Le Infezioni in Medicina, n. 1, 10-19, 2021
REVIEWS
Airborne transmission of SARS-CoV-2 is the dominant route of transmission: droplets and aerosols
Ali A. Rabaan1, Shamsah H. Al-Ahmed2, Maysaa K. Al-Malkey3, Roua A. Alsubki4, Sayeh Ezzikouri5, Fadel Hassan Al-Hababi6, Ranjit Sah7, Abbas Al Mutair8,9, Saad Alhumaid10, Jaffar A. Al-Tawfiq11,12,13, Awad Al-Omari14,15, Ayman M. Al-Qaaneh16,17, Manaf Al-Qahtani18,19, Raghavendra Tirupathi20,21, Mohammad A. Al Hamad22, Nadira A Al-baghli23, Tarek Sulaiman24, Arwa Alsubait25, Rachana Mehta26, Elfadil Abass27, Maha Alawi28,29, Fatimah Alshahrani30, Dhan Bahadur Shrestha31, Mohmed Isaqali Karobari32, Samuel Pecho-Silva33,34, Kovy Arteaga-Livias35,36,37, D. Katterine Bonilla Aldana38,39, Alfonso J. Rodriguez-Morales34,37,40,41
1Molecular Diagnostic Laboratory, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia;
2Specialty Paediatric Medicine, Qatif Central Hospital, Qatif, Saudi Arabia;
3Tropical Biological Research Unit, College of Science, University of Baghdad, Baghdad, Iraq;
4Department of Clinical Laboratory Sciences, Chair of Medical and Molecular Genetics Research, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia;
5Virology Unit, Viral Hepatitis Laboratory, Institut Pasteur du Maroc, Casablanca, Morocco;
6Virology Department, Riyadh Regional Laboratory, Riyadh, Saudi Arabia;
7Department of Microbiology, Tribhuvan University Teaching Hospital, Institute of Medicine, Kathmandu, Nepal;
8School of Nursing, Wollongong University, Australia;
9Research Center, Almoosa Specialist Hospital, Alahsa, Saudi Arabia;
10Administration of Pharmaceutical Care, Ministry of Health, Alahsa, Saudi Arabia;
11Specialty Internal Medicine, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia;
12Department of Medicine, Indiana University School of Medicine, Indianapolis, IN, USA;
13Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA;
14School of Medicine, Critical Care and Infection Control Department, Al-Faisal University, Riyadh, Saudi Arabia;
15Dr. Sulaiman Al-Habib Medical Group, Riyadh, Saudi Arabia;
16Department of Genetic Research, Institute for Research and Medical Consultations (IRMC), Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia;
17Clinical Pharmacy Services Division, Pharmacy Services Department, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia;
18Department of Medicine, Royal Medical Services, Bahrain Defence Force Hospital, Manamah, Bahrain;
19Department of Medicine, Royal College of Surgeons in Ireland-Bahrain Medical University, Manamah, Bahrain;
20Penn State University School of Medicine, Hershey, PA, USA;
21Wellspan Chambersburg and Waynesboro Hospitals, Chambersburg, PA, USA;
22Department of Pathology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia;
23Directorate of Health Affairs, Ministry of Health, Dammam, Saudi Arabia;
24King Fahad Medical City, Riyadh, Saudi Arabia;
25King Abdullah International Medical Research Center, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs;
26National Public Health Laboratory, Kathmandu, Nepal;
27Department of Clinical Laboratory Science, College of Applied Medical Sciences, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia;
28Department of Medical Microbiology and Parasitology, King Abdulaziz University, Jeddah, Saudi Arabia;
29Infection Control and Environmental Health Unit, King Abdulaziz University Hospital, Faculty of Medicine, Jeddah, Saudi Arabia;
30Division Of Infectious Diseases, Department of Internal Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia;
31Department of Emergency Medicine, General Practice, Mangalbare Hospital, Urlabari-03, Morang, Nepal;
32Conservative Dentistry Unit, School of Dental Sciences, University Sains Malaysia, Health Campus, Kelantan, Malaysia;
33Pneumology Service, Hospital Nacional Edgardo Rebagliati Martins, Lima, Peru;
34Master in Clinical Epidemiology and Biostatistics, Universidad Cientifica del Sur, Lima, Peru;
35Faculty of Medicine. Universidad Nacional Hermilio Valdizan. Huanuco, Peru;
36Hospital II Huánuco, EsSalud. Huanuco, Peru;
37Facultad de Ciencias de la Salud, Universidad Científica del Sur, Lima, Peru;
38Semillero de Investigacion en Zoonosis (SIZOO), Grupo de Investigacion BIOECOS, Fundacion Universitaria Autonoma de las Americas, Sede Pereira, Pereira, Risaralda, Colombia;
39Public Health and Infection Research Group, Faculty of Health Sciences, Universidad Tecnologica de Pereira, Pereira, Colombia;
40Public Health and infection Research Group, Faculty of Health Sciences, Universidad Tecnologica de Pereira, Pereira, Risaralda, Colombia;
41Grupo de Investigación Biomedicina, Faculty of Medicine, Fundacion Universitaria Autonoma de las Americas, Pereira, Risaralda, Colombia
Corresponding authors
Ali A. Rabaan
E-mail: arabaan@gmail.com; ali.rabaan@jhah.com
Alfonso J Rodriguez-Morales
E-mail: arodriguezm@utp.edu.co
SummaRY
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a pandemic worldwide. On a daily basis the number of deaths associated with COVID-19 is rapidly increasing. The main transmission route of SARS-CoV-2 is through the air (airborne transmission). This review details the airborne transmission of SARS-CoV-2, the aerodynamics, and different modes of transmission (e.g. droplets, droplet nuclei, and aerosol particles). SARS-CoV-2 can be transmitted by an infected person during activities such as expiration, coughing, sneezing, and talking. During such activities and some medical procedures, aerosols and droplets contaminated with SARS-CoV-2 particles are formed. Depending on their sizes and the environmental conditions, such particles stay viable in the air for varying time periods and can cause infection in a susceptible host. Very few studies have been conducted to establish the mechanism or the aerodynamics of virus-loaded particles and droplets in causing infection. In this review we discuss the various forms in which SARS-CoV-2 virus particles can be transmitted in air and cause infections.
