Le Infezioni in Medicina, n. 1, 65-69, 2021
ORIGINAL ARTICLES
Clinical profile and treatment outcomes of patients with brucellosis: a hospital-based cohort study from Southern India
Sindhu Pericherla1, Nitin Gupta2,3, Kavitha Saravu2,3
1Department of Medicine, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India;
2Department of Infectious diseases, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India;
3Manipal McGill Center for Infectious Diseases, Manipal Academy of Higher Education, Manipal, Karnataka, India
Corresponding author
Kavitha Saravu
E-mail: kavithasaravu@gmail.com
SummaRY
The clinical epidemiology of patients with brucellosis in India has not been well described. The aim of this study was therefore to delineate the demographic and clinical characteristics, complications and treatment outcomes of patients diagnosed with brucellosis. A prospective cohort study was conducted from January 2015 to June 2017. All patients above the age of 18 years with a confirmed diagnosis of brucellosis were enrolled and followed up for six months to study the outcomes of treatment. Of the 94 patients enrolled, 77% were male. A total of 38% of the patients had a history of animal contact, and 24% had a history of consumption of unpasteurized dairy products. Acute brucellosis was found in 65% of the patients, and sub-acute presentation was seen in the rest. Fever (94%) and arthralgia (54%) were the most predominant symptoms. The most common focal complication was osteoarticular involvement (34%). Except for three patients, all those who were available for follow-up showed a complete response to therapy. In conclusion, brucellosis should be suspected in patients with fever and osteoarticular involvement in endemic areas. Early identification and prompt initiation of treatment are associated with high cure rates.
Keywords: Brucella spp., spondylodiscitis, neurobrucellosis.
INTRODUCTION
Brucellosis is a zoonotic disease caused by a Gram-negative bacteria belonging to the genus Brucella [1]. With sustained efforts like effective livestock vaccination, strict hygienic practices during handling of animals or their products, and pasteurization, the disease has been controlled in developed countries. Although brucellosis is thought to be endemic in developing countries like India, epidemiological reports from India are scarce [2]. Diagnostic challenges and the large etiologic spectrum of febrile illnesses may have contributed to substantial under-diagnosis of Brucella infections in developing countries. This study, therefore, aimed to describe the clinical profile and outcomes of patients diagnosed with brucellosis.
PATIENTS AND METHODS
A prospective cohort study was conducted in Kasturba Hospital (KH), Manipal, Karnataka, India during a two and a half year period (from January 2015 to June 2017). Kasturba Medical College and Hospital, Manipal is a teaching hospital that has more than two thousand beds and several intensive care units and caters to a large catchment area in South India. Ethical clearance for the study was obtained from the Institutional Ethics Committee (IEC No-543/2015) before the commencement of this study. Written informed consent was obtained from all participants prior to enrolment. All the individuals above the age of 18 years who presented with clinical features suggestive of brucellosis were screened by the investigators for possible inclusion in the study. Their blood culture (BACTEC Plus Aerobic/F and/or PEDS PLUS/F culture bottles; Becton Dickinson, Franklin Lakes, NJ, USA) and standard agglutination test was sent in consultation with the treating unit. A positive SAT was defined as a single titre of ≥1:160. Any patient with a positive Standard Agglutination Test (SAT) or blood culture growing Brucella spp. was enrolled in the study. Information regarding demographic profile, risk factors of brucellosis, clinical characteristics, laboratory investigations and treatment regimen were captured in a structured case report form (CRF). The treatment in each patient was determined by the treating physicians. Patients were followed up for a period of 6 months for outcome assessment. At six-month follow-up, patients were categorized as “cure” if they had complete resolution of symptoms and were classified as “relapse” if they had reappearance of the symptoms after initial improvement.
Data was entered in the CRF using Microsoft Excel 2013 and independently reviewed by a second person for any errors. Frequencies and proportions were used to summarize categorical variables. Mean±SD was used to summarize continuous variables, and median with interquartile range was used to summarize the skewed variables. Data analysis was performed using Statistical Package for the Social Sciences (SPSS) version 22.0.
