Le Infezioni in Medicina, n. 1, 20-36, 2021
REVIEWS
COVID-19 pandemic: from origins to outcomes. A comprehensive review of viral pathogenesis, clinical manifestations, diagnostic evaluation, and management
Rohan Kumar Ochani1, Ameema Asad1, Farah Yasmin1, Shehryar Shaikh1, Hiba Khalid1, Simran Batra1, Muhammad Rizwan Sohail2, Syed Faisal Mahmood3, Rajkumar Ochani4, Mohammad Hussham Arshad5, Arjan Kumar6, Salim Surani7,8
1Department of Internal Medicine, Dow University of Health Sciences, Karachi, Pakistan;
2Division of Infectious Diseases, Baylor College of Medicine, Houston, Texas, USA;
3Section of Infectious Diseases, Department of Medicine, Aga Khan University, Karachi, Pakistan;
4Department of Anesthesiology, Australian Concept Infertility Medical Center, Karachi, Pakistan;
5Department of Internal Medicine, Aga Khan University, Karachi, Pakistan;
6Department of Medical ICU, Dr. Ruth K.M. Pfau Civil Hospital Karachi, Karachi, Pakistan;
7Department of Internal Medicine, Corpus Christi Medical Center, Corpus Christi, Texas, USA;
8Department of Internal Medicine, University of North Texas, Dallas, USA
Corresponding author
Rohan Kumar Ochani
E-mail: rohanochani@gmail.com
SummaRY
Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), the causative pathogen for the COVID-19, first emerged in Wuhan, China, in December 2019 and by March 2020, it was declared a pandemic. COVID-19 pandemic has overburdened healthcare systems in most countries and has led to massive economic losses. SARS-CoV-2 transmission typically occurs by respiratory droplets. The average incubation period is 6.4 days and presenting symptoms typically include fever, cough, dyspnea, myalgia or fatigue. While the majority of patients tend to have a mild illness, a minority of patients develop severe hypoxia requiring hospitalization and mechanical ventilation. Management is mostly supportive. However, several direct anti-viral agents, and immunomodulatory therapy with steroids and various cytokine blockers seem promising in early results. However, an effective vaccine has been established, which will help curb the pandemic.
Keywords: Bvnbmb
INTRODUCTION
The 2019 novel CoV, now named as Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) by the International Committee on Taxonomy of Viruses, belongs to the genus beta-CoV [1]. Beta-CoV also comprises of the Severe Acute Respiratory Syndrome CoV (SARS-CoV), and Middle Eastern Respiratory Syndrome CoV (MERS-CoV). On February 11th, 2020, the World Health Organization (WHO) announced a new name for disease caused by SARS-CoV-2: CoV disease (COVID-19), and exactly a month later, on March 11th, 2020, it was declared as a pandemic [1, 2].
SARS-CoV-2 first emerged in Wuhan, China, in December 2019, with the first case being linked to a seafood market [3, 4]. Since then, the virus has spread very rapidly, and as of January 17th, 2021, it has infected over 93 million people and has claimed over 2million lives [5]. Although the mortality rate of SARS-CoV-2 appears to be lower than SARS-CoV and MERS-CoV, it is transmitted much more quickly and widely in comparison, resulting in a global healthcare and financial crisis [6].
In this review, we summarize current knowledge about geographic distribution, virology, clinical manifestations, diagnosis, and management of COVID-19.
METHODS
A literature search was performed using PubMed/MEDLINE and Google Scholar from their inception until January 2021 using the following search string: “Coronavirus” AND “outbreak” OR “transmission” OR “geographical distribution’’ OR “virology” OR “pathogenesis” OR “genomic structure” OR “causality” OR “genomic distribution” OR “etiology” OR “clinical manifestation” OR “transmission” OR “diagnosis” OR “treatment” OR “prevention” OR “vaccination” OR “biosafety” OR “economic burden”. Articles in languages other than English were excluded.
GEOGRAPHICAL DISTRIBUTION
In December 2019, several patients with pneumonia of an unknown etiology were admitted to hospitals in Wuhan [3, 4]. According to a document published by WHO, 44 patients affected by of pneumonia of unknown etiology had been reported by January 3rd, 2020, with 11 patients severely ill. On January 8th, 2020, the genetic sequencing demonstrated a novel CoV as the potential causative organism [3, 7].
On March 11th, 2020, the WHO declared SARS-CoV-2 as a pandemic with confirmed cases in 114 countries [2]. By mid-March, Europe had more cases than anywhere in the world while COVID-19 had spread to more than 160 countries [8].
By the end of August 2020, the WHO region of Americas had the highest burden of COVID-19 globally, accounting for almost half of all new cases reported in the last week of August. The United States of America (USA) had the highest number of cases in the world; however, a decline in new cases was seen from previous peaks in July of over 70,000 cases per day to an average of 41,000 new cases per day [9].
A consistent increase in new cases and deaths was seen over the month of September 2020 in the Eastern Mediterranean Region with the highest number of new cases reported by Iraq, Iran and Morocco. The region of Americas continued to be the most affected WHO region with the USA, Brazil, Argentina and Colombia reporting the highest number of new cases in the last week of September. The number of new cases in the USA continued to rise and by the end of October, they started approaching the previous epidemic peak observed in July [10].
In December 2020, two new variants of SARS-CoV-2 were reported by the WHO, one by the authorities from the United Kingdom, referred as VOC 202012/01 and another detected in South Africa, named 501Y.V2. Initial analysis of these variants suggested that they may spread more rapidly [11].
As of January 17th, 2020, COVID-19 has affected a total of 93,217,287 people worldwide with 60 countries reporting imported cases or community transmission of the VOC 202012/01 variant and 23 countries reporting cases of the 501Y.V2 variant. Several ongoing studies are being conducted to determine the transmission and severity of these new variants [12].
The total numbers of cases, deaths, and recovered patients in the 20 leading countries are shown in Table 1, and Figures 1 and 2.


Figure 1 - Top 20 countries affected by COVID-19 (October 18, 2020).

Figure 2 - Deaths in the top 20 countries affected by COVID-19 (October 18, 2020).
VIROLOGY
CoV is an enormous group of viruses belonging to the Nidovirales order, which comprises of Coronaviridae, Roniviridae and Arteriviridae families. Crucial features are common to all the viruses of Nidovirales order, which means that all are enveloped, non-segmented positive-sense RNA viruses. Moreover, they all contain very large genomes for RNA viruses, and additional features include:
- a highly conserved genomic organization, with a large replicase gene preceding structural and accessory genes;
- expression of many non-structural genes by ribosomal frameshifting;
- several unique or unusual enzymatic activities encoded within the large replicase-transcriptase polyprotein;
- expression of downstream genes by the synthesis of 3′ nested sub-genomic mRNAs [13].
The CoV (one of two subfamilies in the Coronaviridae family) is subdivided into four groups based on serology: the alpha, beta, gamma, and delta CoVs [13]. Amongst these, the alpha-and beta viruses infect mammals, gamma CoV infect avian species, and delta CoV can infect the mammals as well as the avian species [14].
Structurally, CoVs form enveloped and spherical particles of 100-160 nm in diameter. The most notable characteristic of CoV is the club-shaped spike projections protruding from its surface. CoV has the largest identified RNA genomes, containing approximately 30 kilobase (kb) genomes. This is packed inside a helical capsid formed by the nucleocapsid (N) protein and then further surrounded by an envelope. Additionally the spike is an imperative determinant of viral host range and tissue tropism and a distinguished inducer of host immune responses [14, 15].