Keywords: SARS-CoV-2, COVID-19, airborne transmission, droplets, aerosol.
INTRODUCTION
The coronavirus disease-2019 (COVID-19) caused by the new coronavirus known as SARS-CoV-2 was recently reported in China, in late December 2019 and quickly spread worldwide [1-3]. As of February 13, 2021, there were 107,838,255 confirmed cases of COVID-19 and total number of deaths due to COVID-19 was 2,373,398 worldwide [3].
COVID-19 patients present typical symptoms of severe acute respiratory disease [4-6].
COVID-19 follows several modes of transmission from infected person to others through droplets, aerosols, and fomites [7]. Several pathways are followed by infectious agents to spread from the natural reservoir to the susceptible hosts [8]. However, the respiratory viruses employ multiple modes of transmission; of them, droplet and aerosol transmissions are of significant importance [9, 10]. When an infected person talks, breaths, sneezes or coughs, the viral particles are released into the air encapsulated in globs of mucous and saliva. The spread of these virus particles through these globs depend on the size of the globs. Bigger globs fall faster in the nearby areas and form droplets, whereas, the smaller globs evaporate and form aerosols [11]. These aerosols last for more time in the air and travel farther than the droplets. It is believed that aerosols pose more risk of COVID-19 spread to susceptible persons at a distance as compared to droplets. However, it has been seen that viral disease spread through aerosol is not as rigorous as it is speculated because of the dilution and inactivation of the viruses during longer periods of travel in the air [10].
There is no agreement on the minimum required viral load to cause COVID-19 in a healthy individual. In contrast, many researchers consider that a few hundred SARS-CoV-2 are enough to cause COVID-19 in the susceptible hosts [12].
There are varying reports on the average particle size of aerosols and droplets [10]. According to the World Health Organization (WHO) and Center for Disease Control and Prevention (CDC), particles with diameter more than 5 μm are considered as droplets and, those with diameters less than 5 μm are considered as aerosols [13, 14]. Others identify particles as aerosols based on their capability to stay in the air for a long-lasting period, and their ability to reach the alveolar region of the lungs [15, 16]. Small aerosols are inhaled deep into the lung and cause infections in the lower respiratory tract whereas large droplets are limited in the upper respiratory tract [17].
In case of COVID-19 more evidence is in support of the hypothesis that droplets predominantly transmit the disease than aerosols. Therefore, research has been focussed more on the role and mechanism of droplet transmission. However, recent evidences support the hypothesis that aerosols also play an important role in the transmission of SARS-CoV-2 [7, 9]. It has been speculated that the environmental settings play an important role in the SARS-CoV-2 transmission and may be beneficial or adverse in terms of the virus spread [8, 16].
Since the COVID-19 has been declared as a pandemic by the WHO, plethora of research is being done on controlling the disease spread in closed environments. Very less attention has been paid to the measures to study the droplet or aerosol transmission aerodynamics and mechanisms in viral infections, especially SARS-CoV-2. In the present review we have discussed the various forms in which the SARS-CoV-2 particles can be transmitted in air and cause infections.
Reproduction number (R0)
Reproduction number (R0) indicates the transmissibility potential of a virus. R0 signifies the average number of naïve individuals that can be infected by an infectious person. Several studies have reported the R0 for SARS-CoV-2. In a comprehensive review published recently, it was reported that the R0 for SARS-CoV-2 ranged from 1.4 to 6.49, with a mean of 3.28, a median of 2.79 and interquartile range (IQR) of 1.16 [18]. In another article it was highlighted that the R0 for SARS-CoV-2 is 2·5 (range 1·8–3·6) which was higher than the R0 reported for SARS-CoV and the 1918 influenza pandemic (2∙0–3∙0), MERS-CoV (0.9), and the 2009 influenza pandemic (1.5) [19].
