Le Infezioni in Medicina, n. 1, 46-53, 2021
ORIGINAL ARTICLES
Role of neutrophil-to-lymphocyte, lymphocyte-to-monocyte and platelet-to-lymphocyte ratios as predictors of disease severity in COVID-19 patients
Aleksandr Kalabin1, Vishnu Raj Kumar Mani1,2, Sebastian Cristobal Valdivieso1, Brian Donaldson1
1Columbia University College of Physicians and Surgeons at Harlem Hospital, New York, NY, USA;
2Duke University Medical Center, Durham, North Carolina, USA
Corresponding author
Aleksandr Kalabin
E-mail: kalabin.al@gmail.com
SummaRY
Direct viral damage and uncontrolled inflammation contribute to disease severity in SARS-CoV-2 infection. The aim of this study was to investigate the prognostic significance of neutrophil-to-lymphocyte [NLR], lymphocyte-to-monocyte [LMR] and platelet-to-lymphocyte [PLR] ratios in COVID-19 patients. All 184 COVID-19 patients hospitalized in our institution between March - April 2020 were retrospectively analyzed. The patients were grouped into intubated and non-intubated, and subgrouped into survived and deceased. An unpaired Student’s t-test was used for continuous variables, and the Pearson Chi-square (χ²) test for categorical. Univariate and multivariate logistic regression models were developed to assess the independent relationship between NLR, LMR and PLR and unfavorable outcomes. Non-parametric correlations were calculated using Spearman’s Rho correlation coefficient. The mean age of the patients was 64.7; mean BMI was 29.10; 73 (39.67%) were female and 111 male (60.33%). No statistical difference between groups was identified with regard to NLR (mean 8.29, standard deviation [SD] 7.86). On multivariate regression analysis, only PLR and LMR were shown to influence the ratio and it was positively correlated with PLR, lactate and C-reactive protein [CRP]. LMR for non-intubated survived [NI-S] (mean 2.29, SD 1.31) and non-intubated deceased [NI-D] (mean 1.79, SD 0.81) groups were statistically significant (p=0.03). LMR was influenced only by NLR on regression analysis. A positive correlation of LMR with body mass index [BMI] was ascertained. No statistical significance was found between groups for PLR (mean 269.85, SD 207.98) and the ratio was influenced by age and NLR on regression analysis, and positively correlated with NLR. To conclude, previously reported findings of a prognostic role of NLR, LMR and PLR in COVID-19 were not validated in our cohort and we would caution against using the ratios in question as independent markers for disease severity.
Keywords: COVID-19, neutrophil, lymphocyte, platelet, disease severity, prognostic markers.
INTRODUCTION
The ongoing global pandemic with SARS-CoV-2 infection has claimed more than a million lives with at least 45 million recorded infection as of date [1]. United States has been and continues to be the epicenter with infections steadily on the rise. There have been rampant advances in both clinical as well as basic science research into coronavirus, effectively assisting scientists, researchers and clinicians to combat the disease. As we gain more insight into the spectrum of COVID-19 disease, it is becoming clear that there is a complex interplay within the immune system initiated by the viral infection. In addition to direct viral damage, COVID-19 triggers uncontrolled and altered inflammatory response contributing to the severity associated with the disease [2]. The hyper-inflammatory response and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) results in major morbidity and mortality. This effectively translates in the sequelae of ensuing homeostatic derangements and organ failures. Biomarkers can serve as predictors of disease severity as well as indirect surrogate of treatment effectiveness. Derangements of various clinical biomarkers in patients with SARS-CoV-2 infection were recently reported, and diagnostic value of Neutrophil to Lymphocyte [NLR], Lymphocyte to Monocyte [LMR] and Platelet to Lymphocyte [PLR]1 ratios to assess disease severity was demonstrated [3-5]. The aim of this study was to investigate the prognostic significance of these ratios and their clinical utility in COVID-19 patients.
