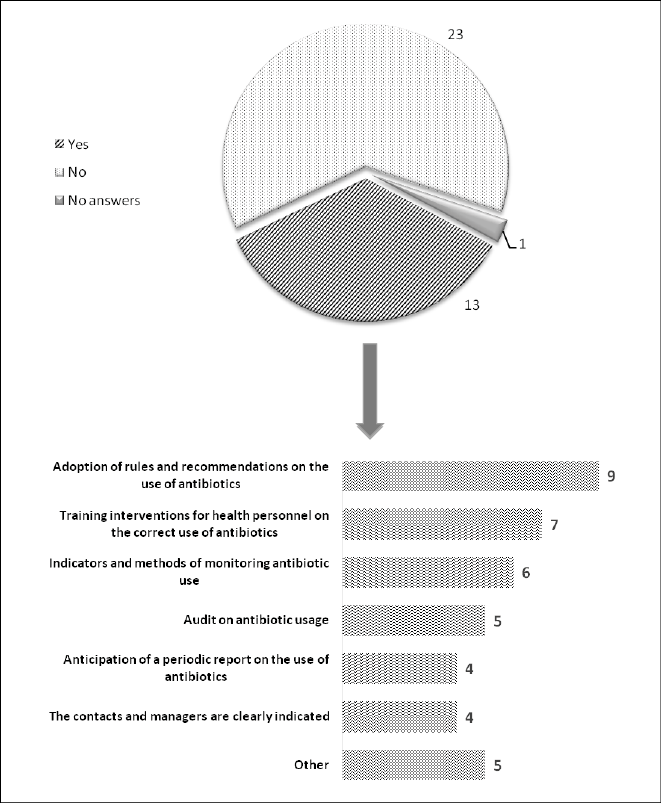
Figure 3 - Prevalence and characteristics of antimicrobial stewardship activity plans (ASAP) at the different clinical facilities participating in the study.
Panel A: Prevalence of a formal ASAP on site.
Panel B: Features of the ASAP in the facilities with an existing plan.
In terms of microbiology laboratory procedures, the stool samples tested for CDI are usually those classified as Bristol 5, 6 or 7 (81%) and this may be related to the tendency of analysing all samples with an associated clinician request. Interesting data emerged regarding tests available to diagnose CDI in different laboratories of our region. A GDH and Toxin A/B EIA was used in 27% of the hospitals, whereas only a single test, NAAT or GDH EIA or Toxin A/B EIA, was available in the other facilities. Therefore, the recommended two step algorithm could be effectively carried out only in a minority of our region laboratories, thus influencing the reliability of both negative and positive results (Figure 4). In fact, most of the microbiology laboratories performed CDI diagnosis only by means of NAAT.
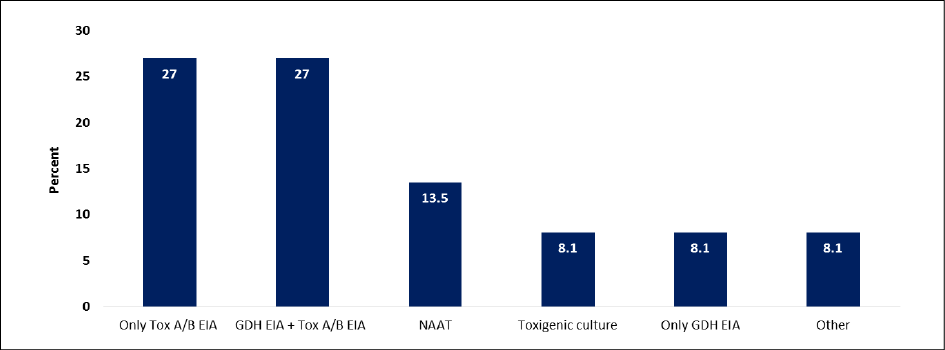
Figure 4 - Laboratory tests available to diagnose CDI in the participating centers.
We then analysed the results of the active surveillance study conducted in 24 of the hospitals participating in the project. Total CDI cases diagnosed were 87 and total patient bed-days were 903334, with a total number of admissions equal to 122988. The incidence of CDI infection according to these figures was 0.96 CDI cases/10000 patient bed-days, a figure much lower than expected based on prior studies conducted elsewhere [21]. A detail of the distribution of cases among the participating clinical centres is shown in Figure 5.