RESULTS
A total of 94 subjects with brucellosis were included in the study. Of the 94 patients, 77 patients were male. The mean age was 43.6 years (range 18 to 75), with the highest number of cases observed between the ages of 30-49 years. A total of 40/94 (42.6%) patients were agriculturists. In terms of comorbidities, 24/94 (25.5%) had diabetes, 23/94 (24.4%) had hypertension and 2/94 (2.2%) had chronic renal disease. Though cases were distributed throughout the year, the greatest number of cases were seen in May (10/94, 13.5%). A total of 23/94 (24.5%) patients had a history of consumption of unpasteurized dairy products, and 36/94 (38.2%) had a history of animal contact with cow (n=16, 44.4%), buffalo (n=15, 41.6%), sheep (n=4, 11.3%) and goat (n=1, 2.7%).
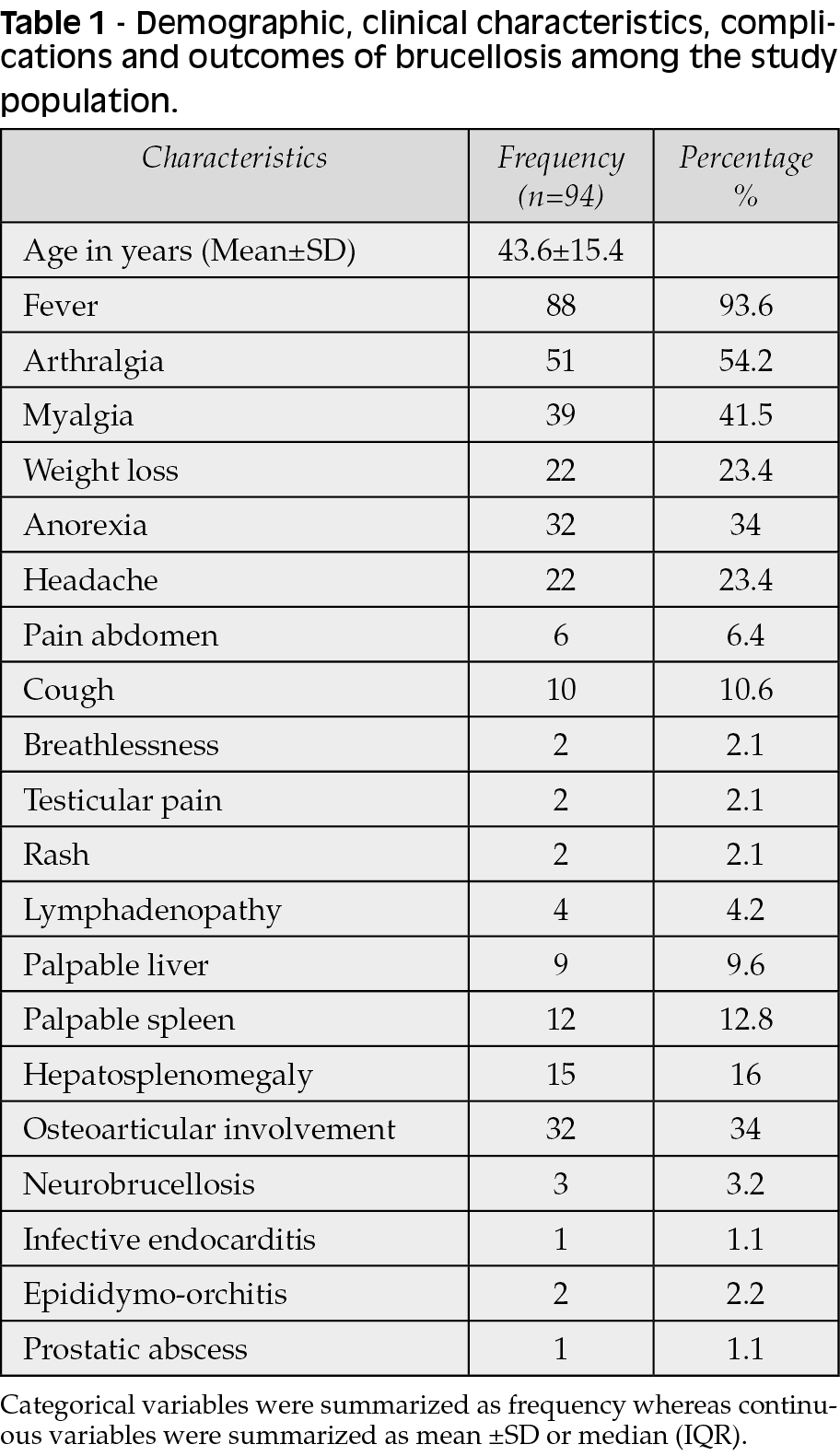
Fever was the most predominant symptom and was seen in 88 (93.6%) patients. This was followed by arthralgia, which was seen in 51 (54.2%) patients. The median duration of fever was 20 (IQR: 14-45) days. The details of other clinical features have been summarized in Table 1. Osteoarticular involvement was the most common focal complication, which was seen in 32 (34%) patients. Of these 32 patients, isolated peripheral joint involvement was seen in three patients while the remaining 29 patients had spine involvement in the form of spondylitis/ spondylodiscitis (n=26), isolated sacroiliitis (n=2) and epidural abscess with no vertebral abnormality (n=1). Magnetic resonance imaging was done in all patients presenting with back pain. Disk abnormalities were noted in 19 patients, marginal anterior osteophytes in 15 patients, and sclerosis of the vertebral body in 5 patients. Cerebrospinal fluid analysis in three patients with neurobrucellosis showed pleocytosis with total cells exceeding 100 cells, lymphocytic predominance and elevated protein.