MATERIALS AND METHODS
Study design
Ethical approval from the hospital Institutional Review Board (IRB) for Health Sciences Research was expeditiously sought and approved. This retrospective study entails the clinical and laboratory characteristics of hospitalized patients with confirmed SARS-CoV-2 infection in March - April 2020.
Data collection
Data collection was done through review of Electronic Medical Records (EMR) for all parameters included in the study of patients confirmed with SARS-CoV-2 infection.
Inclusion and exclusion criteria
184 patients with confirmed SARS-CoV-2 infection and admitted to our facility during the study period were included. All other patients were excluded.
Patients were classified into four main groups: Non-intubated (NI-T) vs Intubated (I-T) patients and Survived (S) vs Deceased (D). We further subclassified NI-T group into Non-intubated Survived (NI-S) and Non-intubated Deceased (NI-D) as well as I-T group into Intubated-Survived (I-T) and Intubated-Deceased (I-D) groups. Patients defined as survived were alive at the time of data collection.
Outcomes
Primary outcome was to determine if NLR, LMR and PLR can serve as predictors of disease severity. Secondary outcomes were to assess the role of other inflammatory markers, mortality, percent of patients requiring mechanical ventilation and independent factors associated with disease severity.
Statistical analysis
Continuous variables were reported as mean values and standard deviation (SD), while categorical variables were expressed as counts and percentages. The statistical significance of intergroup differences was compared through unpaired Student’s t-test for continuous variables and through Pearson Chi-square (χ²) test for categorical variables. Univariate logistic regression analyses were performed to separately examine the association between unfavorable outcomes and each of the variables. Multivariate logistic regression models were conducted to determine the independent predictors adjusted for the previously specified baseline covariates. Criteria of p<0.05 for entry and p>0.10 for removal were imposed in this analysis. Nonparametric correlations between multiple continuous variables were calculated using Spearman’s Rho correlation coefficient. Two-sided p value <0.05 was considered to represent statistically significant difference. Microsoft Excel spreadsheet was used to display extrapolated data. JMP®, Version 15. SAS Institute Inc., Cary, NC, 1989-2019 was used for statistical analysis.
RESULTS
Patient characteristics
Mean age of our cohort was 64.7 (SD 14.87), range 28-97. Intubated patients tended to be younger (mean 59.57, SD 11.56) compared to their non-intubated counterparts (mean 65.75, SD 15.25) (p=0.03), however non-intubated Deceased patients were older (mean 74.05, SD 14.52) compared to non-intubated Survived subgroup (mean 64.58, SD 15.04) (p=0.01). 73 were females (39.67%) and 111 males (60.33%). Mean BMI was 29.10, range 13.38-61.68 kg/m2 (SD 7.39). Deceased people had a trend of lower BMI (mean 26.82, SD 5.77) compared to those who Survived (mean 29.60, SD 7.62) (p=0.03). On subgroup analysis BMI of NI-D group (mean 25.71, SD 6.12) was lower compared to BMI of NI-S (mean 29.00, SD 7.07) (p=0.04), and I-D patients had mean BMI of 28.57 (SD 4.19) compared to I-S group with mean BMI of 33.98 (SD 4.19) (p=0.03). Ethnic inclusions were 114 (61.96%) African-Americans, 58 (31.52%) Hispanic, 11 (5.98%) Asians and only 1 (0.54%) Caucasian (Table 1).

