Le Infezioni in Medicina, n. 1, 130-137, 2021
CASE REPORTS
Multidrug-resistant Gram-negative post-neurosurgical meningitis and the role of intraventricular colistin: a case series
Chiara Iaria1, Giuseppe Roberto Giammalva2, Daria Spicola1, Anna Maria Fimognari3, Claudia Imburgia1, Francesco Di Lorenzo1, Antonio Ficalora1, Adriana Sanfilippo1, Vincenzo Mazzarese4, Antonio Scafidi4, Francesco Cimò5, Antonio Capodicasa6, Grazia Laura Marsala7, Antonella Saporito8, Francesca Di Bernardo8, Domenico Gerardo Iacopino2, Vito Fiorenza3
1U.O.C Malattie Infettive, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy;
2Neurosurgical Clinic, AOUP “Paolo Giaccone”, Department of Biomedicine Neurosciences and Advanced Diagnostic (BiND), School of Medicine, University of Palermo, Palermo, Italy;
3U.O.C Neurochirurgia, Dipartimento Testa-Collo, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy;
4U.O.C Anestesia e Rianimazione, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy;
5U.O.C Farmacia, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy;
6U.O. Risk Management, Direzione sanitaria, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy;
7Direzione Medica, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy;
8U.O.C. Microbiologia, A.R.N.A.S. Civico-Di Cristina-Benfratelli, Palermo, Italy
Corresponding author
Giuseppe Roberto Giammalva
E-mail: robertogiammalva@live.it
SummaRY
The aim of this study was to report the clinical experience of intraventricular colistin for the treatment of multi-resistant Gram-negative post-surgical meningitis in a tertiary hospital. Post-neurosurgical meningitis (PNM) is one of the life-threatening complications of neurosurgical procedures, and is frequently sustained by Acinetobacter baumannii and Klebsiella pneumoniae. Here we describe our experience of five cases of PNM caused by gram-negative multi-drug resistant (MDR) bacteria, treated with intraventricular (IVT) colistin, admitted to the Neurosurgery Unit of A.R.N.A.S. Civico of Palermo, Italy, from January 2016 to June 2020. In four patients the cerebrospinal fluid (CSF) culture was positive for A. baumannii, while in one patient it was positive for K. pneumoniae. IVT colistin therapy was administered for a median time of 18 days (range 7-29). The median time to CSF negativization was seven days (range 5-29). IVT colistin administration was associated with intravenous administration of meropenem and colistin in all patients. As regards clinical outcome, four patients were successfully treated and were subsequently discharged, while one patient died following respiratory complications and subsequent brain death. IVT colistin administration is an effective therapy for MDR post-neurosurgical meningitis and its administration is also prescribed by guidelines. However, IVT therapy for Gram-negative ventriculitis is mostly understudied. Our paper adds evidence for such treatment that can actually be considered life-saving.
Keywords: Intraventricular colistin, post-neurosurgical meningitis; MDR Gram-negative bacteria.
INTRODUCTION
Post-Neurosurgical Meningitis (PNM) are fearful complications of neurosurgical procedures among the short-term ones, burdened by high morbidity and mortality and determining an increase in hospitalization, care burden and therefore social costs [1]. In recent years, the widespread use of different classes of antibiotics, preoperative surgical antibiotic prophylaxis and the use of antibiotic-impregnated shunts against Gram positive, have profoundly altered the prevalence and epidemiology of the microorganisms causing PNM. In facts, today several cases of PNM are sustained by Gram-negative bacteria, of which an increasing proportion are multidrug-resistant (MDR) [1]. In particular, Acinetobacter baumannii and Klebsiella pneumoniae have recently emerged as etiological agents most frequently implicated in these cases [1, 2].
Here, we describe our experience of five cases of PNM caused by Gram-negative MDR bacteria, treated with intraventricular (IVT) colistin, admitted to the Neurosurgery Unit of A.R.N.A.S. Civico of Palermo, Italy, from January 2016 to June 2020.