Generation and transmission of droplets and aerosols
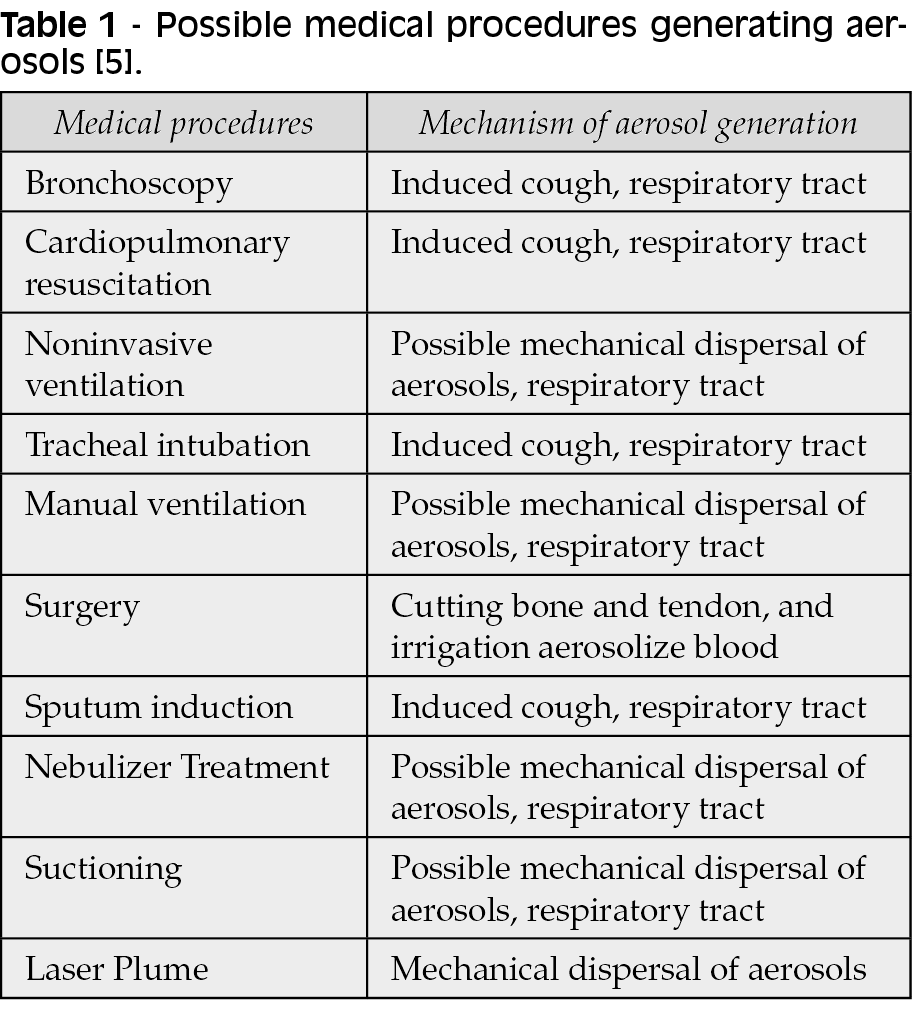
The primary source of aerosols and droplets is the infected person. When an infected person coughs, sneezes or talks, aerosols and droplets containing the virus particles are generated. Besides the infected person there are other sources of aerosol and droplets such as some medical and surgical procedures, toilet flushes, and running tap water [5, 8].
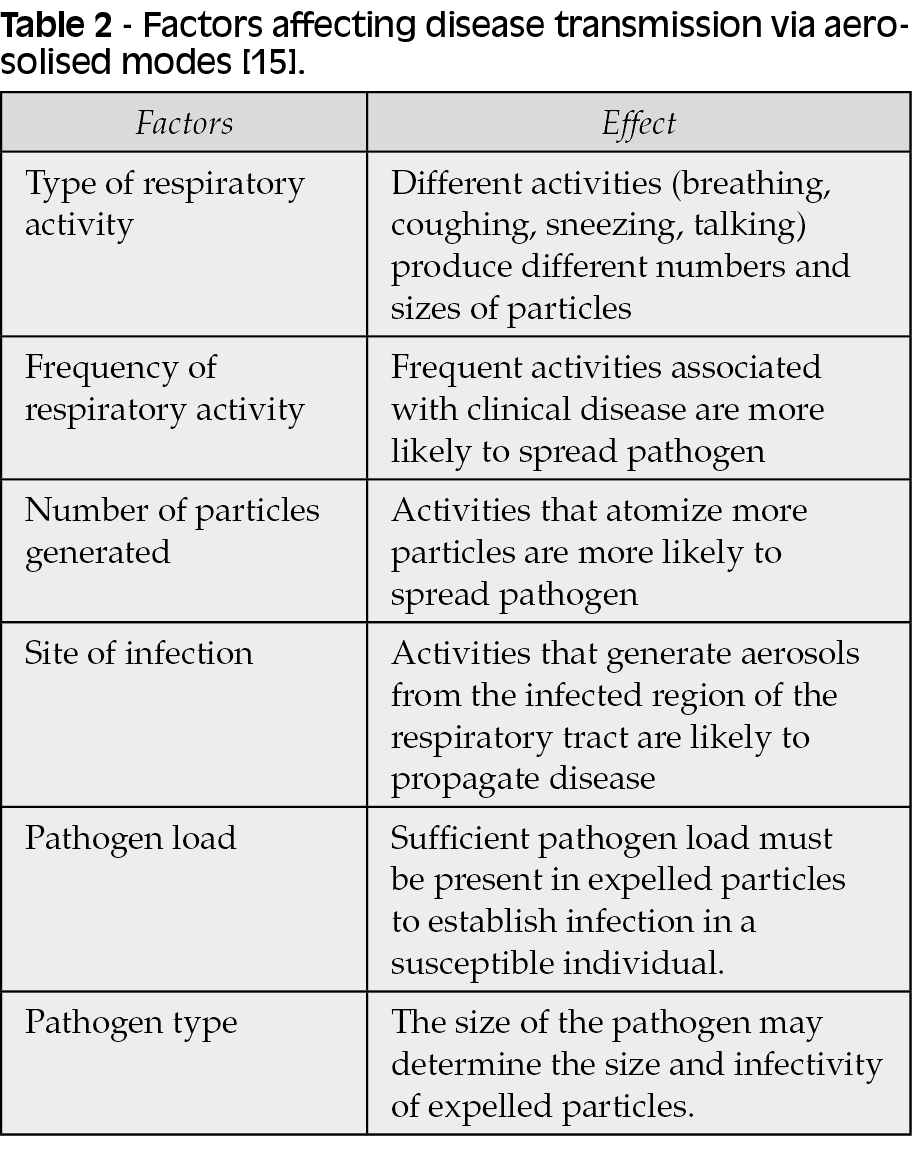
The influenza virus can be transmitted by three modes: aerosol, droplet, and through nasal mucosa contaminated hands [16]. According to another classification given by Judson and Munster (2019), “airborne transmission” is the transmission of the virus by small aerosol droplets and aerosol nuclei and “droplet transmission” is the transmission of the virus by large aerosol droplets. Another important modes of transmission are direct contact and through fomite generated by medical procedures that produce aerosols [5] (Table 1). Several factors such as the presence of pathogens, type of pathogen, clinical manifestation of the disease, and site of infection influence the potential of spread of infection through aerosolised particles [15] (Table 2). Droplet transmission can occur when an infected person coughs, talks, or sneezes by the direct spray on to the mucous membranes or conjunctiva of the susceptible hosts. Contact transmission occurs by either direct physical contact of the infected person with susceptible host or indirectly by the contact with infectious secretions from the infected persons [20-22, 16]. COVID-19 is highly contagious because of human to human transmission. Self-inoculation from contaminated fomites is the major factor making SARS-CoV-2 contagious. The most important causes of self-inoculation are poor hand hygiene and negligence in following the basic infection control guidelines [23]. However, since the COVID-19 outbreak is novel, there is very less confirmed evidence for its potential routes of transmission and therefore it is believed that it spreads like other human coronaviruses [24].
