Le Infezioni in Medicina, n. 1, 54-64, 2021
ORIGINAL ARTICLES
Psychological distress during the initial stage of the COVID-19 pandemic in an Italian population living with HIV: an online survey
Valentina Delle Donne1, Nicoletta Ciccarelli2, Valentina Massaroni1, Francesca Lombardi3, Silvia Lamonica3, Alberto Borghetti3, Massimiliano Fabbiani4, Roberto Cauda1,3, Simona Di Giambenedetto1,4
1Infectious Diseases Institute, Department of Safety and Bioethics, Catholic University of Sacred Heart, Rome, Italy;
2Department of Psychology, Catholic University, Milan, Italy;
3UOC Infectious Diseases, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy;
4Infectious and Tropical Diseases Unit, Department of Medical Sciences, University Hospital of Siena, Siena, Italy
Corresponding author
Valentina Delle Donne
E-mail: valentina.delledonne@unicatt.it
SummaRY
The aim of this study was to explore the psychological impact of the initial stage of the 2019 coronavirus (COVID-19) pandemic on people living with HIV (PLWH), a population at increased risk of psychological distress. PLWH participated in an online survey exploring demographic and clinical data, physical symptoms, contact history, knowledge and concerns, precautionary measures and additional information about COVID-19 during the first phase of the pandemic in Italy. The Impact of Event Scale-Revised (IES-R) (identifying the COVID-19 pandemic as a specific traumatic life event) and the Depression, Anxiety and Stress Scale (DASS-21) also formed part of the survey. Out of 98 participants, 45% revealed from mild to severe psychological impact from COVID-19 according to IES-R. A lower percentage, instead, complained of significant levels of depression (14%), anxiety (11%) or stress (6%) according to DASS-21. Higher education, being unemployed, number of perceived COVID-19 physical symptoms, concerns about risk of contracting COVID-19 and the pandemic situation in Italy, and needing additional information to prevent COVID-19 infection were positively associated to a higher risk of negative psychological impact. Moreover, among the participants, female gender, age, fewer years from HIV diagnosis and not being aware of their own viremia were associated to a higher risk of negative psychological outcomes. Almost half of our PLWH sample experienced significant levels of distress related to the COVID-19 pandemic. Women, elderly patients and those with recent HIV diagnosis appear to be the more psychologically fragile subgroups. Our findings could help identify patients most in need of psychological interventions to improve the wellbeing of PLWH.
Keywords: COVID-19, pandemic, HIV, psychological impact, distress, mental health.
INTRODUCTION
The 2019 Coronavirus Disease (COVID-19), originated from Wuhan (China) at the end of 2019, has rapidly spread over the world becoming soon a pandemic. COVID-19 outbreak was declared a public health international emergency on January 30, 2020, by the World Health Organization (WHO) and now is affecting more than 200 countries and territories around the world.
Italy has been the first-hit European country to face the outbreak of COVID-19 and one of the most affected areas. On March 9th 2020, the Italian Government settled several emergency containment measures that began to be loosened only from May 4th onwards, to deal with the spread of the pandemic.
Evidence accumulated during the initial phase of the COVID-19 outbreak confirms that the pandemic is having a great psychological impact on individuals especially in worst-hit countries [1-3]. Mental health outcomes seem to be related to many factors: widespread contagion, containment and prevention measures such as self-isolation, social distancing, lockdown, and socio-economic impact [4-7].
Given the unprecedented nature of the COVID-19 outbreak, an increase in anxiety has been prevalent worldwide [8].
A review about the mental health outcomes of COVID-19 pandemic identified a wide list of negative psychological responses in Chinese general population: anxiety, depression, stress, insomnia, indignation, worries about their own and family health, sensitivity to social risks, life dissatisfaction, phobias, avoidance, social functioning impairment, compulsive behaviour and physical symptoms [3, 9-13]. Consistent predictors of psychological outcome were identified: female gender, aging, specific physical symptoms, poor self-rated health status, specific health information and certain precautionary measures, having relatives or acquaintances infected with COVID-19, and medical history of chronic illness [11, 13-15].
In Italy, a relevant percentage of the general population (38%) have experienced from mild to-severe psychological distress symptoms during the early phase of the COVID-19 outbreak, and evidence suggests a higher proportion compared to other European countries [16-19]. Furthermore, high rates of negative mental health outcomes, including post-traumatic stress symptoms and anxiety, were found [20].
Among predictors of psychological distress, a history of medical issues seems to be fundamental to identify groups at greater risk of distress and needing tailored psychological interventions [3].
Indeed, the Centers for Disease Control and Prevention highlighted that individuals with chronic health conditions, such as People Living With HIV (PLWH), may develop a stronger stress response than the rest of the population [21].
Although there is no clear evidence that the risk of COVID-19 infection is higher among PLWH compared to the general population, to cope with COVID-19 outbreak might have significant effects on the biological, psychological and social aspects of their lives [8].
Firstly, outpatients’ visits and treatment have been interrupted or postponed as a consequence of lockdown, and the fear of contracting COVID-19 has led to decreased engagement with care among PLWH in several countries [8, 22-26]. An incorrect management of HIV disease could lead to an increased risk of contracting COVID-19 and experiencing complications related to it, in addition to complications related to HIV disease progression [8].
Furthermore, the current pandemic is a significant stressor and could increase the risk of mental health concerns among PLWH [27].
Depression is the most common mental health disorder among PLWH, being two to four times more frequent than in HIV-negative people [28-31]. Depressive symptoms may be exacerbated by loneliness due to the physical distancing necessary to contain COVID-19, and may have adverse effects on treatment adherence [32-34].
Then, COVID-19 is assumed to function in a syndemic framework “that is two or more epidemics interacting synergistically to produce an increased burden of disease in a population” with several health challenges faced by PLWH including HIV itself, chronic non-communicable diseases, mental health burden, substance abuse, and other infections [35-37].
Therefore, due to the syndemic framework, the exposition to mental health issues and to a chronic illness, PLWH seem to be a group at greater risk of suffering from psychological distress during COVID-19 pandemic [8, 38-41].