The Replication-Transcription Complex (RTC) has been investigated by Van Hemert MJ et al. [16]. The findings of the study concluded that viral RNA synthesis and intracellular membranes are functionally connected and, thus, consequently established that host factors play a prominent role in CoV RNA synthesis [16].
PATHOGENESIS
CoV’s four structural proteins, S, N, M, and E, enable the virus to gain access to the host cell [17, 18]. The S protein is heavily N-glycosylated, the M protein is present as a dimer in the virion, which maintains its shape and the E protein, a transmembrane protein with an Ion channel activity plays an important role in viral pathogenesis. This promotes the assembly and release of the virus from the host cell [19]. The N protein is only present in the nucleocapsid, which helps bind the viral genome with the NSP3 protein of the RTC and packages the RNA species produced during infection into the viral particles. It also serves as an antagonist of interferon (IFN), which appears to be beneficial for viral replication [20, 21]. Finally, the HE enhances the S protein binding activity and spread of the virus through the mucosa [22].
Following the initial attachment of the Receptor Binding Domain (RBD) of the S protein with its receptor, the virus enters the human cells. [23-25, 26].
Recent literature suggests that the high pathogenicity and transmissibility of SARS-CoV-2 could be attributed to the modified residues of RBD of S protein compared to SARS-CoV, presence of the polybasic furin cleavage site (RRAR) not observed in other coronaviruses. This facilities an effective cleavage of S protein by furin and other proteases. Additionally, the ‘S trimer’ exists in a partially opened state in highly pathogenic coronaviruses [27].
Following the viral entry into the host cell cytoplasm, the replication, transcription and the translation of the viral structural proteins, including M, E, and N proteins, occur, which are assembled into the virus and released via exocytosis. The S protein does not get assembled and directs the cell-cell fusion between infected cells leading to the formation of large multinucleated cells that go undetected by virus-specific antibodies, thus allowing the virus to spread within an infected organism [28].
The new SARS-CoV-2 uses the ACE2 receptor like the original SARS-CoV to facilitate viral entry into the target cells that leads to the downregulation of these receptors, and increased production of angiotensin-2 (AT2). Increased production of AT2 potentially increases pulmonary vascular permeability and may cause lung injury. Approximately 83% of the ACE2 receptors are expressed on the luminal surface of alveolar epithelial type II cells, making these as the primary reservoirs of viral invasion. Additionally, the multi-organ dysfunction observed in these patients can be attributed to the wide distribution of ACE2 receptors in extra-pulmonary tissues, including heart, kidney, endothelium, and intestine [29].
Pathological findings of a patient diagnosed with Acute Respiratory Distress Syndrome (ARDS) indicated diffuse alveolar damage with cellular fibromyxoid exudates and pulmonary edema, desquamation of pneumocytes, and hyaline membrane formation upon lung biopsy. Furthermore, the infiltration of interstitial mononuclear inflammatory infiltrates, dominated by lymphocytes, was also observed. The over activation of the T-cells leads to an increased concentration of pro-inflammatory cytokines released by the CD4 T-cells and higher amounts of cytotoxic granules in CD8 T-cells contributed to the severe immune injury in the patient. SARS-CoV-2 infects alveolar macrophages and epithelial cells that contain these viral particles and initiate lung inflammatory responses [30]. The clinical phase of SARS-CoV-2 can be categorized into three phases namely “viremia phase” in which the virus enters the peripheral blood from the lungs, “acute or the pneumonia phase” in which the immune-compromised individuals become severely critical with T lymphocytes and B lymphocytes significantly reduced while inflammatory cytokines mainly IL-6 and coagulation parameters such as D-Dimer are abnormally elevated in the “recovery phase”. As a result, Disseminated Intravascular Coagulation (DIC) due to inflammation and infection due to excessive activation of the coagulation cascade is observed [31]. Initial plasma levels of inflammatory cytokines in patients affected with SARS-CoV-2 is observed to be higher as compared to healthy adults. Chest CT scans in patients with viral pneumonia demonstrated ground-glass opacification with or without consolidative abnormalities which are more likely to be bilateral with a peripheral distribution involving the lower lobes of the lungs. Additionally, splenic atrophy, necrosis of hilar lymph nodes and focal hemorrhage in the kidney, liver enlargement with infiltration of inflammatory cells, edema and scattered neuronal degeneration in brain [32,33]. Furthermore, an autopsy study conducted by Wichmann et al. demonstrated a high incidence of Deep Venous Thrombosis (DVT) (58%) with one-third of COVID-19 patients having Pulmonary Embolism (PE) as a direct cause of death [34]. Lastly, the pathological mechanisms underlying myocardial injury in SARS-CoV-2 patients constitutes coronary spasm, hypoxic injury, microthrombi, direct vascular endothelial injury, hypercoagulability, and atherosclerotic plaque instability that increases the risk of developing acute myocardial infarction due to acute coronary occlusion [35]. Furthermore, olfactory dysfunction has also been reported in COVID-19 patients, however it still remains unclear whether the virus affects sensory cells or the olfactory bulb directly [36, 37]. The pathophysiology of SARS-CoV-2 is summarized in Figure 3.

Figure 3 - Pathophysiology of SARS-CoV-2.
Abbreviations: RBD; receptor binding protein, ACE-2; angiotensin converting enzyme-2 receptors, TMPRSS2; type 2 transmembrane serine protease, SARS-CoV-2, severe acute respiratory syndrome coronavirus-2, ARDS; acute respiratory distress syndrome, DVT, deep venous thrombosis, COVID-19; coronavirus disease-19.
TRANSMISSION
The newly identified SARS-CoV-2 has been suspected to extend to humans from bats through pangolins even though conclusive evidence in support of this is yet to be found [38].
After successful infection of a human host, further horizontal transmission of the SARS-CoV-2 occurs chiefly through human-to-human contact, either directly through respiratory droplets or indirectly by touching contaminated surfaces [39].
In addition, it has also been discovered that SARS-CoV-2 can remain airborne for up to 3 hours [39], increasing the risk of contracting the virus [39]. In regard to vertical transmission, maternal COVID-19 has a low likelihood for transmission to the newborn [39-41]. The presence of SARS-CoV-2 RNA in urine and feces has been detected leading to the implication of the fecal-oral route in its transmission as well; however, this route is considered to have a minor role only as the levels of the viral genetic material found in urine and feces is much lower than that in nasopharyngeal fluids [42].
Viral shedding by asymptomatic people is a major factor for ongoing transmission and may represent 25 to 50% of total new infections. This has led to the recommendation for universal masking [43]. Viral shedding may start 1 to 2 days before symptom onset and viral titers in respiratory secretions are noted to be highest in the early stages of infection with a quick decline soon after [44]. As already reported above, of recent concern is a new strain identified in the United Kingdom (UK) namely, SARS-CoV-2 VOC 202012/01 (Variant of Concern, year 2020, month 12, variant 01), as it is reported as having 75% more transmissibility and has spread to multiple countries outside of the UK [45, 46].
CLINICAL MANIFESTATIONS
Of the seven strains of H-CoV known, their potential to cause a respiratory tract disease ranges from mild to severe [47]. The incubation period, clinical presentation, and case fatality for each H-CoV are mentioned in Table 2.