CASE SERIES
First case
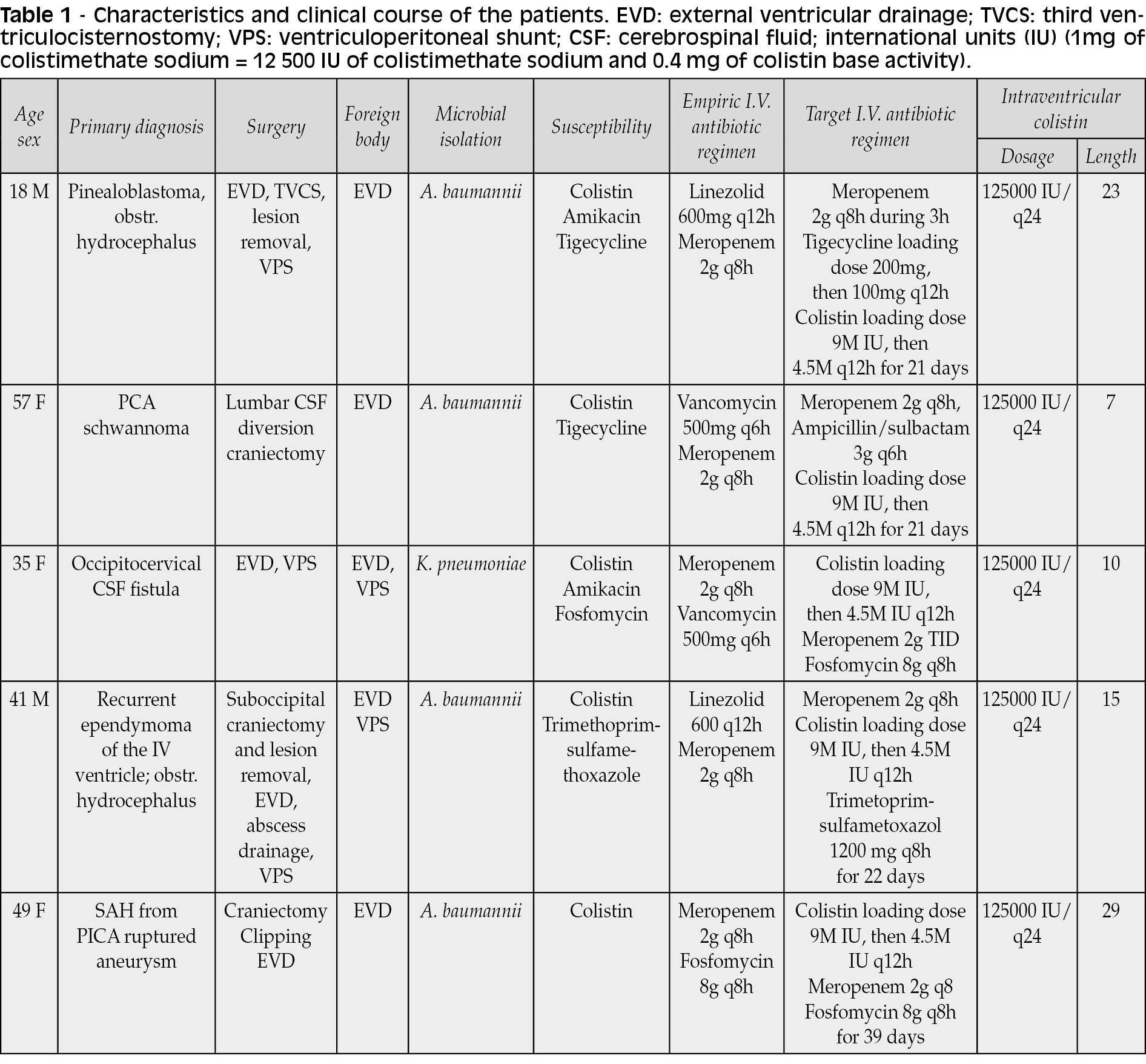
An 18-year-old male referred to the Emergency Department of our Institution due to the onset of lower limb asthenia, hearing loss, bilateral low vision, and psychomotor slowdown. A brain Computed Tomography (CT) scan was performed showing a rounded lesion in the pineal site causing severe obstructive hydrocephalus, flattening of the cerebral sulci, and trans ependymal transudation. He was transferred to the Neurosurgery Unit and then he underwent External Ventricular Drainage (EVD). The following day a brain MRI with contrast medium was performed, raising suspicion of “pinealoblastoma”, for which he underwent endoscopic third ventriculocysternostomy and biopsy of the lesion. In the postoperative period, the patient became febrile; so, blood and cerebrospinal fluid (CSF) cultures were performed and empiric antibiotic therapy with linezolid 600 mg q12h and 3-hours slow infusion meropenem 2 g q8h was established, with a resolution of the symptoms. CSF and blood culture were negative. Once the patient was clinically stabilized, after repositioning the right EVD, he underwent suboccipital craniectomy and subtotal removal of the pineal lesion through infratentorial supracerebellar approach. Then, he was transferred to post-surgical intensive care unit. Four days after the procedure, the patient became febrile; CSF chemical-physical examination revealed LDH 314 U/L, proteins 3601 mg/L, glucose 10 mg/dL, cellularity 2100/µL; MDR A. baumannii, (susceptible to colistin and tigecycline, intermediate to amikacin, resistant to quinolones, trimethoprim/sulfamethoxazole and carbapenems) was isolated from the CSF culture. At this time a brain MRI was performed which revealed marked thickening of brain ependyma with strong contrast enhancement due to ependymitis [Figure 1a].

Figure 1 - Pre-treatment brain imaging before IVT colistine administration. a: patient no. 1 brain MRI. b: patient no. 2 brain MRI. c: patient no. 3 brain MRI. d: patient no. 4 brain MRI. e: patient no. 5 brain CT.
Triple intravenous antibiotic therapy was then set up with 3-hours slow infusion meropenem 2 gr q8h, colistin 4.5 million IU q12h (after a loading dose of 9 M IU), and tigecycline 100 mg q12h preceded by a loading dose of 200 mg, associated with IVT therapy with colistin 10 mg (125,000 IU CMS) q24h. Bacterial CSF clearance time was 7 days. The above antibiotic therapy was continued for 21 days. No adverse events and no therapy-related toxicity were recorded. Then he underwent ventriculo-peritoneal shunt and revision of the suboccipital wound a month after the onset of PNM; then