Currently, there are only few data about mental health of PLWH during COVID-19 pandemic reporting elevated levels of anxiety, and showing that COVID-19 and associated restrictive measures seem detrimental to the well-being and follow-up of PLWH [42, 43]. The aim of this study was to better explore the psychological impact of the COVID-19 outbreak on an Italian cohort of PLWH and to assess the possible risk and protective factors, in order to help to tailor specific psychological interventions.
MATERIALS AND METHODS
Participants
This is a cross-sectional survey enrolling PLWH, followed at Infectious Diseases Institute of “Policlinico Gemelli Foundation” of Rome, between March 9th and May 25th 2020. This timeframe was chosen to assess participants’ responses at the end of the first phase of COVID-19 outbreak, following the Italian Government Decree-Law of May 4th 2020 that began to loosen emergency containment measures. All subjects were volunteers. They did not receive any financial remuneration for participating.
Exclusion criteria were age <18 years and difficulties with the Italian language.
Procedure
Each participant completed a 105-item online survey adapted from Wang C et al. (2020), in which data on demographic, clinical and COVID-related variables were collected “since the Decree-law of March 9th 2020 to today” (see below) [11]. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study
Demographic and HIV-associated clinical variables
Data were collected on gender, age range, education, employment status, sexual orientation, time from HIV diagnosis, time from first combined Antiretroviral Treatment (cART), HIV-1 plasma viral load and adherence to cART in the last month [using a Likert scale from 1 (very bad) to 10 (excellently)].
Physical health status variables
We gathered information regarding Health Service utilization, including consultation with a doctor, admission to the hospital, being tested for COVID-19 infection and being quarantined by a health authority. Moreover, physical symptoms variables included fever, chills, headache, myalgia, cough, breathing difficulty, dizziness, coryza, sore throat, and the triad of fever, cough and difficult breathing. Moreover, it was collected a self-report judgment about own health-state choosing one of the following answer options: poor, passable, good, very good or excellent.
Contact history variables
We asked if the respondents had contacts with individuals with suspected or confirmed COVID-19 infection or with infected materials (surfaces, objects, utensils).
Knowledge and concerns about COVID-19 variables
Regarding knowledge of COVID-19, we collected data about respondents’ habit of keeping informed about pandemic trend (number of infections, hospitalizations and deaths), the main source of health information, the level of satisfaction on health information [using a Likert scale from 1 (not satisfied) to 10 (extremely satisfied)], the knowledge about routes of transmission and likelihood of surviving if infected with COVID-19, choosing one of the following answer options: no chance, unlikely, likely, very likely and highly likely. The COVID-19 pandemic concerns were investigated as follows: level of confidence in the own doctor’s ability to diagnose COVID-19 [using a Likert scale from 1 (no trust) to 10 (full confidence)], concern of COVID-19 situation in Italy, to contract COVID-19 and about other family members getting COVID-19 infection [using a Likert scale from 1 (no concern) to 10 (extremely concern)], and feeling excessively worried about the epidemic, choosing one of the following answer options: always, most of times, sometimes, occasionally and never.
Precautionary measures variables
We investigated precautionary measures against COVID-19 put in place among: washing hands with soap and water, washing hands immediately after coughing, rubbing nose or sneezing, washing hands after touching contaminated objects, avoiding sharing of utensils during meals, covering mouth when coughing and sneezing, wearing mask regardless of the presence or absence of symptoms (choosing one of the following answer options: always, most of times, sometimes, occasionally and never), and average number of hours staying at home per day to avoid COVID-19 infection.
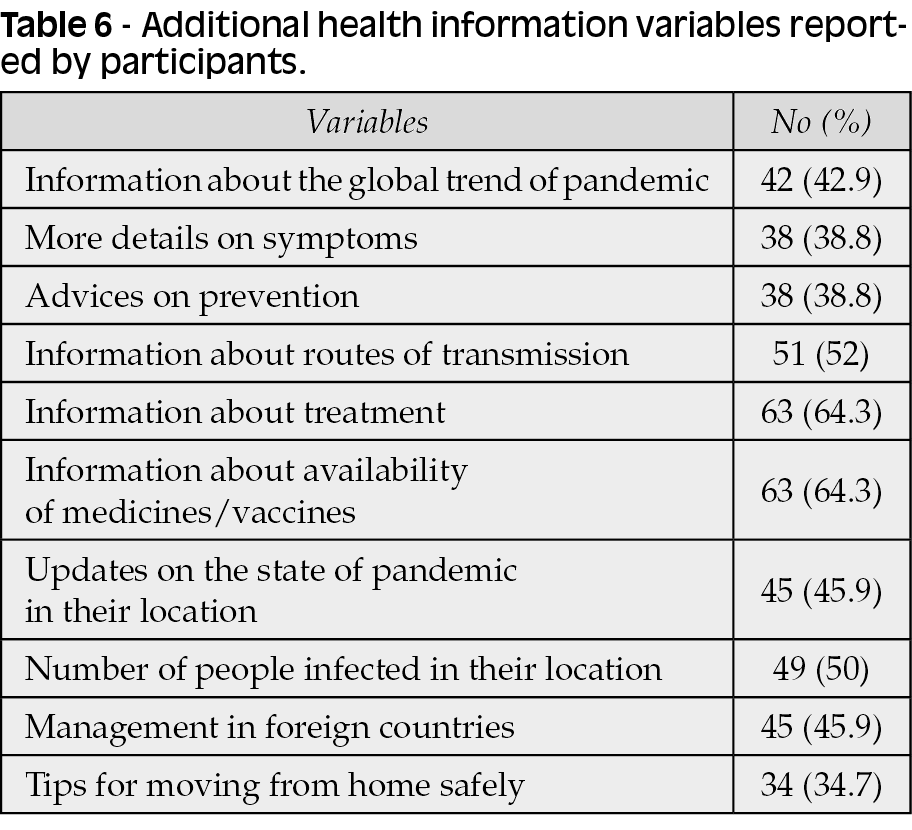
Additional health information variables
Further data were collected about the global trend of pandemic, more details on symptoms, additional advices on prevention, routes of transmission, treatment and the availability of medicines/vaccines, further regular updates on the state of pandemic and the number of people infected in their location and on the management of the outbreak in foreign countries, and more tips for moving from home safely during the outbreak.