Primary outcomes
NLR (Neutrophil to Lymphocyte ratio). Mean NLR was 8.27 for NI-T (95% CI 6.99-9.56) versus 8.35 (95% CI 5.82-10.88) for I-T group (p=0.96). Comparison of S vs D groups revealed mean NLR of 8.01 (95% CI 6.72-9.28) and 9.58 (95% CI 6.88-12.28), respectively (p=0.29). Subgroup analysis of NI-T demonstrated that mean NLR of NI-S subgroup was 7.99 (95% CI 6.63-9.34), while for NI-D subgroup 10.31 (95% CI 6.13-14.49), (p=0.28). Analysis of I-T revealed no statistical significance: mean NLRs was 8.23 (95% CI 4.23-12.23) for I-S subgroup compared to 8.51 (95% CI 5.17-11.85) of I-D subgroup (p=0.91). The results of multivariate regression model (The Standard Least Square Personality) assessing the relationship of NLR and other continues variables, showed that only PLR (p<0.001) and LMR (p=0.001) were influencing the ratio. Nonparametric correlations between continuous variables were performed using Spearman’s Rho correlation coefficient and resultant heat map generated in figure [Figure 1a, 1b]. NLR was positively correlated with PLR (r=0.58, p<0.0001), Lactate (r=0.23, p=0.004), CRP (r=0.23, p=0.045) and negatively correlated with LMR (r=-0.54, p<0.0001). Correlations with Age (r=0.08, p=0.27), BMI (r= -0.13, p=0.08), Fever (r=-0.05, p=0.56) and Comorbidities (r=0.07, p=0.34) were not statistically significant.
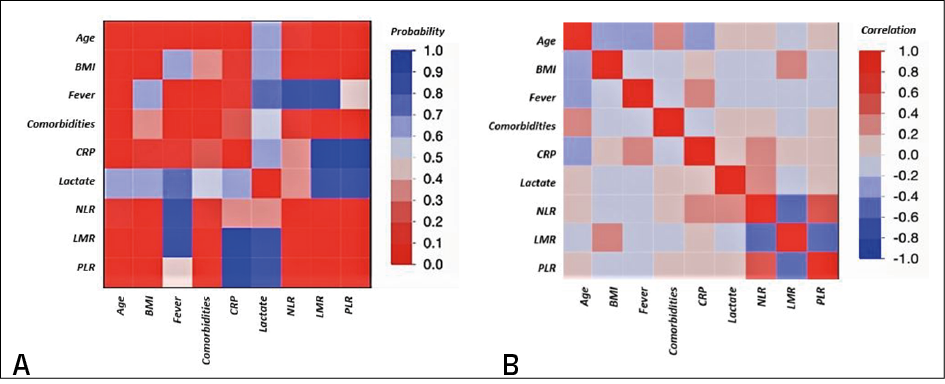
Figure 1 - Multivariate analysis of correlations. A) Color map on p values. B) Color map on Spearman’s coefficient.
BMI - Body Mass Index; CRP - C Reactive Protein; NLR - Neutrophil to Lymphocyte Ratio; LMR - Lymphocyte to Monocyte Ratio; PLR - Platelet to Lymphocyte Ratio.
LMR (Lymphocyte to Monocyte ratio). Mean LMR was 2.22 in NI-T (95% CI 2.02-2.43) versus 2.84 (95% CI 2.14-3.54) in I-T group (p=0.09). S group mean LMR was 2.34 (95% CI 2.12-2.56) and 2.25 (95% CI 1.72-2.78) for D group (p=0.75). Analysis of NI-S and NI-D groups revealed statistically significant difference (p=0.03) between mean LMRs: 2.29 (95% CI 2.06-2.51) and 1.79 (95% CI 1.39-2.18), respectively. No statistical difference was found in subgroup analysis of I-T group: mean LMR was 2.76 (95% CI 1.80-3.72) for I-S versus 2.93 (95% CI 1.76-4.11) for I-D, (p=0.81). Multivariate regression analysis for LMR revealed that only NLR (p=0.001) has statistically significant effect on the ratio compared to other variables. LMR was positively correlated with BMI (r=0.28, p=0.0002), negatively correlated with NLR (r=-0.53, p<0.0001), PLR (r=-0.42, p<0.0001) and comorbidities (r=-017, p=0.02). Correlations with Age (r=-0.14, p=0.05), Fever (r=-0.01, p=0.85), CRP (r=0.05, p=0.67) and Lactate (r=-0.06, p<0.48) were not statistically significant (Figure 1a, 1b).