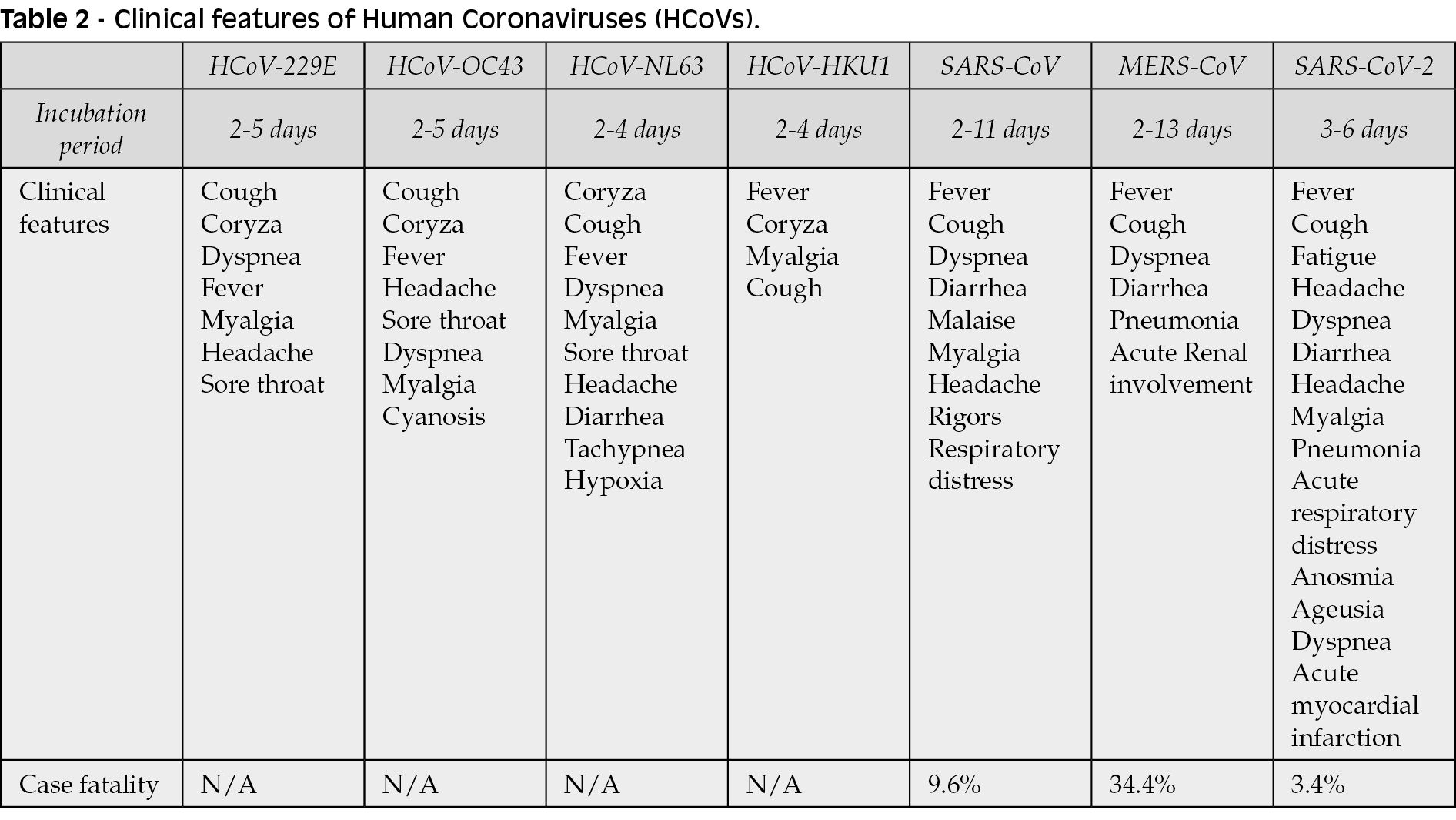
The most common complaints are fever, cough, and dyspnea, and less frequently gastrointestinal symptoms like diarrhea [48,49]. Older age group (65 years or older) is at higher risk of developing severe SARS-CoV-2 infection because of higher proportion of established co-morbidities [49]. However, younger adults are also being hospitalized with severe illness, albeit with much lower frequency. In a study by Zhang et al., SARS-CoV-2 infection was less likely in smokers, but the likelihood of the severity of disease upon infection in smokers may be higher [49]. Data from USA suggests that obesity may be considered as an independent risk factor for hospitalization and severe disease [50]. Children are less likely to develop symptomatic infection and are less prone to severe disease [51].
Furthermore, there have been reports of taste alterations and olfactory disturbances documented during the earlier course of the disease [52]. Additionally, cutaneous manifestations such as eryhtematous rashes and urticaria have also been reported in infected patients [53]. COVID-19 has also been associated with the involvement of the cardiovascular system [54-56]. Moreover, neurological manifestations such as headache, altered conscious state, dizziness, and acute cerebrovascular disease have also been exhibited by patients [57]. Regarding liver injury in COVID-19, multiple reasons such as drug-related hepatotoxicity and immune-mediated damage like cytokine storm have been suggested to play a role [58]. On studying the development of venous and arterial thrombotic events, most of the venous thromboembolic events were Pulmonary Embolisms (PEs) [59]. Moreover, there have also been reports of an increase in the number of children presenting with a disease termed Multisystem Inflammatory Syndrome in Children (MIS-C), thought to be a result of SARS-CoV-2 induced inflammation [60,61]. Lastly, opthalmological involvement is infrequent but it has been documented nevertheless; majorly as ocular pain, redness, and follicular conjunctivitis [62].
DIAGNOSIS
The diagnosis of CoV infection early in the course of the illness is essential to minimize the risk of large-scale outbreaks in hospitals and local communities [63].
The Center for Disease Control and Prevention (CDC) and WHO recommends respiratory specimens for SARS-CoV-2 nucleic acid amplification tests. Screening of asymptomatic patients is conducted using upper respiratory specimens such as nasopharyngeal (NP) swabs, oropharyngeal (OP), nasopharyngeal wash/aspirate or nasal aspirate (NA), throat swab while symptomatic patients or those with productive cough are screened via lower respiratory specimens such as sputum, a lower respiratory tract aspirate and bronchoalveolar lavage. In most cases, the sensitivity of NP swab PCR for COVID-19 is <80% depending on the assay used, sample procurement methods, and stage of illness. As the infection progresses from upper to lower respiratory tract, the sensitivity of NP swab further decreases but lower respiratory specimens such as bronchoalveolar lavage (BAL) may offer higher yields (80-90%) [60, 61]. Lastly, whole blood, urine and autopsy from deceased patients can also be used to detect the presence of virus [64]. Saliva is also highly applied for laboratory surveillance in busy clinical settings as it reduces waiting time for patients, and decreases the viral transmission risk to healthcare workers [65]. The rate of detection of respiratory viruses in saliva has been reported to be comparable to NP swabs [66]. The common factors affecting the accuracy of the results are shown in Figure 4.

Figure 4 - Factors affecting the accuracy of COVID-19 testing.
Methods for COVID-19 diagnosis
Electron Microscopy (EM) and cell culture
These two techniques are recommended by CDC for antiviral, and pathogenesis research, but not for clinical practice due to biosafety concerns. The culture and intubation of SARS-CoV-2 with cell lines such as Vero revealed cytopathic effects following six weeks of inoculation. EM allows the visualization of the virus, and ultra-structural details of viral-infected cells such as spherical particles with crown-like spikes in cell cultures of SARS-CoV-2 infected patients.