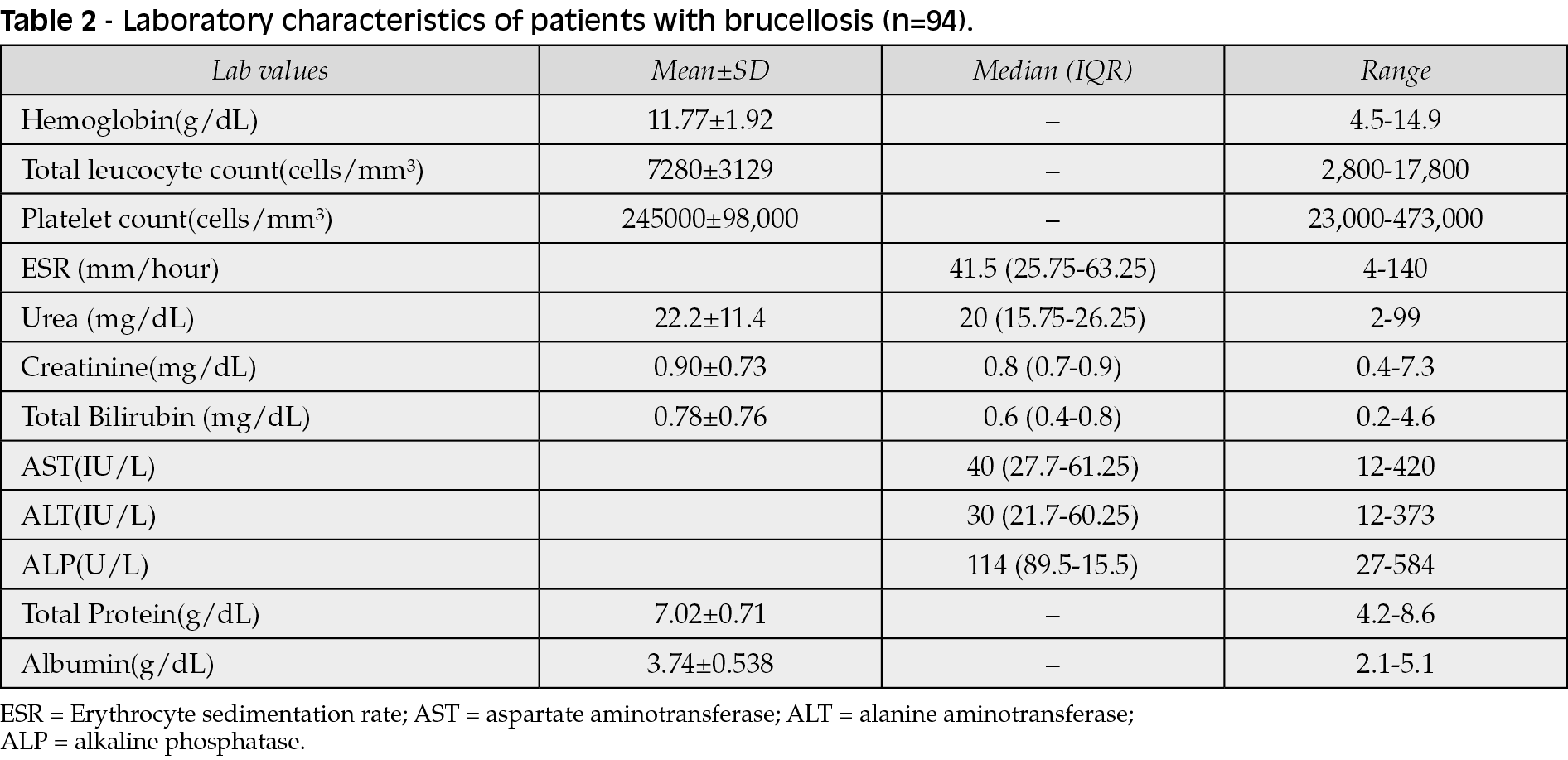
The haematological and biochemical abnormalities have been summarized in Table 2. SAT positivity was seen in 84 (89%) of which 1:160 titre in 41 (43.6%), 1:320 in 15 (16%), 1:640 in 22 (23.4%) and 1:1280 in 6 (6.3%) patients. Brucella was isolated from blood in 51 (54.2%), bone marrow in 8 (8.4%) and from a suppurative collection in one (1.06%) patient.