he was transferred to the Onco-Hematology Unit of our Institution for the follow-up. During the last month of hospitalization, the patient underwent chemotherapy with cisplatin and etoposide and pressure sores on his heels and in the occipital region were treated daily. The patient also underwent physical therapy with the gradual recovery of motor skills in the lower limbs. He was discharged in fair general conditions with the activation of integrated home assistance.
Second case
A 57-year-old woman was admitted to the Neurosurgery Unit of our Institution for a left ponto-cerebellar angle neoformation. She had been suffering for a year from hearing loss on the left, instability, and deviation to the left while walking, paraesthesia on the left side of the face, and taste disturbances on the left side of the tongue.
After spinal CSF drainage, a left occipital craniectomy was performed and the lesion was removed. Following the pathological examination, an acoustic neuroma was discovered. Subarachnoid drainage for continuous CSF drainage was placed during surgery and it was removed in the sixth postoperative day. The same day, the patient became dyspneic and sleepy with episodes of uncontrollable vomiting, then she was transferred to the intensive care unit. Cultures of CSF, blood, and bronchial alveolar lavage were performed, and an empirical antibiotic therapy was started with vancomycin 500 mg IV q6h and 3 hours slow infusion of meropenem 2 gr IV q8h. The patient’s CSF was cloudy with a glucose concentration of 20 mg/dl, a LDH concentration of 243 U/L, a protein level of 5595 mg/L, and a WBC count of 20336/µL, with 92.8% polymorphonuclear leukocytes and 7.2% lymphocytes. A few days later, cultures of CSF, blood, and bronchial alveolar lavage yielded A. baumannii resistant to carbapenems, cephalosporins, fluoroquinolones, aminoglycosides, and trimethoprim-sulphamethoxazole, and sensitive only to colistin. At this time, brain MRI showed a widespread leptomeningeal and cortico-pial contrast enhancement [Figure 1b]
On the basis of the antibiogram, antibiotic therapy was modified: 3-hours slow infusion of meropenem 2 g IV q8h, ampicillin/sulbactam 3gr IV q6h, colistin 4.5M IU IV q12h after a loading dose of 9 M IU. On the fifth day after the patient’s worsening, EVD was placed and the administration of IVT colistin 10 mg (125.000 IU) q24h was started. Because the patient was still comatose, a week later the ICU’s admission a percutaneous tracheostomy was performed. Then the patient improved, became eupneic, alert, oriented, phasic, with crural left hemiparesis, left anacusis, and left VI cranial nerve deficit.