Most studies advocate that SARS-CoV-2 is spread through contact transmission and respiratory droplets [24-26]. A few studies have also highlighted the presence of live SARS-CoV-2 virus in the faeces of COVID-19 patients [27]. Therefore another potential route of transmission is through the faeces of infected persons [27, 28].
A study on the influenza virus highlighted that trans-ocular transmission of the virus is an effective route of infection [29]. The conjunctiva of the eye is accessible to infectious droplets and fomites during contact with contaminated hands and infected individuals. Several respiratory viruses such as human adenovirus (species D) and avian influenza virus (H7) frequently cause conjunctivitis or keratoconjunctivitis [30, 31]. The nasolacrimal duct connects the mucosa of the ocular surface and the upper respiratory tract and therefore the ophthalmic surface can act as an entry point for the human coronaviruses to cause respiratory infections on exposure to contaminated droplets and aerosols. However, SARS-CoV and MERS-CoV infections have not been reported in the eye and conjunctivitis has been reported in only a few cases with COVID-19 (only five cases). This suggests that eye is not a preferred route of CoV infection. However, the chances of COVID-19 infection through the ocular surfaces cannot be completely ruled out [30, 32-36]. Recent studies have reported very low positive rates of RT-PCR tests with the tear and conjunctival scraping samples [30, 35-42].
According to the U.S. Centers for Disease Control and Prevention, ears are not believed to be an effective route of COVID-19 infection. It is not known if the respiratory mucosa lining the middle ear and mastoid air cell system is involved in COVID-19 [43, 44]. However, a recent study reported SARS-CoV-2 colonization of the middle ear and mastoid in 2 of 3 patients [45].
The SARS-CoV-2 stays alive in the air for many hours posing the risk of aerosol mediated transmission of COVID-19 [46]. Not only the infected person but also the hospital procedures such as endotracheal intubation, bronchoscopy, open suctioning, administration of nebulized treatment, manual ventilation before intubation, turning the patient to the prone position, disconnecting the patient from the ventilator, non-invasive positive-pressure ventilation, tracheostomy, and cardiopulmonary resuscitation also generate aerosols loaded with SARS-CoV-2 particles [23]. The WHO has issued a set of precautionary guidelines to be used while managing the COVID-19 patients in the hospitals to reduce the risk of aerosol mediated transmission of SARS-CoV-2 [47].
Despite the strict application of these guidelines, the healthcare workers are constantly at the risk of exposure to SARS-CoV-2 through respiratory droplets, aerosols, and direct handling of contagious samples of COVID-19 patients. In an attempt to investigate the sources of transmission of SARS-CoV-2 in healthcare settings, Ong et al. (2020) reported that there was no transmission through the Personal Protective Equipment (PPE) used by the hospital staff attending the COVID-19 patients. However, they observed that samples collected from the air outlet exhaust fans of the patient rooms showed the presence of SARS-CoV-2 indicating that airborne transmission is possible in the hospital settings [48]. Another study also supported this observation and highlighted that the samples collected from the exhaust air outlets of the COVID-19 patient room were positive for SARS-CoV-2 [48]. These observations support the fact that SARS-CoV-2 is transmitted via air or aerosol particles.
Factors modulating the efficiency of the droplets and aerosols in the viral transmission: Size, time of viability in air, and distance of transmission
The SARS-CoV-2 is believed to be transmitted through contaminated droplets [9]. The heavy droplets settle down on nearby surfaces as they are too heavy to travel in the air. Fomites get contaminated by these virus laiden?? droplets and when touched by a susceptible host cause infection (Figure 1). However, the droplets with smaller aerodynamic diameters travel longer distances in the form of aerosols referred as bioaerosols and consequently result in airborne transmission of the disease [8]. When these bioaerosols loaded with SARS-CoV-2 particles are inhaled, result in infection. The larger aerosol particles sometimes become smaller by the process of evaporation and now these smaller particles are called droplet nuclei.