Psychological impact of the COVID-19 outbreak and mental health status measures
To measure Psychological Impact of the COVID-19 outbreak, the Impact of Event Scale-Revised (IES-R) was administered [44]. The IES-R is a 22-items self-report measure designed to assess current subjective distress for a specific traumatic life event. Respondents are asked to identify a specific stressful life event and then indicate how much they were distressed or bothered during the past seven days by it. In our survey, the stressful event to refer was the COVID-19 pandemic. The IES-R was constructed with three subscales: intrusions (e.g., repeated thoughts about the trauma), avoidance (e.g., effortful avoidance of situations that serve as reminders of the trauma) and physiological hyperarousal [45]. The IES-R total score provides an indication of the level of distress experienced and a higher score indicates a greater psychological impact [46, 47].
To measure Mental Health Status the “Depression, Anxiety and Stress Scale” (DASS-21) was administered [48,49]. The DASS-21 is a set of three self-report scales designed to measure the emotional states of depression, anxiety, and stress. The first subscale (DASS-Depression) measures loss of self-esteem/incentives and depressed mood. The second subscale (DASS-Anxiety) measures fear and anticipation of negative events. The third subscale (DASS-Stress) measures persistent state of overarousal and low frustration tolerance. The higher the score, the more severe the emotional distress was [50].
The principal difference between IES-R and DASS-21 (stress subscale) is that the former assesses the psychological impact of a specific traumatic event, while the latter does not identify any specific event. To clarify, we indicated the construct measured by IES-R (i.e. concerning a specific event) as “distress”, and that one measured by DASS-Stress subscale (i.e. do not related to any specific event) as “stress”.
Statistical analysis
Descriptive statistics were calculated for qualitative and quantitative variables. We performed binary logistic regression analyses to explore factors significantly associated with mild-to-severe psychological distress measured by IES-R as well as with mild-to-extremely severe levels of depression, anxiety, and stress measured by DASS-21. A two-tailed p value of less than 0.05 was considered statistically significant.
Due to high inter-correlations between the collected COVID-19 related variables, only univariate analyses were run for these factors.
All analyses were performed using the SPSS version 21.0 software package (SPSS Inc., Chicago, IL).
RESULTS
Demographic and clinical characteristics
A total of 98 Italian PLWH on cART completed the survey. Many of enrolled PLWH were male [75.5% (n=74)], aged 51 to 60 years [46% (n=45)], with upper secondary school’s degree [41% (n=40)] and employed [62.2% (n=61)].
Sixty-four (65.3%) and fifty-nine (60%) of respondents showed a time >10 years from HIV diagnosis and from first cART, respectively. Overall, 74.5% (n=73) of patients reported HIV-RNA<50 copies/mL and the mean adherence to cART was 9.48 (standard deviation, SD 1.10) on a 0-10 scale. Full demographic and clinical characteristics are summarized in Table 1.

Psychological impact and mental health evaluation
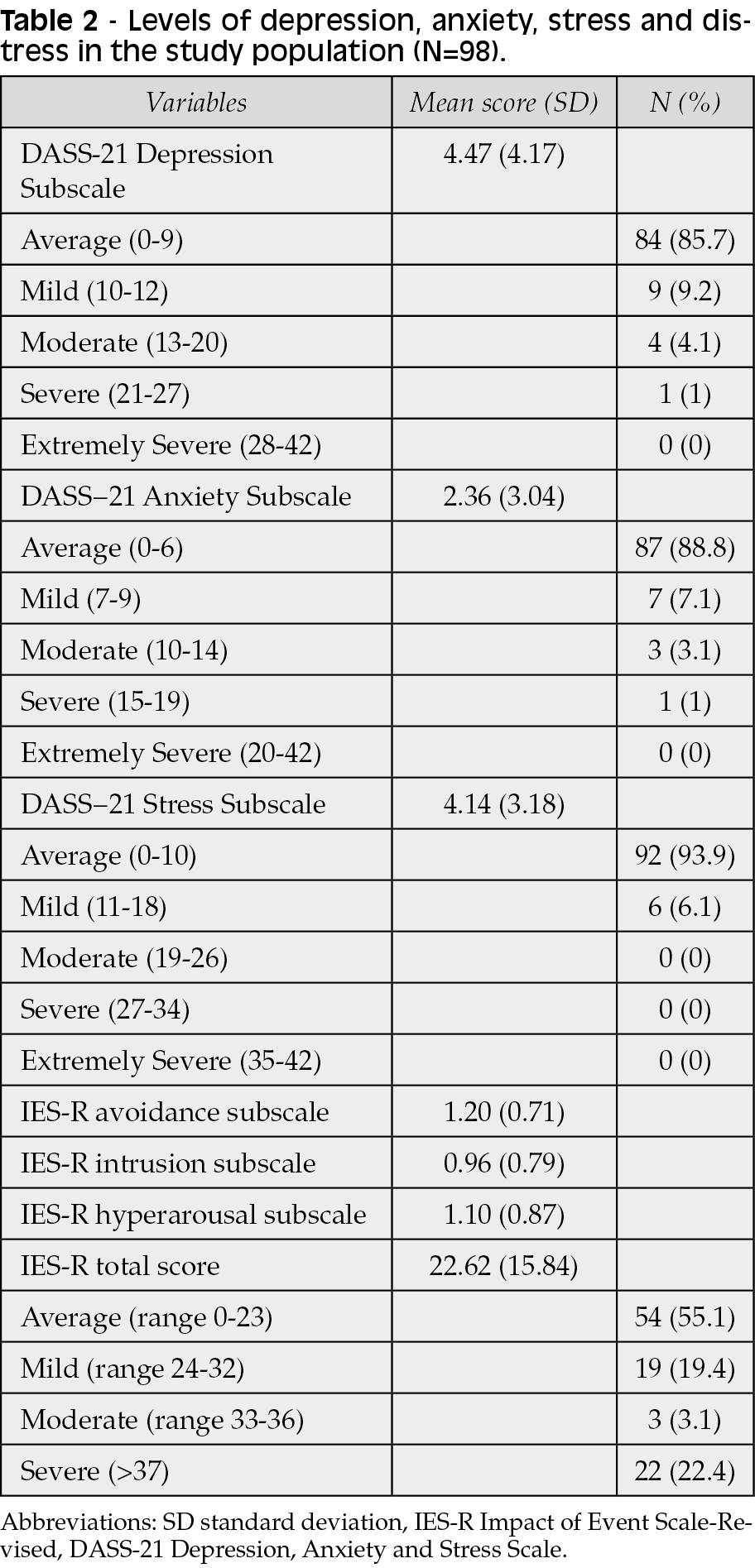
Overall, 45% (n=44) of PLWH revealed from mild to severe psychological impact of COVID-19 outbreak according to the IES-R. As regards the DASS-21, 14.3% (n=14), 11.2% (n=11) and 6.1% (n=6) of PLWH obtained a score suggesting the presence of mild to severe levels of depression, anxiety and stress, respectively; no patients obtained a score in the “extremely severe” range.