Of the 94 patients, 21 (22.3%) received empirical antibiotic treatment, of which four we prescribed drugs for presumed tuberculosis. MRI spine was initially mistaken for Mycobacterium tuberculosis-associated spondylodiscitis in 6 (6.3%) patients. Similarly, bone marrow biopsy was mistakenly diagnosed as tuberculosis due to the presence of granulomas in 2 (2.2%) patients. Brucella-specific regimens included monotherapy with doxycycline in 3 (3%), doxycycline-rifampicin in 10 (10.6%), doxycycline-streptomycin in 24 (25.5%), doxycycline-gentamicin in 38 (40.4%), doxycycline-streptomycin-rifampicin in 7 (7.4%) and doxycycline-gentamicin-rifampicin in 12 (12.7%) patients. The mean duration of parenteral antibiotic (aminoglycoside) was 1.98±0.5 weeks, while it was 8±3.3 weeks for oral antibiotic (doxycycline, rifampicin). The mean duration of hospitalization was 10±5 days. Thirty (31.9%) patients were lost to follow up within six months of discharge. Sixty-one of 94 (64%) patients were cured [61/64 analyzable patients (95.3% [95%CI 86.9-99.0]) during the six-month follow up while three of the patients were diagnosed to have relapse [3/64 analyzable patients (4.8% [95%CI 0.9-13.0]). There was no in-hospital mortality in the present study.
DISCUSSION
Karnataka state, comprising of 30 districts, is the seventh-largest Indian state by area and eighth-largest state by population. Most people in the state reside in the rural area, and agriculture is their main occupation. Our cohort of 94 patients with brucellosis from Kasturba hospital show Brucella spp. infection to be a contributor to prolonged fever syndromes in Southern India. In our study, male preponderance (77.6%) was seen similar to other studies from India, which may be related to increased occupational exposure to the livestock [3, 4]. The disease was widely distributed among all age groups but was more prevalent in middle-aged and young adults. Thirty-six (38.2%) had a history of animal contact, and twenty-three (24.5%) gave a history of consuming unpasteurized dairy products which are known to be risk factors associated with the disease. The results are comparable with a study done by Jia et al. which included 590 patients, of which 145 (24.6%) patients had a history of consumption of unpasteurized dairy products, raw meat [5]. Some authors have emphasized that direct contact with infected animals and their products is more important than ingestion of contaminated animal products for brucellosis transmission [6]. Incident cases in our cohort were distributed throughout the year, in contrast to studies from temperate countries where the incidence of brucellosis is strongly seasonal and in line with exposure to farm animal parturition patterns in these regions [7].