CSF cultures became negative after 7 days of IVT therapy and blood culture became sterile after 13 days of IV therapy. CSF chemical-physical parameters improved, glucose concentration was 62 mg/dl, protein level was 199 mg/L, and a WBC count of 109/µL, with 76% polymorphonuclear leukocytes. As clinical conditions and tests value improved, the EVD was removed and the antibiotic therapy stopped. No toxicity or adverse events occurred. The patient was discharged and transferred to a rehabilitation center.
Third case
A 35-year-old woman was readmitted to Neurosurgery Unit for CSF leakage from a former occipital surgical wound. Two weeks before, she had undergone sub-occipital craniectomy, C1-C2 laminectomy, and C0-C1-C2 transitional meningioma removal, which hesitated in diparesis and paraplegia.
The day after the admission, after perioperative antibiotic chemoprophylaxis with cefazolin 2 gr IV, she underwent surgical wound revision with muscular graft. An EVD was placed in order to facilitate dural sealing and wound closure. After a few days, fever, leukocytosis and an increase in inflammation indices appeared. Cultures of CSF, blood, and bronchial alveolar lavage were performed and empirical antibiotic therapy with 3-hours slow infusion of meropenem 2 gr IV q8h and vancomycin 500 mg q6h was started. An emergent brain MRI without contrast medium revealed the presence of particulate fluid matter within the surgical field [Figure 1c].
Baseline chemical-physical examination of CSF before antibiotic therapy showed a protein level of 2200 mg/L, LDH 163 U/L, and glucose concentration of 14 mg/dl. CSF culture revealed KPC K. pneumoniae only susceptible to colistin, amikacin, and fosfomycin, whereas blood and urine showed no bacterial growth. Antibiotic therapy was enhanced by IV colistin with a loading dose of 9M IU followed by 4,5M IU q12h and IVT colistin 125.000 IU (10 mg) q24h. After 48 hours, the patient showed a progressive improvement, she became afebrile, eupneic, alert, oriented, and underwent physical therapy.
IVT colistin therapy lasted 10 days, CSF sterilization was obtained after 5 days of IVT therapy. CSF chemical-physical parameters improved: glucose concentration was 54 mg/dl, protein level was 376 mg/L, and a WBC count of 405/µL, with 56% polymorphonuclear leukocytes. By then, EVD was removed.
Six days later, suddenly, the patient had visual hallucinations, became confused and disoriented, a brain CT scan revealed an acute hydrocephalous so she underwent ventriculoperitoneal shunt on the same day with progressive neurological improvement. Antibiotic therapy was stopped after twenty days, with no toxicity or adverse events. The patient was transferred to a neuro-rehabilitation center in order to continue physical therapy.