Complete descriptive statistics of IES-R and DASS-21 item scales are shown in Table 2.
Demographic and clinical factor associated to psychological impact and mental health evaluation
We explored factors associated to significant mild-to-severe levels of distress measured by IES-R, and to mild-to-severe levels of depression, anxiety and stress measured by DASS-21. For simplicity, only significant associations at multivariate analyses where reported.
In multivariate logistic regression analyses, female gender (OR 2.99; 95% confidence intervals [CI] 0.99/8.98; p=0.051) emerged as a risk factor for mild-to-severe levels of distress (IES-R), while ages 41 to 50 (OR 0.08; 95% CI 0.01/0.51; p=0.007) and 51 to 60 (OR 0.20; 95% CI 0.04/0.95; p=0.044) compared to be older than 60 years, a secondary (OR 0.17; 95%CI 0.03/0.99; p=0.049), upper (OR 0.12; 95%CI 0.02/0.65; p=0.014) and bachelors (OR 0.14; 95%CI 0.02/0.82; p=0.030) school degree compared to postgraduate degree, and being employed (OR 0.23; 95% CI 0.07/0.75; p=0.016) or retired (OR 0.12; 95% CI 0.01/0.79; p=0.028) compared to being unemployed resulted as protective factors.
Furthermore, a time between 5 and 10 years from HIV diagnosis was a significant risk factor for mild-to-severe levels of depression (DASS-21) (OR 10.02; 95% CI 2.39/41.95; p=0.002) compared to a time>10 years, and not be aware of own viremia emerged as risk factor for mild-to-severe levels of anxiety (DASS-21) (OR 6.15; 95% CI 1.23/30.61; p=0.027).
Others factors related to the severity of HIV infection (time from first cART, HIV-1 plasma viral load and adherence to cART in the last month) were not found to be associated with psychological impact and mental health evaluation.
Contact history variables and physical health status
A detailed description of contact history and physical health status is reported in Table 3.
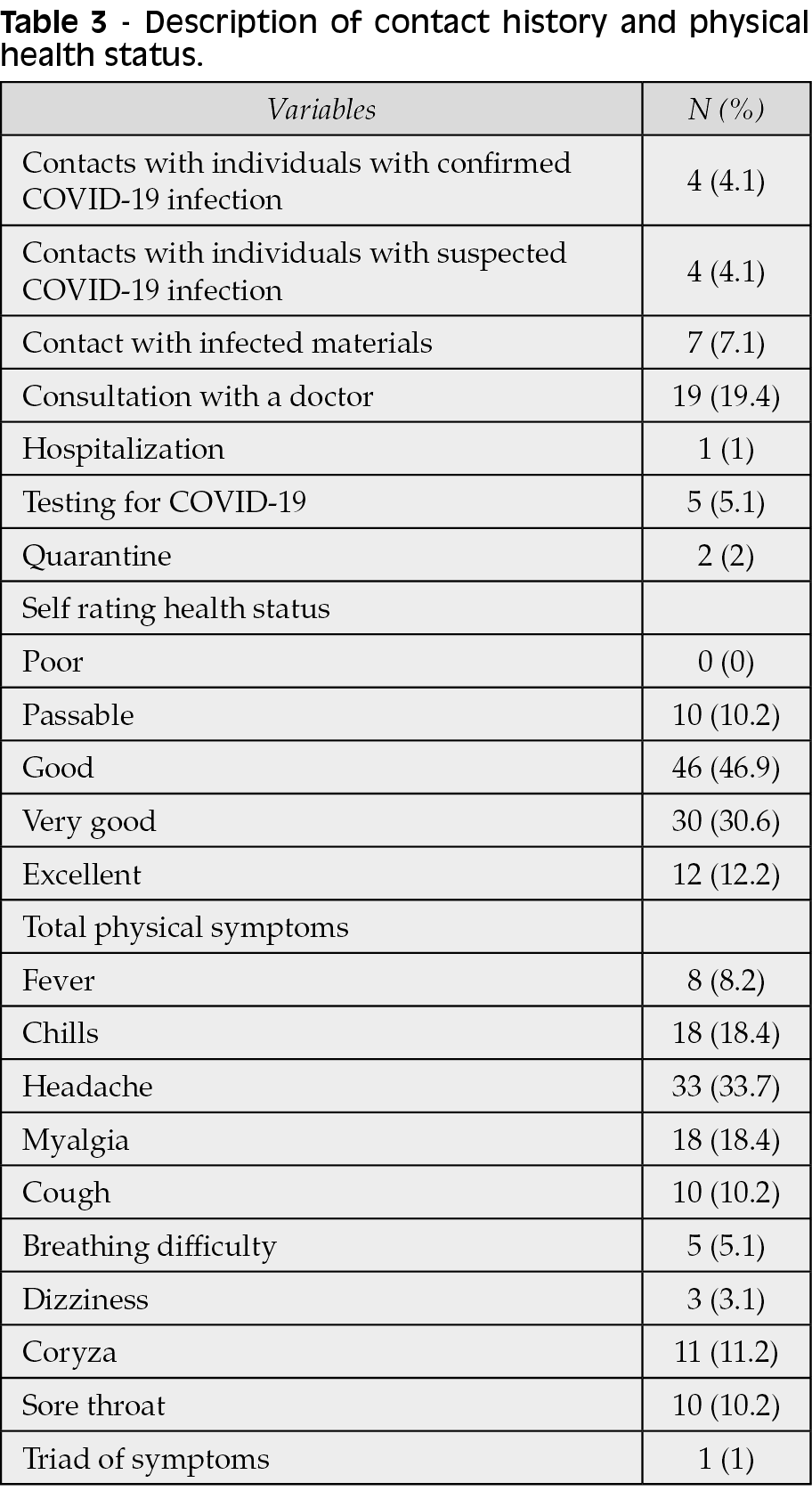
Only 4.1% (n=4) of participants had contacts with individuals with suspected or confirmed COVID-19 infection and 7.1% (n=7) with infected materials.