PLR (Platelet to Lymphocyte ratio): Mean PLR of NI-T was 270.63 (95% CI 236.61-304.64) compared to 265.91 of I-T group (95% CI 199.04-332.78) (p=0.90). Analysis of mean PLRs of I-T group showed that the mean PLR of S group was 260.08 (95% CI 226.28-293.87) versus 316.32 in D group (95% CI 247.94-384.69) (p=0.14). Subgroup analysis of NI-T group revealed that the mean PLRs was 262.36 for NI-S (95% CI 226.34-298.38) versus 329.36 (95% CI 220.96-437.76) for NI-D group (p=0.23). No statistical difference was found between I-T subgroups: mean PLR for I-S was 241.94 (95% CI 133.57-350.31) versus 297.26 (95% CI 219.90-374.61) for I-D subgroup (p=0.38). Multivariate regression analysis for PLR revealed partake of only Age (p=0.005) and NLR (p<0.0001) in elucidating of PRL ratio. PLR was positively correlated with NLR and negatively with LMR as detailed above. Correlation with Age (r=0.07, p=0.34), Lactate (r= 0.05, p=0.53), BMI (r=-0.14, p=0.06), Fever (r=-0.01, p=0.87), CRP (r=0.04, p=0.70) and comorbidities (r=0.08, p=0.26) were not statistically significant [Figure 1a, 1b].
Secondary Outcomes
The overall mortality was 17.39%. Mortality among non-intubated was 12.34% where in those intubated it was as high as 43.33%.
Univariate logistic regression analysis for the association of each variable with unfavorable outcomes, namely intubation and death, were used to calculate R square and the odds ratio [Table 2]. Age (p=0.04, R square 0.03), BMI (p=0.04, R square 0.03), Fever (p=0.0005, R square 0.07), CRP (p=0.02, R square 0.06), Lactate (p=0.02, R square 0.03) and LMR (p=0.04, R square 0.03) were statistically significant indicative of predicting unfavorable outcome (intubation). NLR and PLR along with comorbidity score were not statistically significant and had low R square values. Fever (OR 1.77, 95% CI 1.15-2.72, p=0.004) and Lactate (OR 1.72, 95% CI 1.08-2.75, p=0.008) were independent predictors of intubation on multivariate logistic regression (Figure 2).
To analyze the associations of variables with death as an unfavorable outcome, we performed univariate logistic regression to obtain R square with odds ratio [Table 3]. BMI (p=0.04, R square 0.03), CRP (p=0.01, R square 0.08) and Lactate (p=0.01, R square 0.04) were statistically significant with greatest R square values. NLR, LMR and PLR values were not statistically significant, indicating no power of predicting death. Multivariate logistic regression to determine the independent predictors of death [Figure 3] was CRP (OR 1.05, 95% CI 1.00-1.10, p=0.03).