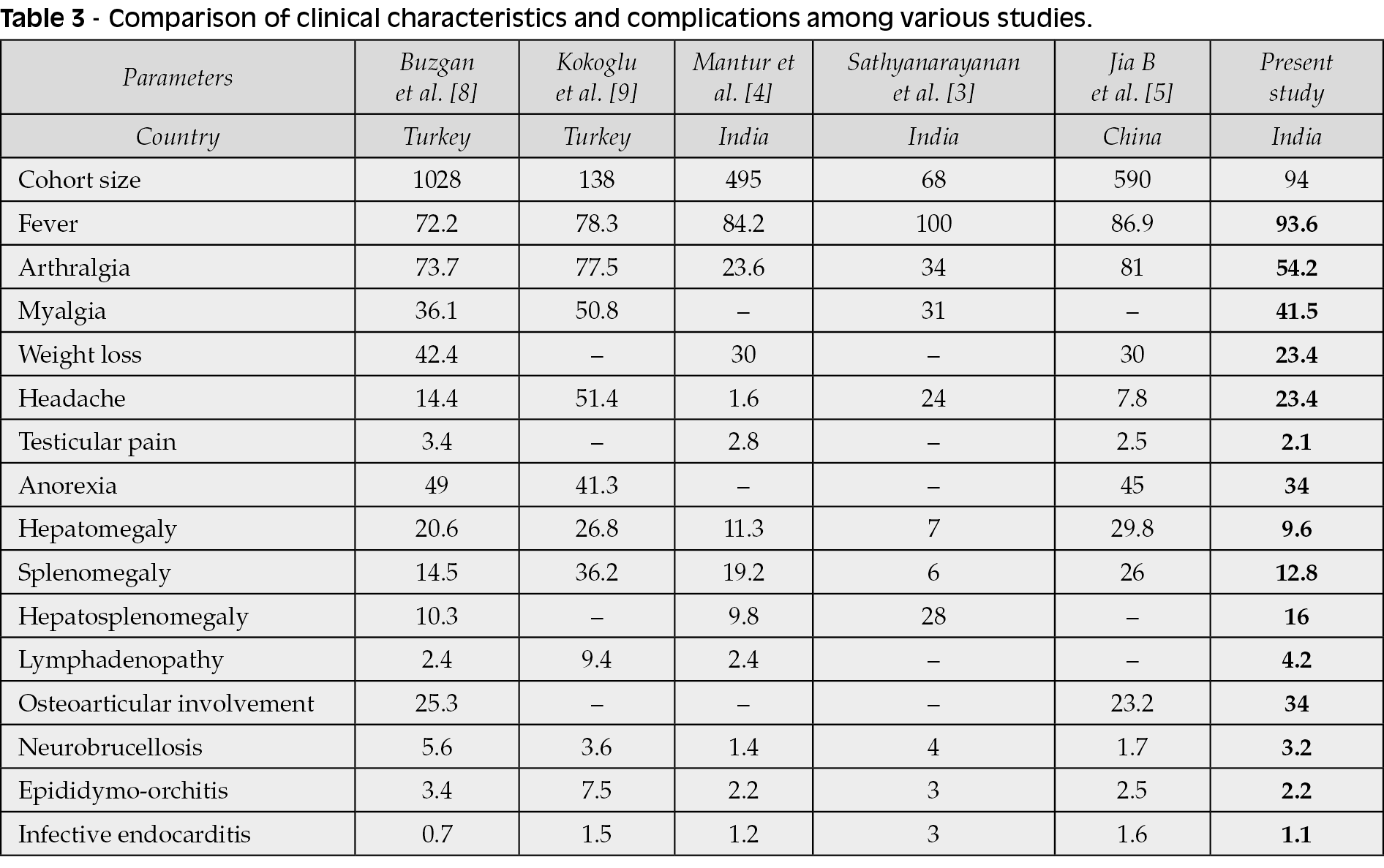
Although prolonged fever was by far the most common presenting symptom, seen in 93.6% of patients, we observed a broad array of clinical manifestations, in agreement with previous reports [5, 8, 9]. The spinal involvement in brucellosis can resemble spondylitis from M. tuberculosis and often leads to empiric antituberculosis prescriptions. In the present study, antituberculous therapy was started in four patients based on radiologic features that were later attributed to brucellosis. Although some radiological findings like epiphysitis of the antero-superior endplate (Pedro-Pons sign) have been suggested to be more common with brucellosis when compared to tuberculosis, they are not specific enough to rule out tuberculosis [10]. Brucellosis and tuberculosis may also present similar histopathological features by inducing the formation granulomas. Hence, in endemic countries where both brucellosis and tuberculosis coexist, confirmatory testing is essential.
Brucella was diagnosed either by standard agglutination test or by culturing blood/bone marrow on BACTEC. The automated culture technique has replaced the conventional method of isolation of Brucella, which helps in early diagnosis [11, 12]. Since blood culture suffers from poor sensitivity; serological tests are often required to make a diagnosis. Ideally, a four-fold increase in titre is required to make a diagnosis on serology, but a single SAT titre of ≥1: 160 has been suggested to be significant [8]. Reliance on SAT for diagnosis of brucellosis is not without problems. Sensitivity in the first two weeks of disease is relatively low [13]. In addition, false-negative results from a “prozone” phenomenon may also be observed with serum agglutination testing (i.e. falsely negative or borderline results from an immunological test due to very high antibody levels) [14]. Conversely, interpretation of SAT results can be complicated by lack of specificity from cross-reactivity with numerous other bacteria [13]. Finally, the usefulness of existing serological tests for the diagnosis of relapsed infections is very limited since host antibodies remain present for many years.