Figure 1 - Transmission of SARS-CoV-2.
The mechanisms of formation and aerodynamics of the droplets and aerosols are not investigated properly especially in the indoor environments. It dates back to 1945 when Duguid for the first time reported the dynamics of aerosol and droplet formation by the persons with chest infection. It was reported that about 95% of the particles were below the size of 100 μm. Most of these particles were 4 and 8 μm in diameter. The respiratory activities (inhalation and exhalation) released a few hundreds of droplets and some of them were aerosol particles while activities of talking, coughing, and sneezing generated more aerosols than droplets [49]. Another study reported contrasting findings and highlighted that 80-90% of particles released during expiration were aerosols with diameters smaller than 1 μm and that coughing generates the highest amount of aerosol particles and nasal breathing generates the lowest amounts of aerosol particles [50].
The behaviour of the airborne aerosols depend on several factors such as evaporation, their interaction with other particles, mode of transport, and deposition on surfaces [8]. The mechanism of diffusion is an important mode of transmission of viruses with sizes at sub-micrometer range along with aerosols [51]. The fate of droplets larger than 1 μm is decided by gravity [52]. Droplets smaller than 100 μm gets evaporated before reaching the surfaces and stay in the air for longer periods. If the droplets contain bioaerosols loaded with infectious virus, the bioaerosols stay in the air even after the liquid content of the droplets is evaporated [8]. The time of survival of the virus in the bioaerosols depends on the type of bioaerosol.
Droplets with size range of 0.5-20.0 μm suspended in the air are more likely to cause to respiratory tract infections [53]. However, due to the process of evaporation, droplets do not stay in the air for long and gets converted into bioaerosols that stay in the air for longer time. Reports have confirmed the airborne transmission of SARS-CoV in closed environments [54]. In another study it was reported that an infected passenger transmitted SARS-CoV to a co-passenger sitting seven rows ahead. This indicates that SARS-CoV can travel horizontally for more than 1 metre [55].
Another study reported that aerosol generated due to sewage system in a building in Hongkong infected more than 1000 residents of the building [56]. Therefore, the aerosol particles carrying the virus are the major players in the SARS-CoV-2 transmission and utmost care and precaution should be considered to prevent the transmission through these aerosol particles.
Studies have shown that the SARS-CoV-2 virus remains infectious in aerosols for 3 hours while in the form of droplets the SARS-CoV-2 remains on various surfaces for different time periods (plastic and stainless steel-72 hours, copper-4 hours, cardboard-24 hours, and glass-84 hours) [46]. The SARS-CoV and SARS-CoV-2 behave more or less in the same way in the form of aerosol particles with an overall survival in the aerosols for 3 hours. However, in the form of droplets the SARS-CoV behaves quite differently than SARS-CoV-2 with different survival times on different surfaces (plastic and stainless steel-72 hours, copper-8 hours, cardboard-8 hours, and glass-96 hours [46]. The SARS-CoV-2 and SARS-CoV have similar median half lives (1.1-1.2 hours) in the aerosols indicating that both the viruses have similar characteristics of airborne transmission [46]. However, the higher transmission rates of SARS-CoV-2 may be due to high viral loads in the upper respiratory tract and the possibility of transmission of SARS-CoV-2 even from an asymptomatic patient [78].
Since the SARS-CoV-2 can be viable in the air for 3-hours, the aerosol particles loaded with the virus can cause infection even in stagnant environment [46].
According to the WHO, the actual airborne time for virus loaded droplets may be greater in circumstances with significant cross-flows such as in quarantine centres and hospitals, for example in conditions of opening of the doors frequently and shifting of equipments into and out of the rooms [58]. In contrast, the airborne durations for droplet nuclei and aerosols is shorter as compared to droplets as the droplet nuclei and aerosols are affected by downdraft, for example when these droplet nuclei or aerosols pass under a ceiling supply vent [40]. This means that the trajectory of the mucous released form an individual depends on the size of the droplets and the path of the airflow patterns. Conflicting reports exist to establish an accepted safe zone of exclusion. The safe zone of exclusion varies in different studies, from 2 metres [59], to 6 metres [60].
Studies on patients with respiratory infections proved that when an infected person sneezes or coughs a cloud of pathogen loaded droplets is formed; these droplets can travel up to 7-8 m away from the source [61, 62]. Recent studies on COVID-19 have given results in agreement with previous findings [63, 64]. According to Xie et al. (2007), pathogen loaded droplets, irrespective of their sizes can travel up to 7-8 m in sneezing events and for more than 2 m in the vents of coughing. However, the WHO and CDC have different recommendations for the maintenance of distance between healthcare workers and COVID-19 patients (WHO-1 m; CDC-2 m) [65, 66]. Whereas, majority of the studies on COVID-19 have been conducted in laboratory conditions and therefore the results are not convincing when applied in real life situations.
Environmental factors decide the transmissibility of the droplets and aerosols
The behaviour of the virus while in the aerosol particles largely depend on the environmental conditions such as temperature, humidity, sunlight (radiations), and ventilation. The SARS-CoV-2 virus particles being less than 100 nm in size and their viability and infectivity largely depend on the environmental conditions before reaching the susceptible host [67]. The tolerance of the virus to the environmental stress depends majorly upon the phenotype of the virus, aerosol composition, and the virus payload [68]. Since the environmental factors play an important role in the transmission of SARS-CoV-2 virus in different conditions, the environmental factors should be studied in more details in the context of COVID-19. A recent study has reported association of air pollutants such as PM2.5, PM10, NO2, and O3 with COVID-19 infection [69].