Real-time Reverse Transcriptase Polymerase Chain Reaction (RT_PCR)
Clinical specimens are obtained from nasopharyngeal swabs to extract the viral RNA, which then undergoes RT-PCR in an automated thermocycler with the master reaction mixture containing all the essential materials to generate a complementary DNA that is amplified and detected via gel electrophoresis [67]. However, this traditional technique is time-consuming and requires well-equipped lab environments with highly skilled expertise for diagnosis.
Many commercial and in-house assays have been developed based on varying number of gene targets and different target regions. Extensive research has been conducted to improve the RT-PCR assay such as the COVID-19-RdRp/Hel RT-PCR assay that has lower limit of detection (LoD) and greater specificity than the established RdRp-P2 assay for the detection of SARS-CoV-2 RNA in vitro and in patient specimen [68]. Another kind of assay, i.e. the COVID-19-nsp RT-PCR assay requires only one pair of SARS-CoV-2 primers specific towards nsp2 region which had not been previously targeted but highlighted by genome subtraction [69]. A very recent nucleic acid based test developed by CDC named as the Flu SC2 Multiplex Assay involves the simultaneous detection of SARS-CoV-2, influenza A, and influenza B. that allows for ongoing flu surveillance while also testing for SARS-CoV-2 [70].
Sample-to-answer assay
These tests include the Qiagen QIAstat-Dx Respiratory SARS-CoV-2 Panel, Abbott Diagnostics ID NOW COVID-19, BioFire Filmarray COVID-19, and Cepheid Xpert® Xpress recently authorized by US Food and Drug Administration for the emergency detection of SARS-CoV-2. These do not require the conventional complex PCR settings. These tests integrate the sample and nucleic acid extraction into a cartridge, the nucleic acid amplification and signal detection are also performed inside the closed cartridge, reducing the cross-contamination between samples, and increasing availability of molecular testing [71].
Serology testing (antibody detection)
Detection of a rise in the antibodies against the specific strains of CoV by Enzyme-Linked Immunosorbent Assay (ELISA) in the sera of patients obtained during either the acute or convalescent phase of the disease can be a rapid and secure method of diagnosis [72]. Che et al., observed N protein in the serum samples of the SARS-CoV patients after one day of the disease onset [73]. These N proteins can be used as antigens in ELISA for the detection of antibodies specific to SARS-CoV and several other animal CoV [74, 75].
The sensitivity and specificity of serologic tests are reported to vary. One study found the following serologic response to a recombinant SARS-CoV-2 nucleocapsid: IgM (85.4%), IgA (92.7%) observed 5 days following the symptom onset, and IgG (77.9%) observed 14 days after the onset of symptoms [76].
However, many currently offered serology tests for SARS-CoV-2 are not sufficiently clinically validated and FDA has warned not to use these tests yet to implicate authentic infection, protective immunity, or to rule out infection. Therefore, an active infection can only be ruled out with sensitive molecular (PCR) assays of respiratory secretions.
Computed Tomography (CT) scans
It enables the clinicians to observe the radiologic changes in the lungs, and diagnosis of lung lesions. The typical pattern of a CT scan of COVID-19 infected patient demonstrates ground-glass opacity with consolidation, bilateral patchy shadowing, and peripheral distribution with rare pleural effusion, and lymphadenopathy [77,78]. During later stages of infection, crazy-paving patterns develop and consolidation of the lungs increases the absorption of lesions [79]. The sensitivity of the COVID-19 testing is remarkably increased with a combination of RT-PCR and Chest CT scan [80].
MANAGEMENT AND TREATMENT
Supportive treatments
Supportive care remains the cornerstone of COVID-19 treatment. Oxygen therapy comprises the primary treatment intervention for patients with severe infection. Mechanical ventilation is essential in cases of respiratory failure refractory to oxygen therapy, whereas hemodynamic support is required for managing septic shock [81]. Other supportive measures include fluid management and administration of antimicrobials to treat secondary infections. Many direct antiviral drugs to control the SARS-CoV-2 replication and immunomodulatory agents to control cytokine storm and resultant inflammation are being investigated in clinical trials with some early promising results.
Antiviral agents
Chloroquine (CQ) or hydroxychloroquine (HCQ) were initially reported to have anti-viral activity against SARS-CoV-2. However, in the WHO SOLIDARITY trial, an open-label, randomized trial being conducted to identify drugs that can be repurposed for use against COVID-19, HCQ was discountinued as it did not show any definite effect on mortality [82].
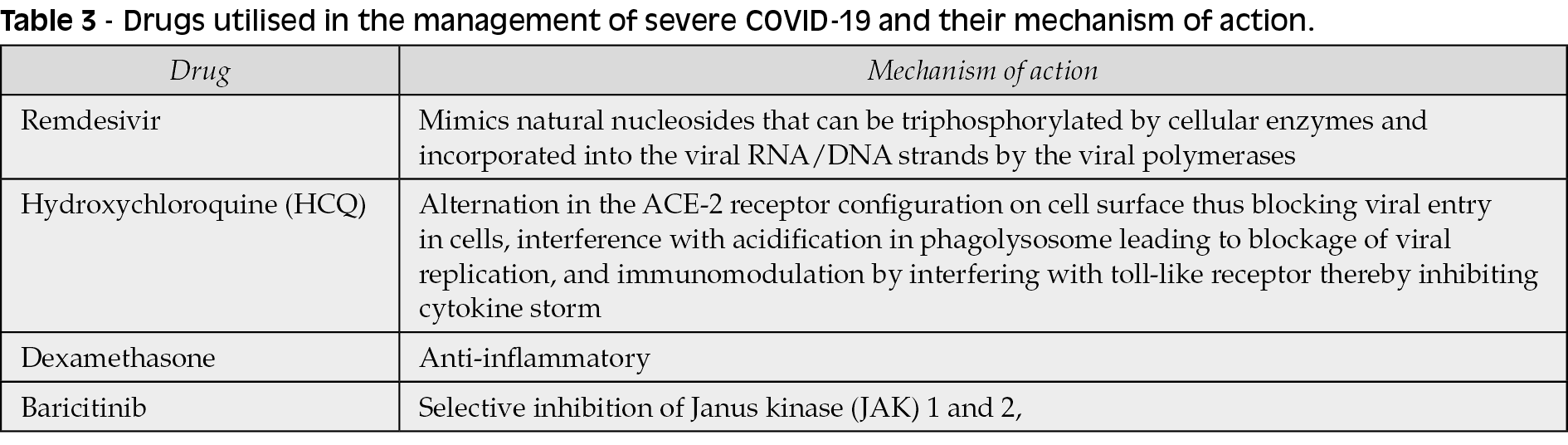
One promising antiviral drug remdesivir, an adenosine analog, is currently undergoing several clinical trials. It is a broad-spectrum antiviral drug. The mechanism of action of remdesivir mimics natural nucleosides that can be triphosphorylated by cellular enzymes and incorporated into the viral RNA/DNA strands by the viral polymerases. Remdesivir was initially developed to treat Ebola virus disease but exhibits activity against many RNA viruses such as RSV and the coronaviruses (including MERS-CoV and SARS-CoV) [83].
Preliminary results of an NIH-sponsored randomized placebo-controlled clinical trial of remdesivir (ACTT; NCT04280705) for COVID-19 patients with evidence of lung involvement showed that patients who received Remdesivir had median time to recovery 11 days vs. 15 days with a placebo [84]. The survival benefit was noted but was not statistically significant. In the SOLIDARITY trial however, remdesivir was shown to have little to no effect on hospitalized patients with COVID-19. Based on this trial and three other randomized controlled trials, the WHO issued a conditional recommendation against the use of remdesivir in hospitalized patients on November 20th, 2020 [85].
