Le Infezioni in Medicina, n. 1, 37-45, 2021
ORIGINAL ARTICLES
Alopecia and severity of COVID-19: a cross-sectional study in Peru
Miguel Ángel Salazar Arenas1, Agueda Muñoz del Carpio-Toia2, Johan Aybar Galdos1, Alfonso J. Rodriguez-Morales3,4
1Urology Service of Hospital Regional Honorio Delgado, Arequipa, Peru;
2Vice-rectorate of Research, Faculty of Human Medicine, Graduate School, Universidad Católica de Santa María, Arequipa, Peru;
3Public Health and Infection Research Group, Faculty of Health Sciences, Universidad Tecnologica de Pereira, Pereira, Risaralda, Colombia;
4Grupo de Investigación Biomedicina, Faculty of Medicine, Fundación Universitaria Autónoma de las Américas, Pereira, Risaralda, Colombia
Corresponding authors
Agueda Muñoz del Carpio-Toia
E-mail: amunozde@ucsm.edu.pe
Alfonso J. Rodriguez-Morales
E-mail: arodriguezm@utp.edu.co
SummaRY
The aim of this study was to determine the relationship between COVID-19 severity and androgenic alopecia in patients hospitalized in the Surgery Service of Honorio Delgado Espinoza Hospital in Arequipa, Peru. A cross-sectional study was performed in male patients with a diagnosis of COVID-19. Alopecia, clinical characteristics, treatment, and evolution were collected. In all, 98 patients were included; median age was 55 years old (range 18-89), 32.7% with comorbidities, and 45.9% with androgenic alopecia. The severity of COVID-19 infection was moderate to severe in 13.2% of patients without alopecia, and in 88.9% of patients with alopecia (p<0.001). In the logistic regression model analysis, patients with alopecia had a higher risk of presenting moderate to severe symptoms due to SARS-CoV-2 infection (OR: 80.2; 95% CI 16.2-397.7). In conclusion, the severity of infection was statistically significant in patients over 60 years old and those with alopecia.
Keywords: COVID-19, male, alopecia, severity, Peru.
INTRODUCTION
In December 2019, at Wuhan, Hubei, China, the first cases of an easily spread atypical pneumonia appeared, leading to an exhaustive investigation to find out the causative microorganism and to implement possible measures to contain the outbreak of this new disease, until it was determined that the causative agent was the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), a betacoronavirus [1-3].
The World Health Organization (WHO) soon declared the COVID-19 a public health problem of international concern and later a pandemic [4, 5].
The first studies published on clinical characterization of COVID-19 in China indicated that a higher percentage of patients affected were male, opening up a new research line to determine whether women were less susceptible to COVID-19 [6, 7]. A study in Lombardy, Italy, reported that 82% of the 1,591 patients admitted to the Intensive Care Unit (ICU) between February 20th and March 18th, 2020 were male [7]. Likewise, a clinical study of COVID-19 in Spain revealed that of 15,111 patients from 150 different hospitals, 57.2% were men [8]. In Italy it was observed that a higher burden of comorbidities, male sex, and advanced age were among the main determinants of a higher risk of death compared to China [9].
On the other hand, studies have observed that gender differences lie in the greater frequency of men infected with SARS-CoV-2, but they present more severe forms of the disease, with a worse prognosis [6,10]. Another study described a relationship between androgens and SARS-CoV-2, reporting that patients with prostate carcinoma treated with Androgen Deprivation Therapy (ADT) had four times lower risk of infections by COVID-19 compared to men who were not treated [11].
Regarding the sensitivity to androgens and COVID-19, the implications of the androgen receptor’s genetic variants are currently being analyzed, especially those related to androgenic alopecia. The variation of this receptor, which regulates the transmembrane protease serine 2 (TMPRSS2) transcription, seems to play an essential role in the host susceptibility and greater risk of severity for COVID-19 [12].
Another study’s preliminary results from Spain determined a high frequency of male pattern alopecia in 71% of patients hospitalized with the diagnosis of COVID-19 [13].