Fourth case
A 41-year-old male was admitted to the Neurosurgery Unit for the recurrence of a fourth ventricle ependymoma. On admission, the patient was conscious, with weakness in all four limbs and ataxic walk. He underwent suboccipital craniectomy and lesion removal prior to antibiotic chemoprophylaxis with cefazolin 2 g IV, which was maintained during the following clinical course. The patient was then transferred to the ICU for post-operative care and monitoring, and he was transferred back to the Neurosurgery Unit on the second postoperative day without any neurological impairments. On the third postoperative day he became febrile with a remitting fever up to 38.8°C and worsening of consciousness. The blood cell counts revealed WBC 1755/µL, blood culture was negative, and an empirical IV antibiotic therapy with 3-hours slow infusion of meropenem 2 g q8h and linezolid 600 mg q12h was administered. On the eighth postoperative day EVD was placed because of obstructive hydrocephalus. The CSF culture revealed A. baumannii resistant to aminoglycosides, fluoroquinolones, carbapenems, and susceptible only to colistin, trimethoprim-sulfamethoxazole, and tigecycline. The CSF examination revealed an LDH concentration of 85 U/L, a protein level of 1879 mg/L, a glucose concentration of 9 mg/dl, and a WBC count of 1970/µL. An antibiotic IV therapy with trimethoprim-sulfamethoxazole, 3-hours slow infusion of meropenem 2g q8h and intravenous 9M IU loading dose of colistin followed by 4.5 MUI q12h were started. At this time patient underwent contrast brain MRI which revealed a strong contrast enhancement of the III, IV, and lateral ventricles, dural enhancement within the surgical field, congestion of cortical vessels, and the presence of particulate CSF [Figure 1d]. The following day CSF culture became negative, but the patient was still febrile so intravenous antibiotic therapy was maintained, and IVT therapy with colistin 125.000 IU (10 mg) q24h was started on the fifteenth postoperative day. Because of the evidence of cerebellar abscess on brain MRI and CSF leakage patient underwent drainage of the abscess and subsequent dural repair. The cultural examination of the intraoperative specimen was negative. IVT therapy with colistin was administered for a total of 15 days. At this time CSF examination revealed an LDH concentration of 32U/L, a protein level of 774 mg/L, a glucose concentration of 46 mg/dl, and a WBC count of 19/µL. The following clinical course was uneventful, the patient kept afebrile and following blood and CSF cultures were negative; so, he underwent a ventriculoperitoneal shunt. Intravenous therapy with colistin 4.5M U q12h, meropenem 2g q8h and sulfamethoxazole-trimethoprim, was maintained for other 7 days, until the patient was discharged to a rehabilitative institution.
Fifth case
A 49-year-old woman was admitted to the Intensive Care Unit of our Institution with subarachnoid hemorrhage and IVT hemorrhage. On admission, the patient was comatose with a Glasgow Coma Scale (GCS) 8 and brain CT scan revealed the presence of increasing obstructive hydrocephalus. The patient underwent urgent EVD prior to antibiotic chemoprophylaxis with cefazolin 2g IV. On the following day brain CT angiogram revealed a ruptured aneurysm of the posterior-inferior cerebellar artery (PICA), so the patient underwent suboccipital craniectomy and clipping of the aneurysm. The clinical course was uneventful and on the third day, the patient was transferred to the Neurosurgery Unit of our Institution with good neurological conditions. On the tenth day she presented remitting fever up to 38.5°C, The CSF turned to be opalescent and the CSF examination revealed an LDH concentration of 34U/L, a protein level of 833 mg/L, a glucose concentration of 80 mg/dl, and a WBC count of 482/µL. Gram staining of CSF revealed early growth of Gram-negative colonies. Initial therapy with 3-hours slow infusion of meropenem 2 gr q8h and fosfomycin 6gr q6h was started. Brain MRI showed the presence of dural and ependymal thickening, a marked enhancement of the IV ventricle ependyma, and the presence of enhancing phlogistic tissue within the right lateral ventricle [Figure 1e]. Two days later CSF culture yielded A. baumannii. It was resistant to aminoglycosides, fluoroquinolones, carbapenems, trimethoprim-sulfamethoxazole, and it was susceptible only to colistin and tigecycline. After the microbial identification, 9M IU loading dose of colistin followed by 4.5 MUI q12h were added and IVT therapy with colistin 125.000 IU (10 mg) q24h was started in association with previous parenteral therapy. The patient became afebrile two days after the administration of IVT colistin. After 28 days of IVT therapy, EVD was substituted because of an obstruction, and the days later CSF culture became negative. At this time CSF examination revealed an LDH concentration of 30U/L, a protein level of 559 mg/L, a glucose concentration of 100mg/dl, and a WBC count of 26/µL. IVT therapy was stopped. Later the patient became again febrile and a lung CT scan revealed bilateral inferior lobar pneumonia. Because of the worsening of consciousness and the onset of respiratory complications, the patient was intubated and transferred to ICU. Unfortunately, the patient died five days later because of severe respiratory failure and subsequent brain death.