Seventy-six (77.5%) participants reported good or very good health status and only two (2%) had been under quarantine by a health authority. The most frequent physical symptom complained was headache (33.7%).
For conciseness, only significant associations at logistic univariate analyses where reported. Contact History variables seemed not significantly associated to IES-R and DASS-21 scores. Instead, when exploring Physical Health Status items, the number of possible COVID-19 physical symptoms was positively associated to the risk of mild-to-severe levels of psychological distress measured by IES-R (OR 1.42; 95% CI 1.07/1.88; p=0.014), and of mild-to-severe levels of depression (OR 1.40; 95% CI 1.03/1.90; p=0.032), anxiety (OR 1.50; 95% CI 1.08/2.09; p=0.016) and stress (OR 1.56; 95%CI 1.03/2.34; p=0.032) measured by DASS-21.
Knowledge and concerns about COVID-19 variables
A detailed description of Knowledge and Concerns about COVID-19 is reported in Table 4. About 94% (n=92) of the respondents usually kept themselves informed about COVID-19 outbreak. The most common source of health information was from television (59.2%, n=58) and the mean satisfaction with the amount of available health information was 6.48 (SD 2.08) on a 0-10 scale.
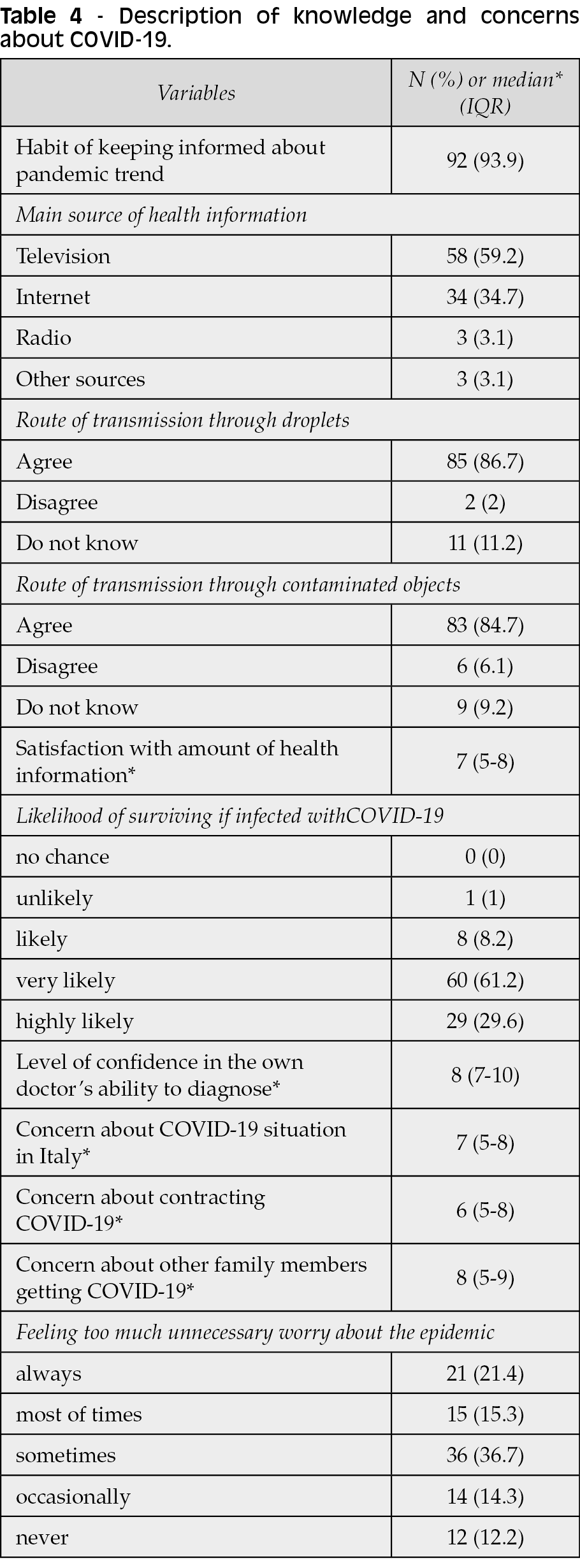
The majority of participants knew routes of transmission of COVID-19: 87% (n=85) agreed with route of transmission through droplets and 85% (n=83) through contaminated objects. About 61% (n=60) of subjects considered very likely surviving if infected with COVID-19.
Regarding COVID-19 pandemic concerns, mean concerns of situation in Italy was 6.39 (SD 2.47), and 37% (n=36) of respondents sometimes felt too much unnecessary worry about the epidemic.
For brevity, only significant associations at logistic univariate analyses where reported. Keeping themselves informed about COVID-19 outbreak was associated to a lower risk of mild-to-severe levels of depression measured by DASS-21 (OR 0.13; 95% CI 0.02/0.75; p=0.023), while greater concern to contract COVID-19 emerged as risk factor for mild-to-severe levels of psychological distress measured by IES-R (OR 1.23; 95%CI 1.04/1.45; p=0.012), and for mild-to-severe levels of depression (OR 1.35; 95% CI 1.03/1.78; p=0.028) and stress (OR 2.04; 95% CI 1.13/3.70; p=0.017) measured by DASS-21.
Moreover, wider concern about COVID-19 situation in Italy was associated to a higher risk of mild-to-severe psychological distress measured by IES-R (OR 1.29; 95% CI 1.07/1.55; p=0.007).