In Peru, there are also differences in the frequency and severity of the disease in regard to gender. As of January 24th, 2021, there have been 39,044 deaths from COVID-19, with a fatality rate of 3.6%, of which 68.18% are men and 31.82% women [14]. In Arequipa, Southern Peru, the second most important region and the one most severely affected by COVID-19, according to data from the Regional Health Management, 2,544 deaths have been registered, 29% of them women and 71% men [15]. Despite these figures, there is no characterization regarding other characteristics, such as alopecia at a national level.
Therefore, the aim of this study was to determine the association between the severity of COVID-19 and androgenic alopecia in patients hospitalized in the Surgery Service of the Honorio Delgado Espinoza Hospital (HRHDE), an institution of the Peruvian Ministry of Health (MINSA) in Arequipa, Peru.
PATIENTS AND METHODS
Study design and population
A cross-sectional study was carried out from July to September 2020 in the Men’s Surgery Service of Honorio Delgado Espinoza Hospital of the Peruvian Ministry Health in Arequipa, Peru. Patients with COVID-19 hospitalized in the General Surgery Service, were invited in an anonymous, confidential and voluntary manner to participate to the study, after obtaining informed consent,
Inclusion criteria were COVID-19 diagnosis confirmed by rapid test or molecular test for COVID-19, or suspected COVID-19 diagnosis by imaging (Thoracic Tomography or AP Chest X-ray).
Variables
Age, occupation, comorbidities, clinical evaluation (general condition, the reason for hospitalization, use of finasteride, alopecia, the severity of COVID-19), laboratory diagnosis of COVID-19 (rapid or molecular test), and progress (need for oxygen therapy, days of hospitalization, final evolution) were recorded. The Hamilton-Norwood scale was used for evaluating alopecia, considering patients with grade V to VII of the scale.
Statistical analysis
Data analysis was performed using Statistical Package for the Social Sciences (SPSS®) version 19. To evaluate the quantitative variables, distribution of frequencies and averages were used. Differences in the study variables were assessed using the Chi-square test; the logistic regression model, the risk by odds ratio (OR), with the 95% confidence intervals (95%CI) were calculated. A p value <0.05 was considered statistically significant.
Limitations
Data collection was complicated because the HRHDE Hospital in Arequipa Region belongs to the MINSA system. Due to the public system’s economic restrictions, the clinical records are not electronic, so all the evaluations had to be done directly with the patients. Ten clinical records were excluded due to incomplete data on the patient’s admission or evolution. However, this is the first study at the national level on the relationship between alopecia and severity of COVID-19, so our results could be used in future studies.
RESULTS
A total of 108 patients with SARS-CoV-2 were hospitalized in the surgery department from July to September 2020, but only 98 met the inclusion criteria and were included in this study. The hospitalization reasons were acute respiratory failure-pneumonia in 44.9% of patients, including two pneumothorax cases, trauma or fracture in 32.6%, acute appendicitis in 12.2%, and 10.2% for other clinical conditions. From the total, 98% of patients did rapid tests for COVID-19, of which 35.7% of patients had IgG+, 53.1% IgG+ plus IgM+, and 9.2% IgM+, and the remaining patient had a molecular test (2%). On physical examination, 45.9% of patients had alopecia (Table 1).

Clinical characteristics of patients
At hospitalization, the median age was 55 years (range 18 to 89), with the highest number of cases observed in patients over 60 years (30.6%), more than 57% were workers (dependent or independent and from other activities) and 32.7% presented comorbidity (66% had obesity, 18.8% hypertension, 18.8% diabetes mellitus and 9.3% other pulmonary problems). The general condition of patients was regular in 66.3%. The severity of SARS-CoV-2 infection was mild in 52% of patients, moderate in 12.2%, and severe in 35.7% (Table 1).
According to the condition of alopecia, 13.2% of patients without alopecia, and 51.1% with alopecia were over 60 years of age (p<0.001). 57% of patients without alopecia and 53.3% with alopecia were workers (p=0.035). From the total, 32.7% of patients without alopecia and 40.0% with alopecia had some comorbidity (p=0.225); the proportion of obesity, hypertension, and diabetes mellitus was very similar in both groups of patients (Table 1).
Patients’ general condition at hospitalization was bad in 88.7% and 40% of patients without and with alopecia, respectively. The cause of the hospitalization was acute respiratory failure - pneumonia or pneumothorax - in 13.2% of patients without alopecia and in 82.2% with alopecia, respectively (p<0.01), and trauma or fracture in 50.9% of patients without alopecia and 11.1% with alopecia, respectively (p<0.001). The severity of COVID-19 was moderate to severe in 13.2% of patients without alopecia and 88.9% of patients with alopecia, respectively (p<0.001) (Table 1).