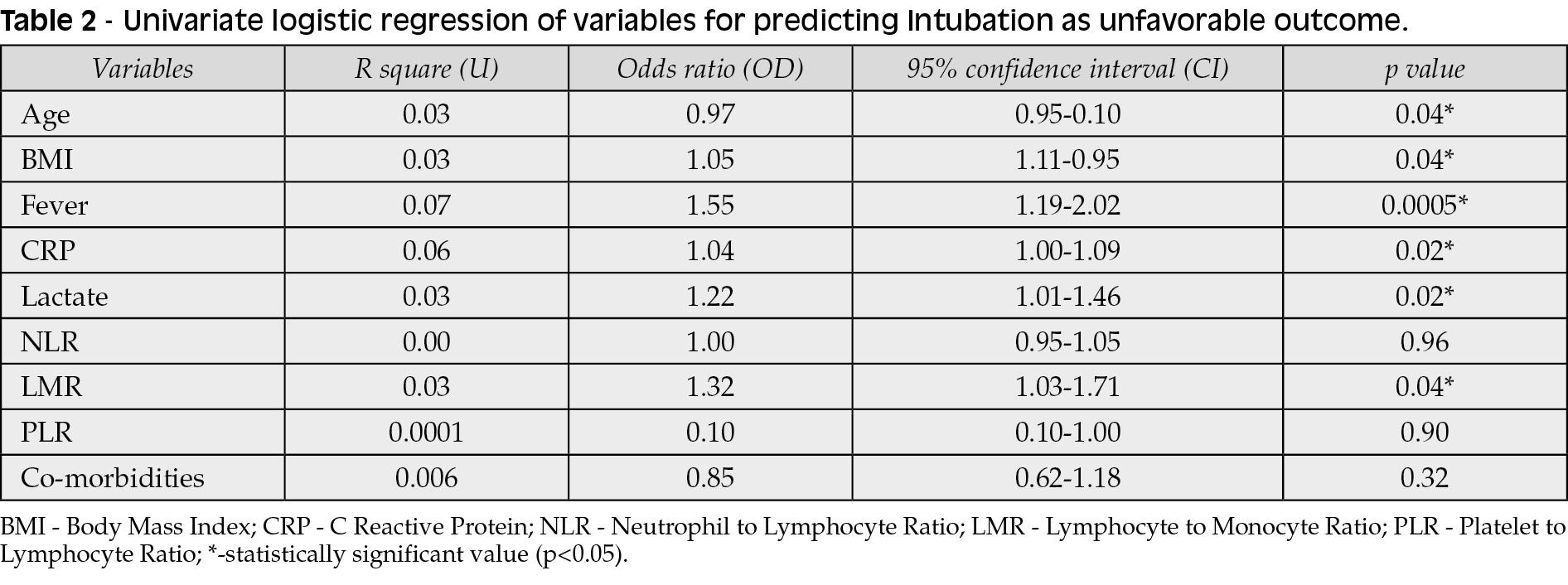
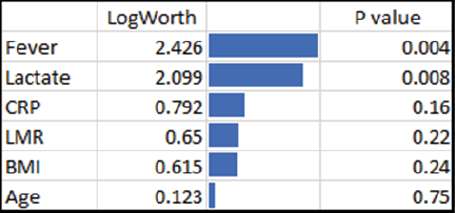
Figure 2 - Multivariate logistic regression model (Intubation). BMI - body mass index; CRP - C reactive protein; LMR - Lymphocyte to Monocyte ratio.

Figure 3 - Multivariate logistic regression model (Death).
CRP - C Reactive Protein; BMI - body mass index.

DISCUSSION
NLR, LMR and PLR are the ratios of main cell players orchestrating inflammatory response to infection or injury. Their significance is being investigated in wide variety of disease states, including malignancies [6-8]. A common aspect among it all is host’s immune response, activation of immune system by the disease states itself and/or altered immune defense mechanisms, as for example in autoimmune diseases. Each of these markers has been studied with different results. NLR elevation was found to be associated with poor outcomes in myocardial infarction, coronary artery disease, atherosclerosis, chronic obstructive pulmonary disease (COPD) and high nuclear grade renal cell carcinoma (RCC) [4, 9, 10]. LMR level has been correlated with several malignancies that might have complex interplay between immune system and oncogenesis. Their prognostic effectiveness has been investigated in hematological malignancies and solid tumors such as colon, bladder, and lung cancers [11]. Moreover, a recent study from Italy proved that COVID-19 patients had higher monocyte absolute count values compared to patients with flu, suggesting a potential prognostic role of monocyte - macrophages activation [12]. PLR and its potential to predict disease severity has been investigated in several neoplastic, prothrombotic and metabolic diseases, its role has been attributed to increased thrombogenic activity. PLR and NLR combination has found some interest in rheumatic disease, Behçet disease and familial Mediterranean fever as well as PLR and LMR combination in breast cancer [13, 14].