Face masks for protection against droplet and aerosol transmission
In addition to the effective vaccines, the best way to prevent the transmission of COVID-19 is wearing face masks. The face masks have been show to be effective in preventing the spread of SARS, MERS, SARS-CoV-2, other human coronaviruses, and influenza viruses from symptomatic individuals [70]. The face masks such as the surgical mask, N95 respirator, and elastomeric respirators are the widely used face masks worldwide. These masks have helped in preventing COVID-19 to different degrees [71, 72]. The N95 masks are shown to prevent aerosol and droplet transmission but the surgical masks fail to prevent aerosol transmission of SARS-CoV-2 [73-75].
However, some studies propose that the N95 mask are no better than the surgical masks and do not recommend the usage of N95 masks for the general public and non-high risk healthcare providers [70]. With exponential rise in the use and demand of masks worldwide, the CDC has recommended the use of handmade cloth masks for general public. In contrast, the use of masks to prevent the spread of COVID-19 is still not clear and there is no consensus on this topic. There are studies that have proven that the homemade cloth masks are not suitable to prevent virus transmission as compared to the surgical masks (3 fold better than the cloth masks) [75].
None of these masks can prevent the virus transmission completely. Therefore, social distancing along with the use of masks can be considered strictly to reduce the risks of SARS-CoV-2 airborne transmission.
CONCLUSION
To conclude, the SARS-CoV-2 can be transmitted by direct or indirect contact (through the acts of sneezing, coughing, through eye and nasal mucous membranes) and other possible routes can be blood, faecal-oral routes, urine, and breastfeeding [77]. Airborne transmission of SARS-CoV-2 is highly virulent and represents the dominant route of SARS-CoV-2 transmission [78]. In summary, the transmission of SARS-CoV-2 from an infected person is majorly through the air in the form of droplets and aerosol particles. These particles vary in their sizes and aerodynamics. The rate of airborne transmission of SARS-CoV-2 depends on several factors such as the source of the droplets and the aerosols, the viral load, the airflow status, environmental conditions, etc. Face masks have been promising in preventing the airborne transmission of SARS-CoV-2 to some extent. However, there is no confirmatory conclusion on the efficiency of the face masks in preventing the SARS-CoV-2 spread.
Conflicts of interest
All authors declare that there exist no commercial or financial relationships that could, in any way, lead to a potential conflict of interest.
Funding
This compilation is a review article written, analysed, and designed by its authors and required no funding to be stated.
REFERENCES
[1] Chen C, Zhao B. Makeshift hospitals for COVID-19 patients: where health-care workers and patients need sufficient ventilation for more protection. J Hosp Infect. 2020; 105 (1), 98-9.
[2] Gorbalenya A.E. Severe acute respiratory syndrome-related coronavirus–the species and its viruses, a statement of the coronavirus study group. BioRxiv. 2020; 02 (07), 1-15.
[3] WHO 2020; https://www.who.int/emergencies/diseases/novel-coronavirus-2019; accessed on 16.11.2020.
[4] Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395 (10223), 497-506.
[5] Judson SD, Munster VJ. Nosocomial transmission of emerging viruses via aerosol-generating medical procedures. Viruses. 2019; 11 (10), 940.
[6] Nicas M, Nazaroff WW, Hubbard A. Toward understanding the risk of secondary airborne infection: emission of respirable pathogens. J. Occup. Environ. Hyg. 2005; 2 (3), 143-54.
[7] Wang J, Du G. COVID-19 may transmit through aerosol. Ir J Med Sci. 2020; 189 (4), 1143-4.
[8] Morawska L. Droplet fate in indoor environments, or can we prevent the spread of infection? Indoor Air. 2006; 16 (5), 335-47.
[9] Morawska L, Cao J. Airborne transmission of SARS-CoV-2: the world should face the reality. Environ. Int. 2020;139, 105730.
[10] Shiu EYC, Leung NHL, Cowling BJ. Controversy around airborne versus droplet transmission of respiratory viruses: implication for infection prevention. Curr Opin Infect Dis. 2019; 32 (4), 372-9.
[11] Grayson SA, Griffiths PS, Perez MK. et al. Detection of airborne respiratory syncytial virus in a pediatric acute care clinic. Pediatr. Pulmonol. 2017; 52 (5), 684-8.
[12] Beggs CB. Is there an airborne component to the transmission of COVID-19?: a quantitative analysis study. medRxiv. 2020; https://doi.org/10.1101/2020.05.22. 20109991.
[13] Siegel JD, Rhinehart E, Jackson M. et al. Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings. 2007. Centers for Disease Control and Prevention (CDC). https://www.cdc.gov/infectioncontrol/guidelines/isolation/index.html, Accessed date: 17 September, 2020.
[14] World Health Organization (WHO). Infection Prevention and Control of Epidemic and Pandemic Prone Acute Respiratory Infections in Healthcare - WHO Guidelines. 2014. https://www.who.int/csr/bioriskreduction/infection_control/publication/en/, Accessed date: 17 September, 2020.
[15] Gralton J, Tovey E, McLaws ML, et al. The role of particle size in aerosolised pathogen transmission: a review. J Infect. 2011; 62 (1),1-13.
[16] Tellier R. Aerosol transmission of influenza A virus: a review of new studies. J R Soc Interface. 2009; 6 (6), 783-90.
[17] Thomas RJ. 2013. Particle size and pathogenicity in the respiratory tract. Virulence. 2013; 4 (8), 847-58.
[18] Liu Y, Gayle AA, Wilder-Smith A, et al. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. 2020; 27 (2), taaa021.