The severity of COVID-19 according to clinical characteristics
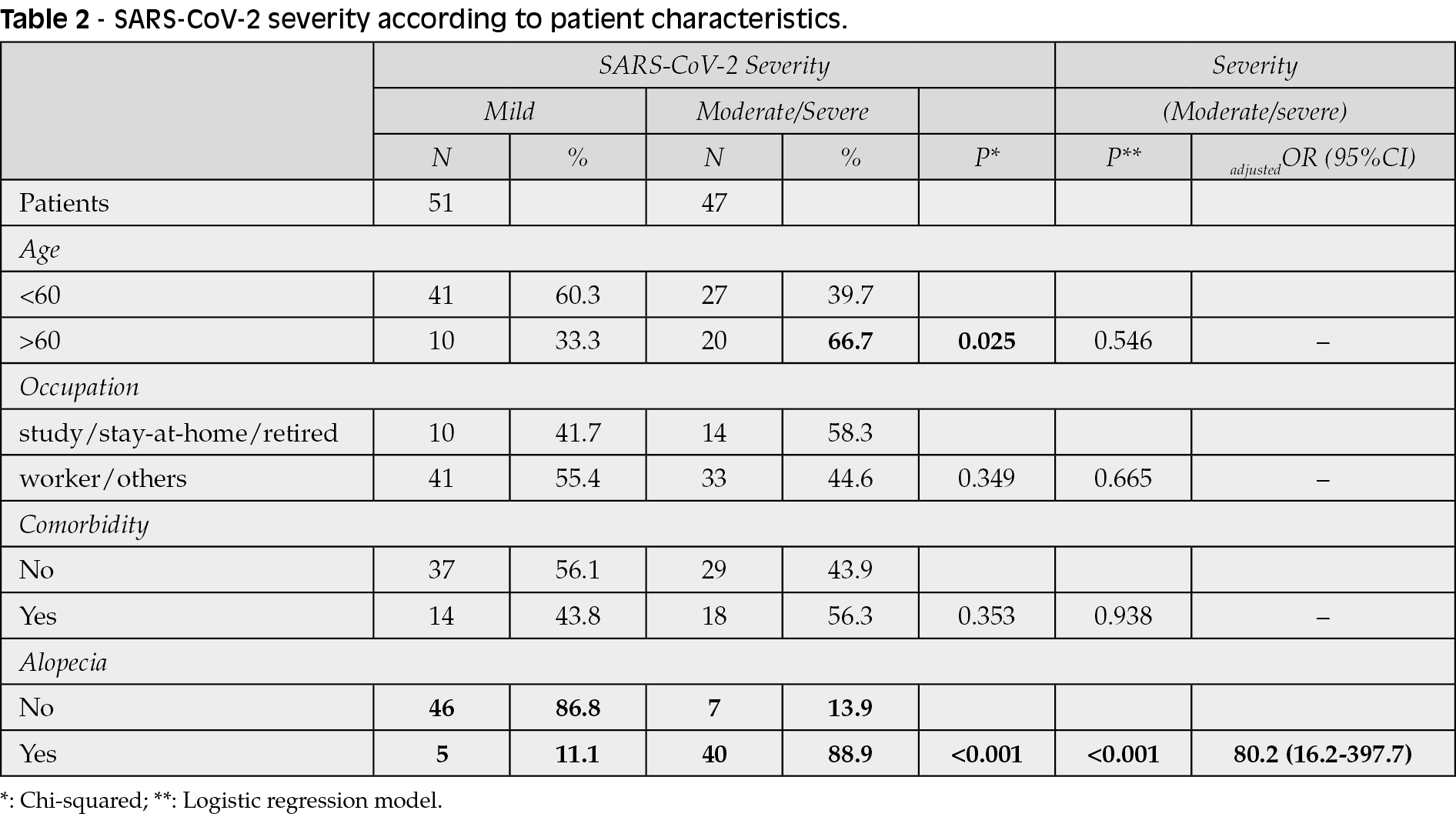
SARS-CoV-2 infection was moderate to severe in 39.7% of patients under 60 years old and 66.7% of patients over 60 years. Moreover, among patients with moderate to severe COVID-19, 58.3% were student/home-retired patients and 44.6% workers (dependent or independent, including other activities). The 56.2% of these patients presented comorbidity, and 88.9% were diagnosed with alopecia. The severity of infection was statistically significant in patients over 60 years old and in patients with alopecia (p<0.05). On the other hand, analyzing by the logistic regression model, patients with alopecia had a higher risk of presenting moderate to severe symptoms due to COVID-19 (OR: 80.2; 95% CI 16.2-397.7) (Table 2).