Precautionary measures variables
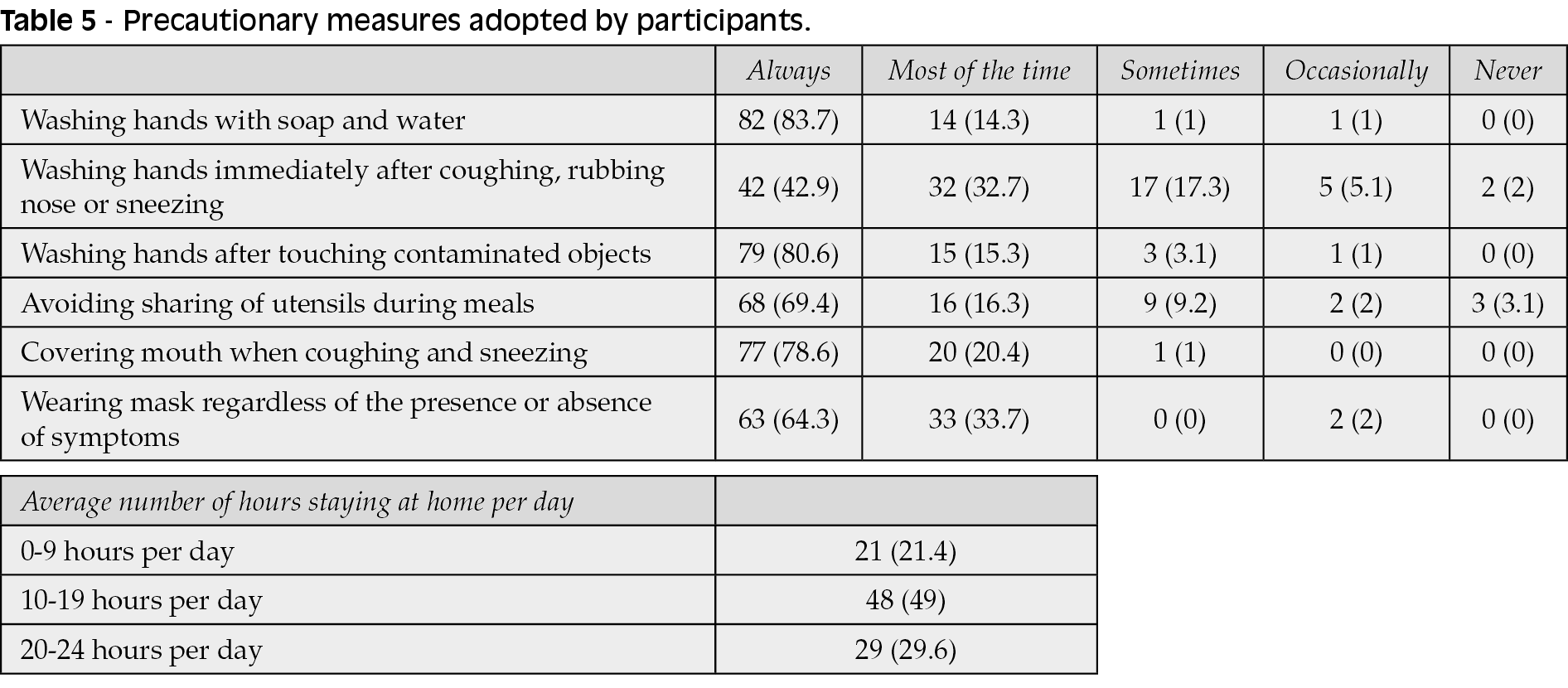
Table 5 - Details precautionary measures adopted by participants.
The two most frequently adopted precautionary measures were always washing hands with soap and water (84%, n=82), and always washing hands after touching contaminated objects (80%, n=79).
Precautionay measures variables seemed not significantly correlated to psychological distress levels measure by IES-R and depression, anxiety and stress levels measured by DASS-21.
Additional health information variables
Table 6 describes additional health information variables reported by participants. For simplicity, only significant associations at logistic univariate analyses where reported. Requiring further information on prevention of COVID-19 infection was associated to a higher risk for mild-to-severe levels of anxiety (OR 5.06; 95% CI 1.25/20.51; p=0.023) measured by DASS-21.
DISCUSSION
We found that, during the first 2 months after the beginning of COVID-19 pandemic in Italy, almost half of our cohort of PLWH suffered from mild to severe psychological distress according to the IES-R scale that measures emotional states referring to a specific event. This proportion is higher compared to that one observed in previous studies in the general population, confirming that PLWH might be a more fragile population needing a particular care [16, 20].
Similarly to a previous Chinese survey, a lower percentage of our sample complained elevated levels of depression, anxiety and stress as measured by the DASS-21, probably because this scale investigates emotional states that do not refer to a specific event and, consequently, it could be less sensitive in case of pandemic-related psychological impact [11].
According to previous evidence, we identified many factors associated with a higher risk of negative psychological impact of Covid-19 pandemic [3, 8, 11, 14, 16, 18, 19, 51]. To be more specific, we confirmed that female gender is associated with increased distress [52]. In addition, aging confirmed its negative association with mental health, probably because the physical distancing due to lockdown has exacerbated isolation and loneliness especially among elderly people [37, 53, 54]. In our study, higher education emerged as risk factor for distress: in literature, there are inconsistent results, indeed both high and low education levels have been found as possible risk factors for adverse psychological outcomes [3, 11, 13, 14]. As risk factor for distress we found also being unemployed, suggesting that pandemic’s disproportionate impact on people who are economically disadvantaged may have amplified pre-existing health disparities within the HIV epidemic [8]. Furthermore, a greater need of additional health information about COVID-19 prevention was associated to negative mental health outcomes, suggesting the usefulness of providing accurate health information during the epidemic to reduce the impact of rumors by government and health authorities [5]. On the other hand, PLWH who keep themselves informed about COVID-19 outbreak showed a lower risk of depression.
Higher number of possible COVID-19 physical symptoms, higher concerns about risk of contracting COVID-19 or regarding epidemic evolution in Italy were also identified as risk factor for adverse psychological impact.
Among HIV factors, fewer years from HIV diagnosis were associated with a higher risk of depression, maybe due to an increased mental health burden during the first years after HIV diagnosis, and not being aware of own viremia emerged as a risk factor for higher levels of anxiety. In other words, “those who perceive their own health as poor might feel more vulnerable when facing a new disease” [39, 55].
We have not found others factors related to the severity of HIV infection to be associated with mental health evaluation, maybe due to the high prevalence of patients with full adherence to cART and virally suppressed in our sample.