[19] Petersen E, Koopmans M, Go U, et al. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis. 2020; 20 (9), 238-44.
[20] Boone SA, Gerba CP. Significance of fomites in the spread of respiratory and enteric viral disease. Appl Environ Microbiol. 2007; 73 (6), 1687-96.
[21] Brankston G, Gitterman L, Hirji Z, et al. Transmission of influenza A in human beings. Lancet Infect Dis. 2007; 7 (12), 760-1.
[22] Nicas M, Nazaroff WW, Hubbard A. Toward understanding the risk of secondary airborne infection: emission of respirable pathogens. J Occup Environ Hyg. 2005; 2 (3), 143-54.
[23] Kwok YLA, Gralton J, McLaws ML. Face touching: a frequent habit that has implications for hand hygiene. Am J Infect Control. 2015; 43 (2), 112-4.
[24] Centers for Disease Control and Prevention (CDC). Coronavirus Disease 2019 (COVID-19): How COVID-19 Spreads. https://www.cdc.gov/coronavirus/2019- ncov/prepare/transmission.html. 2020. Accessed date: 17 September 2020.
[25] World Health Organization (WHO). Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March 2020. https://apps.who.int/iris/handle/10665/331601 2020b. Accessed date: 17 September 2020.
[26] Chan JFW, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020; 395 (10223), 514-23.
[27] Wang W, Xu Y, Gao R, et al. Detection of SARSCoV-2 in different types of clinical specimen. JAMA. 2020; 323 (18),1843-4.
[28] Zhang J, Wang S, Xue Y. Fecal specimen diagnosis 2019 novel coronavirus–infected pneumonia. J Med Virol. 2020; 92 (6), 680-2.
[29] Bischoff WE, Reid T, Russell GB, et al. Transocular entry of seasonal influenza-attenuated virus aerosols and the efficacy of N95 respirators, surgical masks, and eye protection in humans. J Infect Dis. 2011; 204 (2), 193-9.
[30] Belser JA, Rota PA, Tumpey TM. Ocular tropism of respiratory viruses. Microbiol Mol Biol Rev. 2013; 77 (1), 144-56.
[31] Pedrosa PBS, Cardoso TAO. Viral infections in workers in hospital and research laboratory settings: a comparative review of infection modes and respective biosafety aspects. Int J Infect Dis. 2011; 15 (6), 366-76.
[32] Zhou Y, Zeng Y, Tong Y, et al. Ophthalmologic evidence against the interpersonal transmission of 2019 novel coronavirus through conjunctiva. medRxiv. 2020; 10 (1101).
[33] Zhang X, Chen X, Chen L, et al. The evidence of SARS-CoV-2 infection on ocular surface. Ocul Surf. 2020; 18 (3), 360-2.
[34] Vabret A, Mourez T, Dina J, et al. Human coronavirus NL63, France. Emerg Infect Dis. 2005;11 (8), 1225-9.
[35] Van der Hoek L, Pyrc K, Jebbink MF, et al. Identification of a new human coronavirus. Nat Med. 2004; 10 (4), 368-73.
[36] Xia J, Tong J, Liu M, et al. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J Med Virol. 2020; 92 (6), 589-94.
[37] Loon SC, Teoh SCB, Oon LLE, et al. The severe acute respiratory syndrome coronavirus in tears. Br J Ophthalmol. 2004; 88 (7), 861-3.
[38] Chan WM, Yuen KSC, Fan DSP, et al. Tears and conjunctival scrapings for coronavirus in patients with SARS. Br J Ophthalmol. 2004; 88 (7), 968-9.
[39] Dai X Peking University Hospital Wang Guangfa Disclosed Treatment Status on Weibo and Suspected Infection Without Wearing Goggles Xinjing Newpaper (2020). Available online at: http://wwwbjnewscomcn/news/2020/01/23/678189 (accessed January 24, 2020)
[40] World Health Organization Update 27 - One Month Into the Global SARS Outbreak: Status of the Outbreak and Lessons for the Immediate Future (2003) Available online at: https://www.who.int/csr/sars/archive/2003_04_11/en/
[41] Bonn D. SARS virus in tears? Lancet Infect Dis. 2004; 4 (8), 480.
[42] Tong TR, Lam BH, Ng TK, et al. Conjunctiva-upper respiratory tract irrigation for early diagnosis of severe acute respiratory syndrome. J Clin Microbiol. 2003; 41 (11), 5352.
[43] Pitkäranta A, Virolainen A, Jero J, et al. Detection of Rhinovirus, Respiratory Syncytial Virus, and Coronavirus Infections in acute otitis media by reverse transcriptase polymerase chain reaction. Pediatrics. 1998; 102 (2), 291-5.
[44] Heikkinen T, Thint M, Chonmaitree T. Prevalence of various respiratory viruses in the middle ear during acute otitis media. N Engl J Med. 1999; 340 (4), 260-4.
[45] Hooper JE, Mostafa HH, et al. SARS-CoV-2 virus isolated from the mastoid and middle ear implications for covid-19 precautions during ear surgery. JAMA Otolaryngol Head Neck Surg. 2020; 146 (10), 964-6.
[46] van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020; 382 (16), 1564-7.
[47] World Health Organization (WHO), 2020d Infection Prevention and Control Guidance for COVID-19. Available online at: https://www.who.int/publications/i/item/10665-331495 Accessed date: 17 September 2020.
[48] Ong SWX, Tan YK, Chia, PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020; 323 (16), 1610-2.