Treatment and evolution of patients
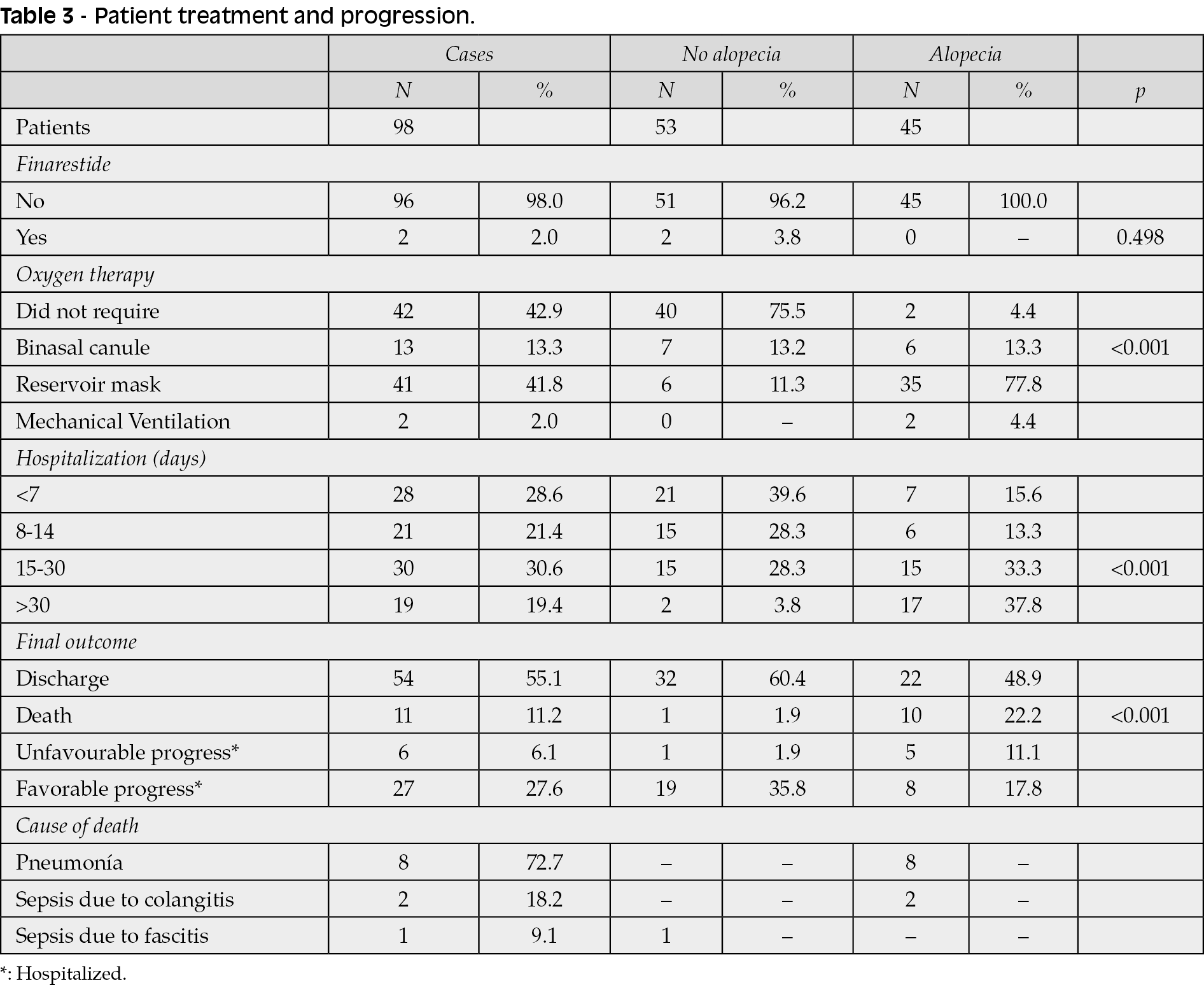
In total, 57.1% of patients required oxygen therapy. Among them, those patients without alopecia (24.5%) were significantly lower than those with alopecia (95.6%), (p<0.001). Of the total patients who received oxygen support, 73.2% had a reservoir mask, 13.3% a nasal cannula, and only two required mechanical ventilation. Hospital length of stay was less than or equal to 7 days in 28.6% of patients, between 8 and 14 days in 21.4%, and more than 14 days in 50% of patients. Among the patients hospitalized for more than 14 days, those without alopecia (32.1%) were significantly lower than those with alopecia (71.1%) (p<0.001) (Table 3).