Along with HCQ and Remdesivir, the SOLIDARITY trial also included lopinavir and interferon beta-1a but they were also eventually discontinued [82].
Furthermore, baricitinib, an antiinflammatory drug that acts by selective inhibition of Janus kinase (JAK) 1 and 2, was predicted to be a potential therapeutic against SAR-CoV-2. It was associated with an improvement in oxygenation and a reduction in select inflammatory markers in three case series. Therefore, similar to the ACTT-1 for remdesivir, a double blind, placebo controlled trial was conducted to compare the combination of baricitinib plus remdesivir to remdesivir alone. Out of 1,033 patients, 515 recived the combination therapy which was shown to have a 1-day shorter time to recovery and a greater improvement in clinical status, notably among those receiving high-flow oxygen or non-invasive ventilation. Based on the results of this trial, the FDA issued an emergency authorization of this combination therapy on November 19th 2020, for the treatment of suspected or laboratory confirmed COVID-19 patients requiring supplemental oxygen, invasive mechanical ventilation, or ExtraCorporeal Membrane Oxygenation (ECMO); however, baricitinib is not authorized as a stand alone treatment [86, 87].
NIH and IDSA COVID-19 treatment guidelines recommend remdesivir for hospitalized patients with SpO2 ≤94% on room air or those who require supplemental oxygen [88, 89]. NIH panel also recommends baricitinib in combination with remdesivir for treatment of COVID-19 in patients who are on mechanical ventilation or ECMO. Treatment duration in patients with severe COVID-19, who are not intubated, is 5 days. For patients who are mechanically ventilated or on ECMO, 10 days of remdesivir is recommended. The mechanism of action of drugs used in the management of COVID-19 are briefly reported in Table 3.
Insufficient data is available on the optimal therapy duration for patients on mechanical ventilation and ECMO, or patients who have not demonstrated adequate improvement after 5 days of therapy. In these patients, some experts prolong the total remdesivir therapy duration to up to 10 days (CIII).
Limited data is available for experts to recommend in favor of or against remdesivir for the treatment of patients with mild to moderate symptoms of COVID-19.
Immunomodulatory agents
Tocilizumab, an FDA-authorized anti-IL6R agent has been widely studied. A randomized controlled trial published in The New England Journal of Medicine studied the effects of tocilizumab on 389 patients.The trial concluded that patients hospitalized with COVID-19 pneumonia, not receiving mechanical ventilation, showed decreased advancement to the composite outcome of mechanical ventilation or death with the use of tocilizumab; however, it did not improve survival [90]. Also, preliminary findings of a French trial comparing tocilizumab plus standard treatment to standard treatment alone administered to a sample of 129 non-ICU hospitalized COVID-19 patients and those with moderate/severe pneumonia indicated that tocilizumab resulted in a decreased rate of non-invasive or mechanical ventilation in comparison to placebo [91].
Other potential drugs under investigation include Sarilumab (anti-IL6R), Siltuximab (anti-IL6), Anakinra (anti-IL1), anti-GM-CSF agents, and monoclonal antibodies, specific to SARS-CoV-2.
Convalescent plasma
A SARS-CoV-specific human monoclonal antibody, CR3022, was reported to bind potently with the SARS-CoV-2 receptor-binding domain (KD of 6.3 nM) [92].
A recent RCT, the PLACID trial, conducted across 39 teritiary care hospitals in India, compared patients with moderate COVID-19 treated with convalescent plasma along with best standard of care to those who received best standard care alone. No difference in 28 day mortality or progression to severe disease was noted between the two groups although treatment with convalescent plasma was associated with a higher resolution of shortness of breath and fatigue on day 7 post-enrolment [93].
FDA has approved an Emergency Investigational New Drug (eIND) for expanded access for convalescent plasma. However, the administration of convalescent plasma is not without risk. These risks include pathogen transmission (nearly 1 per 2 million transfusions for HIV/HBV/HCV), Transfusion-Associated Circulatory Overload (TACO), allergic transfusion reactions, and Transfusion-Related Acute Lung Injury (TRALI). In a study to analyze adverse affects of convalescent plasma administration in 5,000 hospitalized adults with severe or life-threatening COVID-19, 36 Serious Adverse Events (SAEs) were reported within four hours of completion of transfusion. However, the seven-day mortality rate was estimated to be 14.9% which was higher than the crude estimate of 12.0% [94].
Pooled Intravenous Immunoglobulin (IVIG) is proposed as an intervention in the setting of viral-induced lung injury/ARDS. It reduces immune responses through many mechanisms such as reducing interrupting complement cascade, diminished activated CD4+, and cytotoxic CD8+ T cells. However, no clinical trial data to back use in COVID-19 thus far.
Corticosteroids
In a study to investigate the pathological characteristics of a patient who died from severe infection with SARS-CoV-2 by postmortem biopsies, it was suggested that timely and appropriate use of corticosteroids together with ventilator support should be considered for the severe patients to prevent ARDS based on the pathological findings of pulmonary edema and hyaline membrane formation [95].
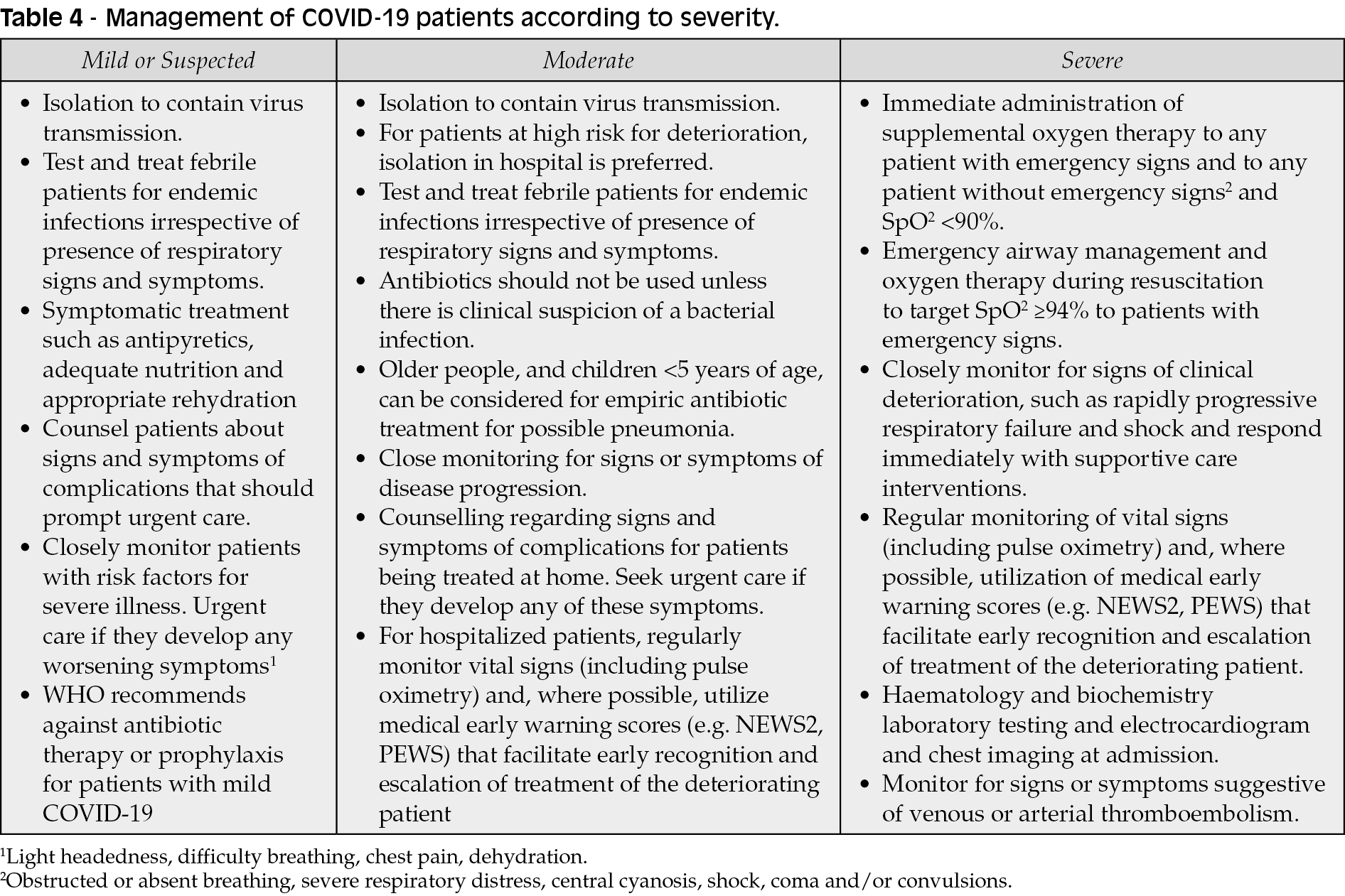