[49] Duguid JP. The numbers and the sites of origin of the droplets expelled during expiratory activities. Edinb Med J. 1945; 52 (11), 385-401.
[50] Papineni RS, Rosenthal FS. The size distribution of droplets in the exhaled breath of healthy human subjects. J Aerosol Med. 1997; 10 (2), 105-16.
[51] Baron PA, Willeke K, Aerosol Measurement: Principles, Techniques, and Applications, second ed van Nostrand Reinhold. 2001, New York.
[52] Cox CS. Physical aspects of bioaerosols particles In: Cox, CS, Wathes, CM (Eds), Bioaerosols Handbook Lewis Publishers, Boca Raton, FL, USA, 1995. pp 15-25
[53] McCluskey R, Sandin R, Greene J. Detection of airborne cytomegalovirus in hospital rooms of immuno-compromised patients. J Virol Methods. 1996; 56 (1), 115-8.
[54] Hui DS, Chan PK. Severe acute respiratory syndrome and coronavirus. Infect Dis Clin North Am. 2010; 24 (3), 619-38.
[55] Olsen SJ, Chang HL, Cheung TYY, et al. Transmission of the severe acute respiratory syndrome on aircraft. N Engl J Med. 2003; 349 (25), 2416-22.
[56] McKinney KR, Gong YY, Lewis TG. Environmental transmission of SARS at Amoy Gardens. J Environ Health. 2006; 68 (9), 26-30.
[57] Bai Y, Yao L, Wei T, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA. 2020; 323 (14), 1406-7.
[58] World Health Organization (WHO), 2009 Natural Ventilation for Infection Control in Health-Care Settings. Available online at: https://www.who.int/water_sanitation_health/publications/natural_ventilation/en/ Accessed date: 17 September 2020.
[59] Wells WF. On air-borne infection: study II droplets and droplet nuclei. Am J Epidemiol. 1934; 20 (3), 611-8,
[60] Xie X, Li Y, Chwang AT, et al. How far droplets can move in indoor environments-revisiting the Wells evaporation-falling curve. Indoor Air. 2007; 17 (3), 211-25.
[61] Bourouiba L, Dehandshoewoercker E, Bush JWM. Violent respiratory events: on coughing and sneezing. J Fluid Mech. 2014; 745 (4), 537-63.
[62] Bourouiba L. Images in clinical medicine: a sneeze. N Engl J Med. 2016; 375 (8), e15.
[63] Bourouiba, L. Turbulent gas clouds and respiratory pathogen emissions: potential implications for reducing transmission of COVID-19 JAMA https://doiorg/10 1001/jama20204756. JAMA. 2020; 323 (18), 1837-8.
[64] Loh NHW, Tan Y, Taculod J, et al. The impact of high-flow nasal cannula (HFNC) on coughing distance: implications on its use during the novel coronavirus disease outbreak. Can J Anaesth. 2020; 67 (7), 893-4.
[65] World Health Organization (WHO), 2020e Management of ill Travellers at Points of Entry (International Airports, Seaports and Ground Crossings) in the Context of COVID-19. Available online at: https://www.who.int/publications/i/item/10665-331512 Outbreak Accessed date: 15 September 2020.
[66] Centers for Disease Control and Prevention (CDC), 2020b Travelers from Countries with Widespread Sustained (Ongoing) Transmission Arriving in the United States. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/travelers/after-travel-precautions.html Accessed date: 14 September 2020.
[67] Kumar P, Morawska L. Could fighting airborne transmission be the next line of defence against COVID-19 spread? City Environ Interact 4. 2019; 100033.
[68] Schuit M, Gardner S, Wood S, et al. The influence of simulated sunlight on the inactivation of influenza virus in aerosols. J Infect Dis. 2020; 221 (3), 372-8.
[69] Zhu Y, Xie J. Association between ambient temperature and COVID-19 infection in 122 cities from China. Sci Total Environ. 2020; 724, 138201.
[70] Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: a systematic review and meta-analysis. J Evid Based Med. 2020; 13 (2), 93-101.
[71] Balachandar V, Mahalaxmi I, Kaavya J, et al. COVID-19: emerging protective measures. Eur Rev Med Pharmacol Sci. 2020; 24 (6), 3422-5.
[72] Leung WWF, Sun Q. Electrostatic charged nanofiber filter for filtering airborne novel coronavirus (COVID-19) and nano-aerosols. Sep Purif Technol. 2020; 250, 116886.
[73] Derrick JL, Gomersall CD. Protecting healthcare staff from severe acute respiratory syndrome: filtration capacity of multiple surgical masks. J Hosp Infect. 2005; 59 (4), 365-8.
[74] Leung NH, Chu DK, Shiu EY, et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020; 26 (5), 676-80.
[75] Sandaradura I, Goeman E, Pontivivo G, et al. A close shave? Performance of P2/N95 respirators in health care workers with facial hair: results of the BEARDS (Adequate Respiratory DefenceS) study. J Hosp Infect. 2020; 104 (4), 529-33.
[76] Davies A, Thompson KA, Giri K, et al. Testing the efficacy of homemade masks: would they protect in an influenza pandemic? Disaster Med Public Health Prep. 2013; 7 (4), 413-8.
[77] Halaji M, Farahani A, Ranjbar R, et al. Emerging coronaviruses: first SARS, second MERS and third SARS-CoV-2: epidemiological updates of COVID-19. Infez Med. 2020; 28 (1), 6-17.
[78] Zhang R, Li Y, Zhang AL, et al. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci USA. 2020; 117 (26), 14857-63.