At the date of the evaluation, 55.1% of the patients were discharged, 11.2% died, 6.1% of the patients were still hospitalized with unfavorable progress, 27.6% were still hospitalized with good progress. Patient who had died presented a significant difference according to the state of alopecia: 1.9% without alopecia and 22.2% with alopecia, respectively (p<0.001). The cause of death was mostly for pneumonia, followed by sepsis (Table 3).
The risk of death was associated with alopecia, age and severity of SARS-CoV-2 infection (p<0.001). 5.9% of patients under 60 years and 23.3% of patients over 60 years, and 3.9% with mild infection and 19.1% with moderate to severe infection died, respectively. However, when analyzed by the logistic regression model, none of these characteristics had a significant effect (p>0.05) on death’s risk (Table 4).
Nonetheless, according to the hospital length of stay and the outcome at discharge (alive or deceased), patients without alopecia had a better prognosis than patients with alopecia (p=0.023), and patients with mild symptoms of COVID-19 were of better prognosis than those with moderate to severe infection, although without significant difference (p=0.175). (Figures 1 and 2).


Figure 1 - Survival of patients hospitalized with COVID 19 according to the condition of alopecia.
DISCUSSION
The aim of this study was to evaluate the association between androgenetic alopecia and COVID-19 severity.
We evaluated 98 hospitalized patients with acute respiratory failure caused by SARS-CoV-2; 45.9% presented alopecia. Our results coincide with those from a study in Spain that identified a more significant loss of male pattern hair in patients with COVID-19; this finding revealed the potential role of androgens in the severity of COVID-19 [16].
We found that the severity of infection was statistically significant in patients over 60 years old and patients with alopecia (p<0.05). In the logistic regression analysis, patients with alopecia had a higher risk to present moderate to severe symptoms due to COVID-19 infection (OR: 80.2; 95% CI 16.2-397.7).
It has been almost ten months since the first cases of the disease were known, with different studies being published on the clinical and laboratory characteristics, associated factors, and evolution of COVID-19 disease. Those findings have determined a significant difference between the severity of infection and gender, being the men most affected. Thus, a study from China reported that 41.9% of COVID-19 patients were women, and 58.1% were men [6].
In a study conducted by Meng et al. significant differences were found between clinical characteristics, prognosis, and gender, with a greater involvement in males and a greater susceptibility associated to age and comorbidities. Hence, the authors suggest gender as an important biological variable in prevention and treatment strategies of COVID-19 [17]. Another meta-analysis that included 656 patients from 19 articles and 39 case reports on the characterization of COVID-19 revealed gender differences with greater frequency in males (55.9%) and also differences in the disease presentation and severity [18]. Another study conducted in Spain on the clinical evolution and factors associated with mortality in critical patients infected by SARS-CoV-2, found that older men had greater severity and prevalence of comorbidities such as hypertension, obesity, and diabetes [19]. Another study from Canada reported that male patients are more likely to be hospitalized, admitted to ICU (ORa =2.24; 95% CI =1.91-2.62; p<0.001) and die (ORa =1.70; 95% CI =1.54-1.88; p<0.001) [20].
Other studies have also analyzed the presence of androgenic alopecia in hospitalized patients and their severity. In this regard, a study showed that 79% of male patients hospitalized by COVID-19 in their centers had androgenic alopecia (diagnosed with the Hamilton-Norwood scale). A substantial proportion of them had severe COVID-19 [21].