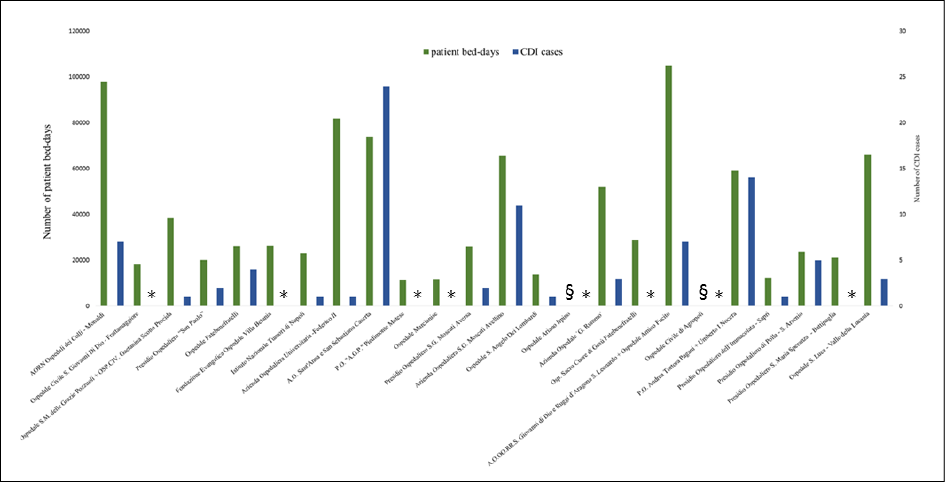
Figure 5 - Graphical representation of admission volumes and Clostridioides difficile infection (CDI) cases for each participating clinical center in the prospective surveillance programme.
* = no reported cases; § = no data available.
To spread awareness of good practice in terms of C. difficile infection and antimicrobial stewardship through the regional hospital network, several educational meetings, carried out after the surveillance period, were organized. These meetings, with colleagues involved in the project, were focused on different aspects of CDI diagnosis and management (diagnostic algorithms, current recommended treatment options and infection control measures to contain CDI diffusion). Moreover, because of the strict association between antimicrobial misuse and CDI, we prepared and spread among local hospitals a short and practical published guide on antibiotic prescription and administration.
DISCUSSION
Our study is among the few epidemiologic analyses of CDI performed in Europe and the first of its kind carried out in a southern Italian region. This setting is of particular interest, being characterised by low aging index, low median population age and high consumption of antibiotics, both in hospitals and the community. The latter factor is the likely determinant of the disproportionately high rates of antimicrobial resistance demonstrated among invasive bacterial isolates [16]. We therefore expected a parallel high incidence of CDI, a paradigm of antimicrobial resistance and a direct consequence of antibiotic use.
The results of our study suggest CDI remains a rather neglected clinical issue in our Region. Surveillance programmes and standardized procedures and protocols aimed at CDI control and prevention were largely lacking. Also, the recommended microbiology diagnostic protocol could be performed only in a minority of our Region laboratories, suggesting inadequate diagnostic capabilities. These two factors were possibly influencing the results of our active surveillance study, showing a lower than expected incidence of CDI (0.96 CDI cases/10000 patient bed-days vs 3.19 in a large European study) [21].
These results clearly show a stringent need to improve the awareness about CDI among the Regional health-care community. Also, our epidemiologic analysis indicates the need to improve hospital-based management strategies for patients with CDI or, in general, nosocomial diarrhoea, in order to fill the gap between international guidelines and our daily clinical practice. Although to a lesser extent, this need is also obvious for the overall antimicrobial stewardship, not only to prevent antibiotic-associated diarrhoea and/or CDI but also reduce the increasing rate of drug resistant microorganisms. We started to give a contribution to improve knowledge and practices regarding CDI in our Region by organizing educational workshops with involved physicians and laboratory personnel.
Spreading the awareness that antimicrobial stewardship is of utmost importance plays, we believe, a key role. Indeed, the absence of an “antimicrobial stewardship activity plan” in a consistent fraction of the participating hospitals demonstrates a sparse interest in this field. This could simply be improved by encouraging dialogue and interdisciplinary exchange among healthcare professionals and by organizing further focused meetings.
In our opinion, it is of paramount importance to concentrate on dedicated training programmes for hospital personnel focusing on the correct use of antimicrobials in order to improve the quality of prescribed antimicrobial courses and reduce the impact of those therapies on our patients’ microbiota.
The low CDI incidence found in our “high antimicrobial resistance” Region deserves further comment. Several reasons could actually explain these figures. As said above, underdiagnosis, both related to the absence of an updated diagnostic algorithm, wrong patient selection and/or absence of adequate diagnostic assays, cannot be ruled out. However, a real lower prevalence of CDI in Campania could be related to the actual diet, the lower patient age (being advanced age a major risk factor for CDI) or the specific genetic background. Unquestionably, further studies are warranted to either confirm or rebut these hypotheses.