Taken together, our findings suggest that among PLWH women and elderly, and those one with recent HIV diagnosis might be at greater risk of distress from COVID-19 pandemic and might require particular care. To regularly monitor physical health and provide accurate information about COVID-19 pandemic appear important to prevent stress and anxiety.
We acknowledge that our study has some limitations. Firstly, this is a cross-sectional observation and future longitudinal studies are needed to confirm and check the progress of our findings. Secondly, further investigations including a HIV-negative control group would be useful to check for any differences in psychological impact or mental health status between PLWH and the general population. Moreover, reliability of self-administered questionnaires may be partially biased because of probable socially desirable responses. Furthermore, we used an online survey leaving unexplored the population who does not use network devices, and due to requirements on anonymity and confidentiality, we were not allowed to collect some personal information from the respondents. Therefore, since all of our patients were over 30 years old, further investigations including younger subjects are needed; however, an older sample is more representative of the current Italian HIV-infected population.
In conclusion, this study shows that almost half of an Italian cohort of PLWH experienced from mild to severe adverse psychological impact related to the first stage of COVID-19 pandemic. Our results describe a first picture of the psychological impact of COVID-19 on an Italian sample of PLWH. This overview could help to identify patients requiring support and highlights the importance to tailor specific psychological interventions to improve psychological wellbeing of PLWH, especially during a pandemic crisis.
Conflicts of interest
Alberto Borghetti fee for advisory board by ViiV Healthcare, personal fee by Janssen Cilag. Massimiliano Fabbiani received speakers’ honoraria and support for travel to meetings from Bristol-Myers Squibb (BMS), Gilead, Janssen-Cilag, Merck Sharp & Dohme (MSD), ViiV Healtcare, and fees for attending advisory boards from BMS, Gilead and Janssen-Cilag. Simona Di Giambenedetto received speakers’ honoraria and support for travel to meetings from Gilead, Janssen-Cilag (JC), Merck Sharp & Dohme (MSD) and ViiV Healtcare. All other authors: none to declare.
Funding
No funds, grants, or other support was received. No institution or funding has been used as the financial resource of this study.
Acknowledgement
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Valentina Delle Donne, Valentina Massaroni and Nicoletta Ciccarelli. The first draft of the manuscript was written by Valentina Delle Donne and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
REFERENCES
[1] Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry. 2020; 63 (1), e32.
[2] Kang L, Ma S, Chen M, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: a cross-sectional study. Brain Behav Immun. 2020; 87, 11-7.
[3] Talevi D, Socci V, Carai M, et al. Mental health outcomes of the CoViD-19 pandemic. Riv Psichiatr. 2020; 55 (3), 137-44.
[4] Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020; 395 (10227), 912-20.
[5] Rubin JG. The psychological effects of quarantining a city. BMJ. 2020; 368, m313.
[6] Duan L, Zhu G. Psychological interventions for people affected by the CoViD-19 epidemic. Lancet Psychiatry. 2020; 7 (4), 300-2.
[7] Ayittey FK, Ayittey MK, Chiwero NB, Kamasah JS, Dzuvor C. Economic impacts of Wuhan 2019-nCoV on China and the world. J Med Virol. 2020; 92 (5), 473-5.
[8] Chenneville T, Gabbidon K, Hanson P, Holyfield C. The Impact of COVID-19 on HIV Treatment and Research: A Call to Action. Int J Environ Res Public Health. 2020; 17 (12), 45-8.
[9] Li S, Wang Y, Xue J, Zhao N, Zhu T. The impact of CoViD-19 epidemic declaration on psychological consequences: a study on active weibo users. Int J Environ Res Public Health. 2020; 17 (6), 2032.
[10] Liu N, Zhang F, Wei C, et al. Prevalence and predictors of PTSS during COVID- 19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. 2020; 16 (287), 112921.
[11] Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020; 17 (5), 1729.
[12] Cao W, Fang Z, Hou G, et al. The psychological impact of the CoViD-19 epidemic on college students in China. Psychiatry Res. 2020; 287, 112934.
[13] Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implication and policy recommendations. Gen Psychiatr. 2020; 33 (2), e100213.
[14] Wang Y, Di Y, Ye J, Wei W. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID-19) in some regions of China. Psychol Health Med. 2020; 26 (1), 13-22.
[15] Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: A Cross-Sectional Study. Int J Environ Res Public Health. 2020; 17 (7), 2381.
[16] Moccia L, Janiri D, Pepe M, et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: an early report on the Italian general population. Brain Behav Immun. 2020; 87, 75-9.
[17] Jacobi F, Höfler M, Siegert J, et al. Twelve-month prevalence, comorbidity and correlates of mental disorders in Germany: The mental health module of the German health interview and examination survey for adults (DEGS1-MH). Int J Methods Psychiatr Res. 2014; 23 (3), 304-19.
[18] Mazza C, Ricci E, Biondi S, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020; 17 (9), 3165.
[19] Wittchen HU, Jacobi F, Rehm J, et al. The size and burden of mental disorders and other disorders of the brain in Europe. Eur Neuropsychopharmacol. 2010; 21 (9), 655-79.
[20] Rossi R, Socci V, Talevi D, et al. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front Psychiatry. 2020; 11, 790.
[21] Centers for Disease Control and Prevention (CDC). Coronavirus Disease 2019 (COVID-19) in People with HIV. Available at: https://www.cdc.gov/coronavirus/2019-ncov/specific-group s/hiv.html. [accessed 23 March 2020].
[22] Kowalska JD, Skrzat-Klapaczynska A, Bursa D, et al. HIV care in times of the COVID19 crisis - where are we now in Central and Eastern Europe? Int J Infect Dis. 2020; 96, 311-4.
[23] Ponticiello M, Mwanga-Amumpaire J, Tushemereirwe P, Nuwagaba G, Rachel King, Sundararajan R. “Everything is a mess”: how COVID-19 is impacting engagement with HIV testing Services in rural southwestern Uganda. AIDS Behav. 2020; 24 (11), 3006-9.
[24] Ballester-Arnal R, Gil-Llario MD. The virus that changed Spain: impact of COVID-19 on people with HIV. AIDS Behav. 2020; 24 (8), 2253-7.
[25] Lodge 2nd W, Kuchukhidze S. COVID-19, HIV, and migrant workers: the double burden of the two viruses. AIDS Patient Care STDS. 2020; 34 (6), 249-50.