In our study, according to the hospital length of stay and the outcome at discharge (alive or dead), we found that patients without alopecia had a better prognosis than patients with alopecia (p=0.023). These results corroborate those found by Andy Goren et al., that identified a relationship between increased male pattern hair loss and increased severity of COVID-19 [16]. Other authors hypothesized that these differences could be due to the correlation between the hyperandrogenic phenotype and the increase of the SARS-CoV-2 viral load, the increase of the viral dissemination, and the more severe presentation of pneumonia and associated lung problems [22-25].
Recently, some therapies used in the treatment of alopecia areata, such as the tofacitinib, Janus Kinase 3 inhibitor, have been recommended to be discontinued during the COVID-19 pandemic for an average of 80 days. A recent study evaluated the drug use and the SARS-CoV-2 infection status of alopecia areata patients concluding that the drug discontinuation due to the COVID-19 pandemic and recurrence was statistically significant (p<0.001). It is then suggested that the patients may continue to the tofacitinib therapy during the rest of the COVID-19 pandemic if the benefit outweigh the risk [26, 27].

Figure 2 - Survival of hospitalized patients according to COVID-19 severity.
Limitations
This is a cross-sectional study. Prospective cohort studies are needed to provide more solid evidence on the findings of this report.
In conclusion, it should be noted that throughout this pandemic, consistent evidence has been generated on the increased risk of men to suffer more severe presentations of COVID-19. However, we must also recognize that a single factor cannot yet explain these differences. On the contrary, it is estimated they are due to various biological factors, differences in immune response, differences in the increased expression of ACE2, present socio-cultural factors, behavior, among others [22-24]. Hence, these factors should be incorporated into new research and therapeutic plans. Our results conclude that the severity of infection by COVID-19 was moderate to severe in 88.9% of patients with alopecia (p<0.001). Also, patients who had alopecia were at greater risk of more severe presentations of COVID-19, and the severity of infection was statistically significant in patients over 60 years of age and patients who had alopecia (p<0.05). The risk of death was associated with age, alopecia, and severity of infection (p<0.001). COVID-19 represents an emotional challenge, with new clinical presentations and impact that should be considered and incorporated into the body of evidence related to the disease knowledge, given their multiple implications [25].
Finally, studies on COVID-19 must identify if these differences between genders persist, presenting the data disaggregated by sex. Likewise, we encourage new research considering the presence of alopecia.
Conflict of interest
None
Funding
None
Contributors
SAMA, AGJ, AMCT: conceptualization and execution of the research project, data analysis.
SAMA, AGJ, AMCT, AJRM: writing, reviewing, and approving the article’s final version.
Acknowledgement
A special thanks to each of the patients who collaborated with the study. We mostly appreciate the General Surgery Department of the Honorio Delgado Regional Hospital in Arequipa, Peru, for their outstanding collaboration in collecting data for this research.
Ethical considerations
The Research Ethics Committee approved the Universidad Católica Santa María’s study in Arequipa; it also complies with the Declaration of Helsinki’s ethical principles. Sensitive data of COVID-19 patients has been protected.
Databases
The databases used may be available upon request.
REFERENCES
[1] Mo P, Xing Y, Xiao Y, et al. Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China. Clin Infect Dis. 2020; doi: 10.1093/cid/ciaa270.
[2] Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel Coronavirus-infected pneumonia. N Engl J Med. 2020; 382 (13), 1199-207.
[3] Wu JT, Leung K, Bushman M, et al. Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China. Nat Med. 2020; 26 (4), 506-10.
[4] Mahase E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ. 2020; 368, m408.
[5] OMS, Alocución de apertura del Director General de la OMS en la rueda de prensa sobre la COVID-19 celebrada el 11 de marzo de 2020, (n.d.). https://www.who.int/es/dg/speeches/detail/who-director-general-sopening-remarks-at-the-media-briefing-on-covid-19---11-march-2020
[6] Guan W-J, Ni Z-Y, Hu Y, et al. Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med. 2020; 382 (18), 1708-20.
[7] Fu L, Wang B, Yuan T, et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J Infect. 2020; 80 (6), 656-65.