Results from the RECOVERY Trial showed that dexamethasone administered regularly for up to 10 days resulted in 28-day mortality reduction in certain groups of hospitalized COVID-19 patient [96]. Hence, dexamethasone, 6mg oral or intravenous daily, is now recommended by NIH and IDSA for patients with severely ill COVID-19 (requiring oxygen therapy) including those on mechanical ventilation [88, 89]. The reduced 28-day mortality was among patients receiving either invasive mechanical ventilation or oxygen alone. However, the findings of the RECOVERY trial data do not recommend dexamethasone for hospitalized COVID-19 patients who do not require respiratory support [97]. The management of COVID-19 according to its severity is described in Table 4.
VACCINE AND PREVENTION
The genetic sequence of SARS-CoV-2 was released on January 11th, 2020, and since then many pharmaceutical companies and academic institutions from various countries have emerged in collaborative efforts to develop the COVID-19 vaccine. Fortunately, some candidates have successfully entered clinical trial evaluation and proceeded to phase 3 onwards [97].
Phase 2/3 trial candidates undergoing clinical evaluation are depicted in Figure 5.

Figure 5 - Vaccine trial candidates undergoing clinical evaluation for SARS-CoV-2.
Fortunately, owing to the strenuous efforts of researchers, eight vaccines have been approved for Emergency Use Authorization (EUA). These belong to four different groups based on their mode of action, which includes mRNA-based vaccine, inactivated vaccine, non-replicating viral vector vaccine and peptide vaccine. Two the mRNA-based vaccines developed by Pfizer/BioNTech and Moderna have gained popularity owing to their approval in multiple countries. In the trial funded by Pfizer/BioNTech, Fosun Pharma the efficacy of this mRNA based vaccine BNT162b2 was assessed. People over 16 years of age or older in a 1:1 ratio were given two doses, 21 days apart, of either placebo or the BNT162b2 vaccine candidate (30 μg per dose). This aforementioned mRNA vaccine encodes a prefusion stabilized, membrane-anchored SARS-CoV-2 full-length spike protein. The vaccine (BNT162b2) was 95% effective in preventing COVID-19. Moreover, similar vaccine efficacy (generally 90 to 100%) was observed across subgroups defined by age, sex, race, ethnicity, baseline body-mass index, and the presence of coexisting conditions. The safety profile of BNT162b2 was characterized by short-term, mild-to-moderate pain at the injection site, fatigue, and headache. Safety over a median of 2 months was similar to that of other viral vaccines [98]. It is imperative to focus on the potential hurdles regarding perception of this vaccine in the mass population and distribution of vaccine especially in low- and middle-income countries. However, a thorough strategic planning will need to be devised to ensure optimum coverage with these vaccines to ease the crippling healthcare system.
The list of COVID-19 vaccines available for usage after undergoing emergent use authorization are shown in Table 5.
The Center for Disease Control and Prevention (CDC) and the WHO has initiated a set of guidelines for the general public as well as health professionals. These guidelines are reported in Figure 6.


Figure 6 - Guidelines to prevent the spread of COVID-19.
CONCLUSION
In conclusion, the COVID-19 pandemic has resulted in millions of infections globally and has stressed healthcare and economic systems to the extreme. Rapid diagnostic testing and effective anti-viral therapy are essential to reduce mortality associated with COVID-19. However, due to its pandemic nature, the prevention of this disease eventually rests on the mass implementation of the vaccine developed.
Conflict of interest
None
Funding
None
REFERENCES
[1] Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 2020; 55 (3), 105924.
[2] World Health Organization. COVID-19 Situation report - 51. 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10. Accessed: July 11, 2020.
[3] Bogoch II, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Pneumonia of unknown aetiology in Wuhan, China: potential for international spread via commercial air travel. J Travel Med. 2020; 27 (2), taaa008.
[4] Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020; 109, 102433.
[5] World Health Organization. COVID-19 Weekly epidemiological update - January 17, 2021. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/weekly_epidemiological_update_23.pdf?sfvrsn=6ac0778_5&download=true. Accessed: January 19, 2021.
[6] Meo SA, Alhowikan AM, Al-Khlaiwi T, et al. Novel coronavirus 2019-nCoV: prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur Rev Med Pharmacol Sci. 2020; 24 (4), 2012-9.
[7] World Health Organization. Pneumonia of unknown cause - China. Available from: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/. Accessed: June 15, 2020.
[8] Khan M, Adil SF, Alkhathlan HZ, Tahir MN, Saif S, Khan M, Khan ST. COVID-19: A global challenge with old history, epidemiology and progress so far. Molecules. 2020; 26 (1), 39.
[9] World Health Organization. COVID-19 Weekly epidemiological update - August 30, 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200831-weekly-epi-update-3.pdf?sfvrsn=d7032a2a_4&download=true. Accessed: January 19, 2021.
[10] World Health Organization. COVID-19 Weekly epidemiological update - September 28. 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200928-weekly-epi-update.pdf?sfvrsn=9e354665_6&download=true. Accessed: January 19, 2021.
[11] World Health Organization. COVID-19 Weekly epidemiological update - January 5. 2021. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20210105_weekly_epi_update_21.pdf?sfvrsn=15359201_15&download=true. Accessed: January 19, 2021
[12] World Health Organization. COVID-19 Weekly epidemiological update - January 19. 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/weekly_epidemiological_update_23.pdf?sfvrsn=6ac0778_5&download=true. Accessed: January 19, 2021.
[13] Fehr AR, Perlman S. Coronaviruses: an overview of their replication and pathogenesis. Methods Mol Biol. 2015; 1282, 1-23.
[14] Li F. Structure, Function, and Evolution of Coronavirus Spike Proteins. Annu Rev Virol. 2016; 3 (1), 237-61.