The most common regimen used in our study was the combination of doxycycline with an aminoglycoside in 62 (65.9%) patients. This was in line with the extensive meta-analysis of randomized control trials done by Skalsky et al., which included 30 trials with 77 treatment arms, showed doxycycline-streptomycin was more effective than doxycycline-rifampicin. [15]. The outcome assessment was limited due to a significantly higher proportion of lost to follow up cases. Although the reason for loss to follow up could have been the development of complications or mortality, no in-hospital mortality was demonstrated in our series. In those where follow up could be done, the cure rate was very high.
This study has the limitation thatthe speciation of Brucella spp. was not done.
In conclusion, brucellosis typically presents as a protracted illness in patients from endemic areas. It may be overlooked and misdiagnosed, due to its protean presentations and overlap with tuberculosis in terms of clinical, radiological and histological features. Early, accurate diagnosis and prompt initiation of treatment are associated with a favourable response.
Conflict of interest
The authors declare no conflict of interest.
Funding
None
Acknowledgements
Authors acknowledge the Department of Microbiology, KMC Manipal for identification of isolates.
REFERENCES
[1] Hayoun MA, Muco E, Shorman M. Brucellosis. StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
[2] Dean AS, Crump L, Greter H, Schelling E, Zinsstag J. Global burden of human brucellosis: a systematic review of disease frequency. PLoS Negl Trop Dis. 2012; 6 (10), e1865.
[3] Sathyanarayanan V, Razak A, Saravu K, Ananthakrishna SB, Prabhu MM, Vandana KE. Clinical profile of brucellosis from a tertiary care center in southern India. Asian Pac J Trop Med. 2011; 4 (5), 397-400.
[4] Mantur BG, Biradar MS, Bidri RC, et al. Protean clinical manifestations and diagnostic challenges of human brucellosis in adults: 16 years’ experience in an endemic area. J Med Microbiol. 2006; 55 (Pt 7), 897-903.
[5] Jia B, Zhang F, Lu Y, et al. The clinical features of 590 patients with brucellosis in Xinjiang, China with the emphasis on the treatment of complications. PLoS Negl Trop Dis. 2017; 11 (5), e0005577.
[6] Abo-Shehada MN, Odeh JS, Abu-Essud M, Abuharfeil N. Seroprevalence of brucellosis among high risk people in northern Jordan. Int J Epidemiol. 1996; 25 (2), 450-4.
[7] Dajani YF, Masoud AA, Barakat HF. Epidemiology and diagnosis of human brucellosis in Jordan. J Trop Med Hyg. 1989; 92 (3), 209-14.
[8] Buzgan T, Karahocagil MK, Irmak H, et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010; 14 (6), e469-78.
[9] Kokoglu OF, Hosoglu S, Geyik MF, et al. Clinical and laboratory features of brucellosis in two university hospitals in Southeast Turkey. Trop Doct. 2006; 36 (1), 49-51.
[10] Pourbagher A, Pourbagher MA, Savas L, et al. Epidemiologic, clinical, and imaging findings in brucellosis patients with osteoarticular involvement. Am J Roentgenol. 2006; 187 (4), 873-80.
[11] Cockerill FR, Wilson JW, Vetter EA, et al. Optimal testing parameters for blood cultures. Clin Infect Dis. 2004; 38 (12), 1724-30.
[12] Mantur BG, Mangalgi SS. Evaluation of conventional castaneda and lysis centrifugation blood culture techniques for diagnosis of human brucellosis. J Clin Microbiol. 2004; 42 (9), 4327-8.
[13] Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Brucellosis. N Engl J Med. 2005; 352 (22), 2325-36.
[14] Díaz R, Casanova A, Ariza J, Moriyón I. The Rose Bengal Test in human brucellosis: a neglected test for the diagnosis of a neglected disease. PLoS Negl Trop Dis. 2011; 5 (4), e950.
[15] Skalsky K, Yahav D, Bishara J, Pitlik S, Leibovici L, Paul M. Treatment of human brucellosis: systematic review and meta-analysis of randomized controlled trials. BMJ 2008; 336 (7646), 701-4.