The clinical utility of PLR, LMR, NLR is not only related to their associations with inflammatory diseases and infectious states, but most importantly to the pragmatism and the ease with which they could be quantified and the frequency with which they could be monitored compared to any other test. Most importantly they are cost effective and will not affect through the already overburdened healthcare system. In light of this and the devastating nature of the ongoing pandemic which has already claimed more than a million lives, any tool that could predict or provide insight towards the severity of disease spectrum would help clinicians to identify those at most risk and to cater appropriate therapy.
Despite the fact that monocyte-derived macrophages are known to be the main players in inflammatory cascade in patients with COVID-19 infection, no studies to date have validated clinical usage of different monocyte assays [15]. On the other hand, studies from China by Liu et al. and Fu et al. indicated that NLR could be an independent predictor of the in-hospital mortality for COVID-19 patients and NLR levels can be served as a reliable prognostic tool in disease severity [4,16]. However, our findings do not replicate neither corroborate the previous results as our study did not show any clinical utility of these inflammatory markers.
Remarkably, NLR and PLR values were elevated at the baseline in our patients compared to healthy individuals suggesting sustained inflammatory/prothrombotic state in SARS-CoV-2 infection, consistent with previous studies [17, 18]. However, clinical associations of increased NLR and PLR values with disease severity and unfavorable outcomes were not meaningful. Only increased LMR values were associated with survival in non-intubated group of patients, probably indicating profound lymphocytopenia in non-survived patients. Nevertheless, these results clearly indicate that NLR, PLR and LMR could not be used as reliable markers of disease severity in COVID-19 patients.
Other findings of this study were consistent with previously published reports of COVID-19 associated hyperinflammation [2]. Conventional markers of inflammation including CRP, lactate and fever were elevated in a proportional fashion owing to the disease severity from low to high among those non-intubated to intubated to the deceased (Table 1). Even though the number of patients included in the intubated and the deceased subgroups was proportionally smaller, the overall mortality was lower for non-intubated and higher for intubated patients comparable to previous studies. Moreover, in our study mortality increased more than three times when patients required mechanical ventilation compared with those who did not indicating clear association of appalling inflammatory response with the disease severity [19].
It is also clear that older age, higher core body temperature, elevated CRP, lactate, LMR, BMI were associated with an increased likelihood of requiring mechanical ventilation among COVID-19 patients, which serves as an indirect surrogate of disease severity, placing patients on the far right of the disease spectrum. BMI, CRP and lactate were also associated with increased mortality in a proportional fashion, again feeding to our previous discussion on disease severity.
This study has certain limitations that need to be considered. First, this retrospective cohort study recruited only patients from a single institution. Second, it is essential to consider that, although inflammatory markers were quantified at a set point in time, each individual patient could have been at different stage of the disease spectrum.
In conclusion, our study could not validate neither replicate the finding of NLR and LMR as independent predictors of poor outcomes or mortality in SARS-Cov-2 infection. Furthermore, these results do not support any prognostic significance of these markers in COVID-19 patients and further research is needed to validate already available data or challenge ours.
Although we encourage clinicians to perform research to query the viability of NLR, LMR and PLR as prognostic inflammatory markers and bring forth their findings, we would caution them not to use these as independent markers for disease severity.
Conflicts of interest
None
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
We would like to acknowledge and thank the Infections Disease Department and Department of Surgery at Columbia University College of Physicians and Surgeons at Harlem Hospital.
REFERENCES
[1] https://coronavirus.jhu.edu/map.html; Last accessed 11/09/2020.
[2] Merad M, Martin JC. Pathological inflammation in patients with COVID-19: a key role for monocytes and macrophages. Nat Rev Immunol. 2020; 20 (6), 355-62.