[8] Casas-Rojo JM, Antón-Santos JM, Millán-Núñez-Cortés J, et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: results from the SEMI-COVID-19 Registry. Rev Clin Esp. 2020; 220 (8), 480-94.
[9] Lippi G, Mattiuzzi C, Sanchis-Gomar F, Henry BM. Clinical and demographic characteristics of patients dying from COVID-19 in Italy versus China. J Med Virol. 2020; 92 (10), 1759-60.
[10] Ortolan A, Lorenzin M, Felicetti M, Doria A, Ramonda R. Does gender influence clinical expression and disease outcomes in COVID-19? A systematic review and meta-analysis. Int J Infect Dis. 2020; 99, 496-504.
[11] Montopoli M, Zumerle S, Vettor R, et al. Androgen-deprivation therapies for prostate cancer and risk of infection by SARS-CoV-2: a population-based study (n= 4532). Ann Oncol. 2020; 31 (8), 1040-5.
[12] Wambier CG, Goren A, Vaño-Galván S, et al. Androgen sensitivity gateway to COVID-19 disease severity. Drug Dev Res. 2020; 81 (7), 771-6.
[13] Goren A, Vaño-Galván S, Wambier CG, et al. A preliminary observation: Male pattern hair loss among hospitalized COVID-19 patients in Spain - A potential clue to the role of androgens in COVID-19 severity. J Cosmet Dermatol. 2020; 19 (7), 1545-7.
[14] Sala Situacional COVID 19 Perú 18 noviembre 2020. Disponible en: https://covid19.minsa.gob.pe/sala_situacional.asp
[15] Sala Situacional COVID 19 Arequipa Acceso 18 noviembre 2020. Disponible en: https://www.saludarequipa.gob.pe/epidemiologia/Covid19/COVID19.pdf
[16] Goren A, McCoy J, Wambier CG, et al. What does androgenetic alopecia have to do with COVID-19? An insight into a potential new therapy. Dermatol Ther. 2020; 33 (4), e13365.
[17] Meng Y, Wu P, Lu W, et al. Sex-specific clinical characteristics and prognosis of coronavirus disease-19 infection in Wuhan, China: A retrospective study of 168 severe patients. PLoS Pathog. 2020; 16 (4), e1008520.
[18] Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med Infect Dis. 2020; 34, 101623.
[19] Ferrando C, Mellado-Artigas R, Gea A, et al. Características, evolución clínica y factores asociados a la mortalidad en UCI de los pacientes críticos infectados por SARS-CoV-2 en España: estudio prospectivo, de cohorte y multicéntrico. Rev Esp Anestesiol Reanim. 2020; 67 (8), 425-37.
[20] Stall NM. Sex-and age-specific differences in COVID-19 testing, cases and outcomes: a population-wide study in Ontario, Canada. J Am Geriatr Soc. 2020; 68 (10), 2188-91.
[21] Wambier CG, Vaño-Galván S, McCoy J, et al. Androgenetic alopecia present in the majority of patients hospitalized with COVID-19: The “Gabrin sign”. J Am Acad Dermatol. 2020; 83 (2), 680-2.
[22] Wambier CG, Goren A. SARS-COV-2 infection is likely to be androgen mediated. J Am Acad Dermatol. 2020; 83 (1), 308-9.
[23] Bunders MJ, Altfeld M. Implications of sex differences in immunity for SARS-CoV-2 pathogenesis and design of therapeutic interventions. Immunity. 2020; 53 (3), 487-95.
[24] Klein SL, Dhakal S, Ursin RL, Deshpande S, Sandberg K, Mauvais-Jarvis F. Biological sex impacts COVID-19 outcomes. PLoS Pathog. 2020; 16 (6), e1008570.
[25] Dhama K, Khan S, Tiwari R, et al. Coronavirus Disease 2019-COVID-19. Clin Microbiol Rev. 2020; 33 (4), e00028-20.
[26] Aşkın Ö, Özkoca D, Uzunçakmak TK, Serdaroğlu S. Evaluation of the alopecia areata patients on tofacitinib treatment during the COVID-19 pandemic. Dermatol Ther. 2021; e14746.
[27] Perry T 2nd, Rosen H, Pettit C, Trinidad JC. Pressure-induced alopecia due to proning in COVID-19. Dermatol Ther. 2021; e14764.