Conflict of interest
None of the authors has any conflict of interest to disclose relevant to the contents of this article.
Funding
This study was supported by the Italian Ministry of Health through the Centro Controllo delle Malattie, bando 2016, grant n. F52F17000000001.
REFERENCES
[1] Furuya-Kanamori L, Marquess J, Yakob L, et al. Asymptomatic Clostridium difficile colonization: epidemiology and clinical implications. BMC Infect Dis. 2015; 15, 516.
[2] Mylonakis E, Ryan ET, Calderwood SB. Clostridium difficile–Associated Diarrhea: A Review. Arch Intern Med. 2001; 161 (4), 525-33.
[3] Gupta A, Khanna S. Community-acquired Clostridium difficile infection: an increasing public health threat. Infect Drug Resist. 2014; 7, 63-72.
[4] Di Bella S., Capone A., Musso M. et al. Clostridium difficile infection in the elderly. Infez Med. 2013; 21 (2), 93-102.
[5] Bauer MP, Goorhuis A, Koster T, et al. Community-onset Clostridium difficile-associated diarrhoea not associated with antibiotic usage-two case reports with review of the changing epidemiology of Clostridium difficile-associated diarrhoea. Neth J Med. 2008; 66 (5), 207-11.
[6] Sedigh ESH, Hamid H, Ali A, et al. A multicenter-based study on epidemiology, antibiotic susceptibility and risk factors of toxigenic Clostridium difficile in hospitalized patients in southwestern Iran. Infez Med. 2018; 26 (4), 308-15.
[7] Rao K, Malani PN. Diagnosis and treatment of Clostridioides (Clostridium) difficile infection in adults in 2020. JAMA. 2020; 323 (14), 1403-4.
[8] Henrich TJ, Krakower D, Bitton A, Yokoe DS. Clinical risk factors for severe Clostridium difficile-associated disease. Emerg Infect Dis. 2009; 15 (3), 415-22.
[9] Eze P, Balsells E, Kyaw MH, Nair H. Risk factors for Clostridium difficile infections - an overview of the evidence base and challenges in data synthesis. J Glob Health. 2017; 7 (1), 010417.
[10] Crobach MJ, Planche T, Eckert C, et al. European Society of Clinical Microbiology and Infectious Diseases: update of the diagnostic guidance document for Clostridium difficile infection. Clin Microbiol Infect. 2016; 22 (Suppl. 4), S63-81.
[11] Gerding DN, Muto CA, Owens RC Jr. Measures to control and prevent Clostridium difficile infection. Clin Infect Dis. 2008; 46 (Suppl. 1), S43-9.
[12] Balsells E, Filipescu T, Kyaw MH, Wiuff C, Campbell H, Nair H. Infection prevention and control of Clostridium difficile: a global review of guidelines, strategies, and recommendations. J Glob Health. 2016; 6 (2), 020410.
[13] McDonald LC, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018; 66 (7), e1-e48.
[14] Pereira JB, Farragher TM, Tully MP, Jonathan Cooke J. Association between Clostridium difficile infection and antimicrobial usage in a large group of English hospitals. Br J Clin Pharmacol. 2014; 77 (5), 896-903.
[15] Deshpande A, Pasupuleti V, Thota P, et al. Community-associated Clostridium difficile infection and antibiotics: a meta-analysis. J Antimicrob Chemother. 2013; 68 (9), 1951-61.
[16] Sarnelli B, D’Agostino F, Signoriello G, Guida A. Rapporto 2017 sull’antibiotico resistenza e sull’uso di antibiotici rilevati nelle strutture ospedaliere della Campania; http://www.regione.campania.it/regione/it/tematiche/antibiotico-resistenza-ed-infezioni-correlate-all-assistenza-64 [Accessed 20 November 2020]
[17] Llor C., Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014; 5 (6), 229-41.
[18] European Centre for Disease Prevention and Control. Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals. Stockholm: ECDC. 2013.
[19] Mancini A, La Vigna G, Puciarelli S, Lombardi FE, Barocci S. A three-year study entailing molecular characterization and epidemiology of Clostridium difficile in an Italian tertiary care hospital. Infez Med. 2018; 26 (3), 204-9.
[20] Riccobono E, Di Pilato V, Della Malva N, et al. Draft genome sequence of Clostridium difficile belonging to ribotype 018 and sequence type 17. Genome Announc. 2016; 4 (5), e00907-16.
[21] European Centre for Disease Prevention and Control. Healthcare-associated infections: Clostridium difficile infections. In: ECDC. Annual epidemiological report for 2016. Stockholm: ECDC; 2018.