[3] Mani VR, Kalabin A, Valdivieso SC, Murray-Ramcharan M, Donaldson B. New York Inner City Hospital COVID-19 Experience and Current Data: Retrospective Analysis at the Epicenter of the American Coronavirus Outbreak. J Med Internet Res. 2020; 18; 22 (9), e20548.
[4] Liu Y, Du X, Chen J, et al. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J Infect. 2020; 81 (1), e6-e12.
[5] Peng J, Qi D, Yuan G, et al. Diagnostic value of peripheral hematologic markers for coronavirus disease 2019 (COVID-19): A multicenter, cross-sectional study. J Clin Lab Anal. 2020; 34 (10), e23475.
[6] Diem S, Schmid S, Krapf M, et al. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer. 2017; 111, 176-81.
7. Duan J, Pan L, Yang M. Preoperative elevated neutrophil-to-lymphocyte ratio (NLR) and derived NLR are associated with poor prognosis in patients with breast cancer: A meta-analysis. Medicine (Baltimore). 2018; 97 (49), e13340.
[8] Hutterer GC, Stoeckigt C, Stojakovic T, et al. Low preoperative lymphocyte-monocyte ratio (LMR) represents a potentially poor prognostic factor in nonmetastatic clear cell renal cell carcinoma. Urol Oncol. 2014; 32 (7), 1041-8.
[9] Hu K, Lou L, Ye J, Zhang S. Prognostic role of the neutrophil-lymphocyte ratio in renal cell carcinoma: a meta-analysis. BMJ Open. 2015; 5 (4), e006404.
[10] Ye Z, Ai X, Liao Z, You C, Cheng Y. The prognostic values of neutrophil to lymphocyte ratio for outcomes in chronic obstructive pulmonary disease. Medicine (Baltimore). 2019; 98 (28): e16371.
[11] Gu L, Li H, Chen L, et al. Prognostic role of lymphocyte to monocyte ratio for patients with cancer: evidence from a systematic review and meta-analysis. Oncotarget. 2016; 7 (22), 31926-42.
[12] Curtolo A, Oliva A, Volpicelli L, et al. Monocyte absolute count as a preliminary tool to distinguish between SARS-CoV-2 and influenza A/B infections in patients requiring hospitalization. Infez Med. 2020; 28 (4), 534-8.
[13] Zhou X, Du Y, Huang Z, et al. Prognostic value of PLR in various cancers: a meta-analysis. PLoS One. 2014; 9 (6), e101119.
[14] Wang D, Bai N, Hu X, et al. Preoperative inflammatory markers of NLR and PLR as indicators of poor prognosis in resectable HCC. PeerJ. 2019; 7, e7132.
[15] Martinez FO, Combes TW, Orsenigo F, Gordon S. Monocyte activation in systemic Covid-19 infection: Assay and rationale. EBioMedicine. 2020; 59: 102964.
[16] Fu J, Kong J, Wang W, et al. The clinical implication of dynamic neutrophil to lymphocyte ratio and D-dimer in COVID-19: A retrospective study in Suzhou China. Thromb Res. 2020; 192, 3-8.
[17] Fest J, Ruiter R, Ikram MA, Voortman T, van Eijck CHJ, Stricker BH. Reference values for white blood-cell-based inflammatory markers in the Rotterdam Study: a population-based prospective cohort study. Sci Rep. 2018; 8 (1), 10566.
[18] Forget P, Khalifa C, Defour JP, Latinne D, Van Pel MC, De Kock M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res Notes. 2017; 10 (1), 12.
[19] Yehia BR, Winegar A, Fogel R, et al. Association of race with mortality among patients hospitalized with Coronavirus Disease 2019 (COVID-19) at 92 US Hospitals. JAMA Netw Open. 2020; 3 (8), e2018039.
1 NLR - Neutrophil to Lymphocyte ratio; LMR - Lymphocyte to Monocyte ratio; PLR - Platelet to Lymphocyte ratio.