[15] Tyrrell DAJ, Myint SH. Coronaviruses. In: Baron S, editor. Medical Microbiology. 4th edition. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 60. Available from: https://www.ncbi.nlm.nih.gov/books/NBK7782/
[16] Van Hemert MJ, van den Worm SH, Knoops K, Mommaas AM, Gorbalenya AE, Snijder EJ. SARS-coronavirus replication/transcription complexes are membrane-protected and need a host factor for activity in vitro. PLoS Pathog. 2008; 4 (5): e1000054.
[17] Neuman BW, Adair BD, Yoshioka C, et al. Supramolecular architecture of severe acute respiratory syndrome coronavirus revealed by electron cryomicroscopy. J Virol. 2006; 80 (16), 7918-28.
[18] Beniac DR, Andonov A, Grudeski E, Booth TF. Architecture of the SARS coronavirus prefusion spike. Nat Struct Mol Biol. 2006; 13 (8), 751-2.
[19] Nieto-Torres JL, DeDiego ML, Verdiá-Báguena C, et al. Severe acute respiratory syndrome coronavirus envelope protein ion channel activity promotes virus fitness and pathogenesis. PLoS Pathog. 2014; 10 (5): e1004077.
[20] Hurst KR, Koetzner CA, Masters PS. Characterization of a critical interaction between the coronavirus nucleocapsid protein and nonstructural protein 3 of the viral replicase-transcriptase complex. J Virol. 2013; 87 (16), 9159-72.
[21] Cui L, Wang H, Ji Y, et al. The nucleocapsid protein of coronaviruses acts as a viral suppressor of RNA silencing in mammalian cells. J Virol. 2015; 89 (17), 9029-43.
[22] Klausegger A, Strobl B, Regl G, Kaser A, Luytjes W, Vlasak R. Identification of a coronavirus hemagglutinin-esterase with a substrate specificity different from those of influenza C virus and bovine coronavirus. J Virol. 1999; 73 (5), 3737-43.
[23] Kubo H, Yamada YK, Taguchi F. Localization of neutralizing epitopes and the receptor-binding site within the amino-terminal 330 amino acids of the murine coronavirus spike protein. J Virol. 1994; 68 (9), 5403-10.
[24] Li W, Moore MJ, Vasilieva N, et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature. 2003; 426 (6965), 450-4.
[25] Raj VS, Mou H, Smits SL, et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature. 2013; 495 (7440), 251-4.
[26] Belouzard S, Chu VC, Whittaker GR. Activation of the SARS coronavirus spike protein via sequential proteolytic cleavage at two distinct sites. Proc Natl Acad Sci USA. 2009; 106 (14), 5871-6.
[27] Samudrala PK, Kumar P, Choudhary K, et al. Virology, pathogenesis, diagnosis and in-line treatment of COVID-19. Eur J Pharmacol. 2020; 883, 173375.
[28] Krijnse-Locker J, Ericsson M, Rottier PJ, Griffiths G. Characterization of the budding compartment of mouse hepatitis virus: evidence that transport from the RER to the Golgi complex requires only one vesicular transport step. J Cell Biol. 1994; 124 (1-2), 55-70.
[29] Zhang H, Penninger JM, Li Y, Zhong N, Slutsky AS. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intens Care Med. 2020; 46 (4), 586-90.
[30] Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020; 395 (10235), 1517-20.
[31] Lin L, Lu L, Cao W, Li T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection-a review of immune changes in patients with viral pneumonia. Emerg Microbes Infect. 2020; 9 (1), 727-32.
[32] China National Health Commision Diagnosis and treatment of novel coronavirus pneumonia in China (trial version 7). Available from: https://www.who.int/docs/default-source/wpro---documents/countries/china/covid-19-briefing-nhc/1-clinical-protocols-for-the-diagnosis-and-treatment-of-covid-19-v7.pdf?sfvrsn=c6cbfba4_2. Accessed: July 10, 2020.
[33] Yao XH, Li TY, He ZC, et al. A pathological report of three COVID-19 cases by minimally invasive autopsies. Zhonghua Bing Li Xue Za Zhi. 2020; 49 (5), 411-7.
[34] Wichmann D, Sperhake JP, Lütgehetmann M, et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann Intern Med. 2020; 173 (4), 268-77.
[35] Ackermann M, Verleden SE, Kuehnel M, et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N Engl J Med. 2020; 383 (2), 120-8.
[36] Luers JC, Rokohl AC, Loreck N, et al. Olfactory and Gustatory Dysfunction in Coronavirus Disease 19 (COVID-19). Clin Infect Dis. 2020; 71 (16), 2262-4.
[37] Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ & Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19). JAMA. 2020; 324 (8), 782-93.
[38] Li X, Zai J, Zhao Q, et al. Evolutionary history, potential intermediate animal host, and cross-species analyses of SARS-CoV-2. J Med Virol. 2020; 92 (6), 602-11.
[39] Doremalen NV, Morris DH, Holbrook MG, et al. Aerosol and surface stability of HCoV-19 (SARS-CoV-2) compared to SARS-CoV-1. N Engl J Med. 2020; 382 (16), 1564-7.
[40] Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020; 324 (8), 782-93.
[41] Zeng L, Xia S, Yuan W, et al. Neonatal Early-Onset Infection With SARS-CoV-2 in 33 Neonates Born to Mothers With COVID-19 in Wuhan, China. JAMA Pediatr. 2020; 174 (7), 722-5.
[42] Jones DL, Baluja MQ, Graham DW, et al. Shedding of SARS-CoV-2 in feces and urine and its potential role in person-to-person transmission and the environment-based spread of COVID-19. Sci Total Environ. 2020; 749, 141364.
[43] Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020; 395 (10226), 809-15.
[44] Sunjaya AP, Jenkins C. Rationale for universal face masks in public against COVID-19. Respirology. 2020; 25 (7), 678-9.
[45] World Health Organization. SARS-CoV-2 Variants. 2020. Available from: https://www.who.int/csr/don/31-december-2020-sars-cov2-variants/en/. Accessed: January 7, 2021.
[46] Leung K, Shum MH, Leung GM, Lam TT, Wu JT. Early transmissibility assessment of the N501Y mutant strains of SARS-CoV-2 in the United Kingdom, October to November 2020. Euro Surveill. 2021; 26 (1), 2002106.
[47] He, X, Lau, EHY, Wu, P. et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020; 26 (5), 672-5.
[48] Ye ZW, Yuan S, Yuen KS, Fung SY, Chan CP, Jin DY. Zoonotic origins of human coronaviruses. Int J Biol Sci. 2020; 16 (10), 1686-97.
[49] Zhang JJ, Dong X, Cao YY, et al. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy. 2020; 75 (7), 1730-41.
[50] Lighter J, Phillips M, Hochman S, et al. Obesity in patients younger than 60 years is a risk factor for Covid-19 hospital admission. Clin Infect Dis. 2020; 71 (15), 896-7.
[51] Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020; 109 (6), 1088-95.
[52] Giacomelli A, Pezzati L, Conti F, et al. Self-reported Olfactory and Taste Disorders in Patients With Severe Acute Respiratory Coronavirus 2 Infection: A Cross-sectional Study. Clin Infect Dis. 2020; 71 (15), 889-90.
[53] Recalcati S. Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol. 2020; 34 (5), e212-3.
[54] Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020; 323 (11), 1061-9.
[55] Zheng YY, Ma YT, Zhang JY, Xie X. COVID-19 and the cardiovascular system. Nat Rev Cardiol. 2020; 17 (5), 259-60.
[56] Long B, Brady WJ, Koyfman A, Gottlieb M. Cardiovascular complications in COVID-19. Am J Emerg Med. 2020; 38 (7), 1504-7.