[26] Prabhu S, Poongulali S, Kumarasamy N. Impact of COVID-19 on people living with HIV: A review. J Virus Erad. 2020; 6 (4), 100019.
[27] World Health Organization. 2019 Novel Coronavirus Global Research and Innovation Forum: Towards a Research Roadmap. 2020. Available at: https://www.who.int/who-documents-detail/2019-novelcoronavirus-overview-of-the-state-of-the-art-and-outline-of-key-knowledge-gaps-slides [accessed 27 April 2020].
[28] Nanni MG, Caruso R, Mitchell AJ, Meggiolaro E, Grassi L. Depression in HIV infected patients: A review. Curr Psychiatry Rep. 2015; 17 (1), 530.
[29] Bing EG, Burnam MA, Longshore D, et al. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch Gen Psychiatry. 2001; 58 (8), 721-8.
[30] Ciesla JA, Roberts JE. Meta-Analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001; 158 (5), 725-30.
[31] Nacher M, Adriouch L, Godard Sebillotte C, et al. Predictive factors and incidence of anxiety and depression in a cohort of HIV-positive patients in French Guiana. Aids Care. 2010; 22 (9), 1086-92.
[32] Gonzalez JS, Batchelder AW, Psaros C, Safren SA. Depression and HIV/AIDS treatment nonadherence: A review and meta-analysis. J Acquir Immune Defic Syndr. 2011; 58 (2), 181-7.
[33] Orban L, Stein R, Koenig L, et al. Coping strategies of adolescents living with HIV: Disease-specific stressors and responses. Aids Care. 2010; 22 (4), 420-30.
[34] Blashill AJ, Perry N, Safren SA. Mental health: A focus on stress, coping, and mental illness as it relates to treatment retention, adherence, and other health outcomes. Curr Hiv Aids Rep. 2011; 8 (4), 215-22.
[35] Singer M. Pathogen-pathogen interaction: a syndemic model of complex biosocial processes in disease. Virulence. 2010; 1 (1), 10-8.
[36] Halkitis PN, Moeller RW, Siconolfi DE, Storholm ED, Solomon TM, Bub KL. Measurement model exploring a syndemic in emerging adult gay and bisexual men. AIDS Behav. 2013; 17 (2), 662-73.
[37] Shiau S, Krause KD, Valera P, Swaminathan S, Halkitis PN. The Burden of COVID-19 in People Living with HIV: A Syndemic Perspective. AIDS Behav. 2020; 24 (8), 2244-9.
[38] Brandt C, Zvolensky MJ, Woods SP, Gonzalez A, Safren SA, O’Cleirigh CM. Anxiety symptoms and disorders among adults living with HIV and AIDS: A critical review and integrative synthesis of the empirical literature. Clin Psychol Rev. 2016; 51, 164-84.
[39] Lynn C, Bradley-Klug K, Chenneville TA, Walsh ASJ, Dedrick R, Rodriguez C. Mental health screening in integrated care settings: Identifying rates of depression, anxiety, and posttraumatic stress among youth with HIV. AIDS Care. 2018; 17 (3), 1-7.
[40] Gebo KA. Epidemiology of HIV and response to antiretroviral therapy in the middle aged and elderly. J Aging Health. 2008; 4 (6), 615-27.
[41] Nachega JB, Hsu AJ, Uthman OA, Spinewine A, Pham PA. Antiretroviral therapy adherence and drug-drug interactions in the aging HIV population. AIDS. 2012; 26 (1), S39-S53.
[42] Kuman TunÇel Ö, PullukÇu H, Erdem HA, Kurtaran B, Taşbakan SE, Taşbakan M 3. COVID-19 related anxiety in people living with HIV: An online cross-sectional study. Turk J Med Sci. 2020; 50 (8), 1792-1800.
[43] Siewe Fodjo JN, Faria de Moura Villela E, et al. Impact of the COVID-19 pandemic on the medical follow-up and psychosocial well-being of people living with HIV: A cross-sectional survey. J Acquir Immune Defic Syndr. 2020; 85 (3), 257-62.
[44] Christianson S, Marren J. The impact of event scale - Revised (IES-R). Medsurg Nurs 2012; 21 (5), 321-2.
[45] Gayle Beck J, Grant DM, Read JP, et al. The Impact of Event Scale-Revised: Psychometric properties in a sample of motor vehicle accident survivors. J Anxiety Disord. 2008; 22 (2), 187-98.
[46] Reynolds DL, Garay JR, Deamond SL, Moran MK, Gold W, Styra R. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiol Infect. 2008; 136 (7), 997-1007.
[47] Creamer M, Bell R, Failla S. Psychometric properties of the Impact of Event Scale-Revised. Behav Res Ther. 2003; 41 (12), 1489-96.
[48] Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005; 44 (2), 227-39.
[49] Norton PJ. Depression Anxiety and Stress Scales (DASS-21): psychometric analysis across four racial groups. Anxiety Stress Coping. 2007; 20 (3), 253-65.
[50] Oei T, Sawang S, Wah Goh Y, Mukhtar F. Using the Depression Anxiety Stress Scale 21 (DASS-21) across cultures. Int J Psycho. 2013; 48 (6), 1018-29.
[51] Ho CSH, Tan ELY, Ho RCM, Chiu MYL. Relationship of anxiety and depression with respiratory symptoms: Comparison between depressed and non-depressed smokers in Singapore. Int J Environ Res Public Health. 2019; 16 (1), 163.
[52] Sareen J, Erikson J, Medved MI, Asmundson GJ, et al. Risk factors for post-injury mental health problems. Depress Anxiety. 2013; 30 (4), 321-7.
[53] Armitage R, Nellums LB. COVID-19 and the consequences of isolating the elderly. Lancet Public. 2020; 5 (5), e256.
[54] Brooke J, Jackson D. Older people and COVID-19: Isolation, risk and ageism. J Clin Nurs. 2020; 29 (13-14), 2044-6.
[55] Hatch R, Young D, Barber V, Griffiths J, Harrison DA, Watkinson P. Anxiety, depression and post-traumatic stress disorder after critical illness: AUK-wide prospective cohort study. Crit. 2018; 22 (1), 310.