DISCUSSION
From the analysis of the data collected, the selected patients had an average age of 40±13 years (range 18-57). Regarding the primary diagnosis and the type of related surgical procedure, three patients underwent craniotomy and removal of an expansive brain lesion, one patient underwent revision of a CSF secondary to the previous removal of an occipital-cervical expansive lesion, one patient underwent craniectomy and clipping of ruptured aneurysm formation in the posterior cranial fossa.
In four patients the CSF culture test was positive for A. baumannii, in one patient it was positive for K. pneumoniae.
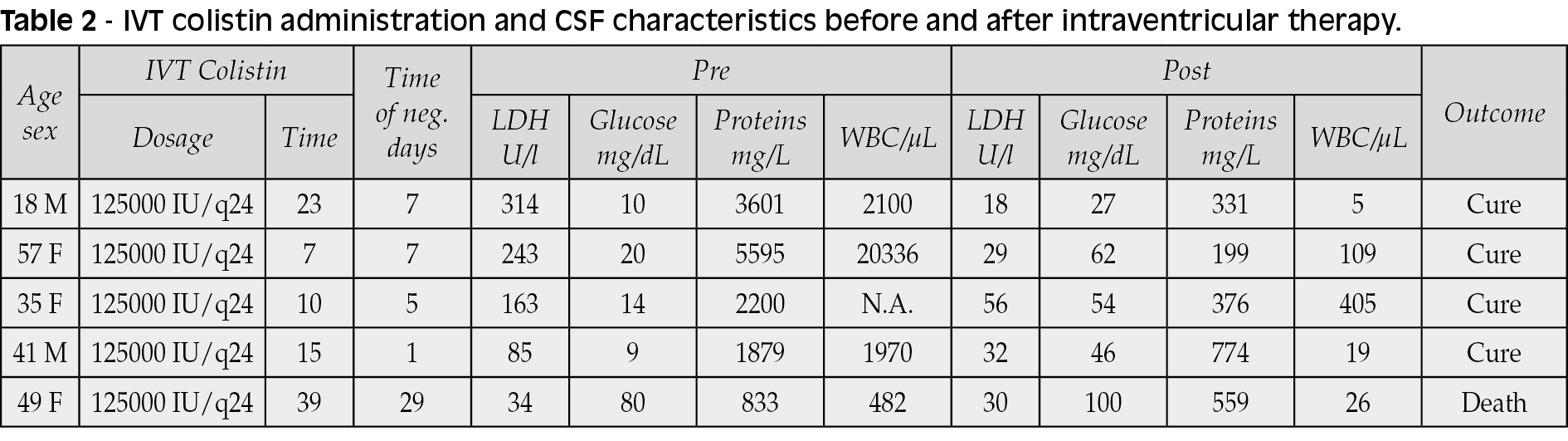
From the chemical-physical characteristics of the CSF prior to the administration of IVT colistin, they showed a mean protein level of 2821 mg/L (range 833-5594 mg/L), an average glucose concentration of 21mg/dl (1-80 mg/dl), an LDH concentration of 168 U/ml (34-314 U/L) and median cellularity of 1226 cells /µL.
Intraventricular colistin therapy was administered for a median time of 18 days (range 7-29). The median time to CSF negativization was 7 days (range 5-29). No toxicities associated with colistin administration were recorded. Intraventricular colistin administration was associated with intravenous administration of meropenem and colistin in all patients; in one patient also with tigecycline, in one patient with ampicillin/sulbactam, in one patient with fosfomycin, in one patient with trimethoprim/sulfamethoxazole. Of note, IVT tigecycline is considered an attractive and promising last-resort therapeutic option for treating patients with healthcare-associated bacterial ventriculitis and meningitis [15].