[57] Mao L, Jin H, Wang M, et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020; 77 (6), 683-90.
[58] Zhang C, Shi L, Wang FS. Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol. 2020; 5 (5), 428-30.
[59] Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020; 191,145-7.
[60] Mahase E. Covid-19: concerns grow over inflammatory syndrome emerging in children. BMJ. 2020; 369: m1710.
[61] Verdoni L, Mazza A, Gervasoni A, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. 2020; 395 (10239), 1771-8.
[62] Aggarwal K, Agarwal A, Jaiswal N, et al. Ocular surface manifestations of coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. PLoS One. 2020; 15 (11), e0241661.
[63] Riley S, Fraser C, Donnelly CA, et al. Transmission dynamics of the etiological agent of SARS in Hong Kong: impact of public health interventions. Science. 2003; 300 (5627), 1961-6.
[64] Pan Y, Zhang D, Yang P, et al. Viral load of SARS-CoV-2 in clinical samples. Lancet Infect Dis. 2020; 20 (4), 411-2.
[65] To KK, Tsang OT, Yip CC, et al. Consistent detection of 2019 novel coronavirus in saliva. Clin Infect Dis. 2020; 71 (15), 841-3.
[66] Kim YG, Yun SG, Kim MY, et al. Comparison between saliva and nasopharyngeal swab specimens for detection of respiratory viruses by multiplex reverse transcription-PCR. J Clin Microbiol. 2016; 55 (1), 226-33.
[67] Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020; 25 (3): 2000045.
[68] Chan JF, Yip CC, To KK, et al. Improved molecular diagnosis of COVID-19 by the novel, highly sensitive and specific COVID-19-RdRp/Hel real-time reverse transcription-polymerase chain reaction assay validated in vitro and with clinical specimens. J Clin Microbiol. 2020; 58 (5), e00310-20.
[69] Yip CC, Ho CC, Chan JF, et al. Development of a Novel, Genome Subtraction-Derived, SARS-CoV-2- Specific COVID-19-nsp2 Real-Time RT-PCR Assay and Its Evaluation Using Clinical Specimens. Int J Mol Sci. 2020; 21 (7), 2574.
[70] Centers for Diseases Control and Prevention. CDC’s Influenza SARS-CoV-2 Multiplex Assay and Required Supplies. update - February 2, 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/lab/multiplex.html
[71] Food and Drug Administration, US. Coronavirus Disease 2019 (COVID-19) Emergency Use Authorizations for Medical Devices. Available from: https://www.fda.gov/medical-devices/emergency-situations-medical-devices/emergency-use-authorizations-medical-devices.
[72] Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395 (10223), 497-506.
[73] Che XY, Hao W, Wang Y, et al. Nucleocapsid protein as early diagnostic marker for SARS. Emerg Infect Dis. 2004; 10 (11), 1947-9.
[74] Blanchard EG, Miao C, Haupt TE, Anderson LJ, Haynes LM. Development of a recombinant truncated nucleocapsid protein based immunoassay for detection of antibodies against human coronavirus OC43. J Virol Methods. 2011; 177 (1), 100-6.
[75] Timani KA, Ye L, Ye L, Zhu Y, Wu Z, Gong Z. Cloning, sequencing, expression, and purification of SARS-associated coronavirus nucleocapsid protein for serodiagnosis of SARS. J Clin Virol. 2004; 30 (4), 309-12.
[76] Guo L, Ren L, Yang S, et al. Profiling Early Humoral Response to Diagnose Novel Coronavirus Disease (COVID-19). Clin Infect Dis. 2020; 71 (15), 778-85.
[77] Jiang F, Deng L, Zhang L, Cai Y, Cheung CW, Xia Z. Review of the Clinical Characteristics of Coronavirus Disease 2019 (COVID-19). J Gen Intern Med. 2020; 35 (5), 1545-9.
[78] Long C, Xu H, Shen Q, et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. 2020; 126, 108961.
[79] Pan F, Ye T, Sun P, et al. Time course of lung changes on chest CT during recovery from coronavirus disease 2019 (COVID-19). Radiology 2020; 295 (3), 715-21.
[80] M Corman V, Landt O, Kaiser M, et al. Detection of 2019 Novel Coronavirus (2019-nCoV) by Real-Time RTPCR. Euro Surveill 2020; 26 (5), 210204e.
[81]Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Features, Evaluation and Treatment Coronavirus (COVID-19) StatPearls. 2020; Available from: https://www.ncbi.nlm.nih.gov/books/NBK554776/
[82] WHO Solidarity Trial Consortium, Pan H, Peto R, et al. Repurposed Antiviral Drugs for Covid-19 - Interim WHO Solidarity Trial Results. N Engl J Med. 2020; doi: 10.1056/NEJMoa2023184.
[83] Sheahan TP, Sims AC, Leist SR, et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat Commun. 2020; 11 (1), 222.
[84] Clinical Trials. Adaptive COVID-19 Treatment Trial (ACTT). Available from: https://clinicaltrials.gov/ct2/show/NCT04280705Accessed: July 24, 2020.
[85] World Health Organization. WHO recommends against the use of remdesivir in COVID-19 patients. Available from: https://www.who.int/news-room/feature-stories/detail/who-recommends-against-the-use-of-remdesivir-in-covid-19-patients
[86] Kalil AC, Patterson TF, Mehta AK, et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Engl J Med. 2020; doi: 10.1056/NEJMoa2031994.
[87] Food and Drug Administration, US. Coronavirus (COVID-19) Update: FDA Authorizes Drug Combination for Treatment of COVID-19. Available from: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-drug-combination-treatment-covid-1987
[88] NIH. COVID-19 Treatment Guidelines. Available from: https://www.covid19treatmentguidelines.nih.gov/ Accessed: August 26, 2020.
[89] Bhimraj A, Morgan RL, Shumaker AH, et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin Infect Dis. 2020; doi: 10.1093/cid/ciaa478.
[90] Salama C, Han J, Yau L, et al. Tocilizumab in Patients Hospitalized with Covid-19 Pneumonia. N Engl J Med. 2021; 384 (1), 20-30.
[91] Some drugs for COVID-19. Med Lett Drugs Ther. 2020; 62 (1595), 49-50. Available from: https://secure.medicalletter.org/w1919a
[92] Tian X, Li C, Huang A, et al. Potent binding of 2019 novel coronavirus spike protein by a SARS coronavirus-specific human monoclonal antibody. Emerg Microbes Infect. 2020; 9 (1), 382-5.
[93] Agarwal A, Mukherjee A, Kumar G, et al. Convalescent plasma in the management of moderate covid-19 in adults in India: open label phase II multicentre randomised controlled trial (PLACID Trial) BMJ 2020; 371, m4232.
[94] Joyner M, Wright RS, Fairweather D, et al. Early Safety Indicators of COVID-19 Convalescent Plasma in 5,000 Patients. medRxiv. 2020; doi: 10.1101/2020.05.12.20099879.
[95] Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020; 8 (4), 420-2.
[96] RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid-19 - Preliminary Report. N Engl J Med. 2020; doi: 10.1056/NEJMoa2021436.
[97] Zhang N, Li C, Hu Y, et al. Current development of COVID-19 diagnostics, vaccines and therapeutics. Microbes Infect. 2020; 22 (6-7), 231-5.
[98] Polack FP, Thomas SJ, Kitchin N, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med. 2020; 383 (27), 2603-15.