Following IVT therapy and negativization of the CSF, the chemical-physical characteristics of CSF showed an average protein level of 448 mg/L (range 199-774 mg/L), an average glucose concentration of 58 mg/dl (27-100 mg/dl), an LDH concentration of 33 U/ml (18-56 U/L) and a median cellularity of 26 cells/µL.
All patients underwent multiple neurosurgical procedures. Four patients were admitted to intensive care.
Regarding the clinical outcome, four patients were successfully treated and were subsequently discharged, one patient died following respiratory complications and subsequent brain death.
In the third and fourth cases, the persistence of cells in the CSF in the absence of bacterial growth is due to chemical ventriculitis, a possible complication of IVT therapy which in both cases fortunately was not associated with convulsions. In a recent meta-analysis chemical ventriculitis was reported in 11% of cases treated intraventricularly or intrathecally [3].
In all cases colistin IVT therapy was associated with meropenem administered in extended infusion. Several studies demonstrate the usefulness of this association thanks to a synergistic effect between the two antibiotics, even if a recent meta-analysis has questioned such evidence [4, 5]. The extended infusion of meropenem allows to make the most of its pharmacokinetic characteristics [6].
The addition of fosfomycin is justified by the fact that this antibiotic has shown synergism against A. baumanni with colistin and diffuses adequately in CSF [7, 8].
The IVT antibiotics have been shown to be safe in a small number of cases. In a study of post-neurosurgery patients with meningitis and ventriculitis, 15 out of 27 patients who were given IVT antibiotics had negative CSF cultures within 48 hours (68 percent) [13]. The mean time to CSF sterilization was three days overall (range 1 to 12 days) and 6.5 days among the subset of patients with ventriculitis. From a retrospective study from China, 14 patients with Gram-negative bacterial meningitis received IVT antimicrobial therapy after an average of 25 days of intravenous antibiotics. The average time to sterilize the CSF was approximately six days. Despite the fact that certain patients displayed drug resistance due to highly-resistant strains of bacteria, 11 out of 15 (73% of patients) were judged to be clinically cured [14]. For treatment of ventriculitis, which accompanies Gram-negative bacillary meningitis most studies recommend that intravenous antibiotics should be given simultaneously if IVT antibiotics are used. In the review by Cascio et al, 24 cases of Acinetobacter ventriculitis treated with colistin administered by an IVT route were analyzed. The daily dose of colistin used ranged from 1.6 mg every 24 h to 20 mg every 24 h in adult patients. The median time necessary to obtain cerebrospinal fluid sterilization was 4.1 days, and treatment was always successful even if in two cases Acinetobacter meningitis relapsed. Toxicity probably or possibly related to the topical administration of colistin was noted in five out of the 32 patients [2].
In conclusion healthcare-associated ventriculitis and meningitis are common complications in patients with head trauma or neurosurgery. Health-associated ventriculitis and meningitis cause substantial morbidity and mortality including recurrent vegetative condition, mild and serious impairment, and death [9]. A. baumannii is the causative pathogen in 3.6-11.2% of health-related meningitis cases [10]. The new recommendations for healthcare-associated ventriculitis and meningitis from the Infectious Diseases Society of America recommend meropenem for treatment of cases infected with Acinetobacter spp, while polymyxins are recommended for carbapenem-resistant strains [11]. The guidelines also prescribe IVT or intrathecal polymyxin administration for patients with healthcare-associated A. baumannii meningitis and ventriculitis hard-to-treat with IV polymyxins [11]. Notwithstanding healthcare-associated cases of difficult-to-treat A. baumannii ventriculitis and meningitis are increasingly common, IVT therapy for Gram-negative ventriculitis is mostly understudied. Medical management of IVT antibiotics should be conducted in consultation with infectious disease specialists and neurosurgeons. Our paper adds evidence for such treatment that can actually be considered life-saving.
Conflicts of interest
None.
Funding
None.
REFERENCES
[1] Hussein K, Bitterman R, Shofty B, Paul M, Neuberger A. Management of post-neurosurgical meningitis: narrative review. Clin Microbiol Infect. 2017; 23 (9), 621-8.
[2] Cascio A, Conti A, Sinardi L, et al. Post-neurosurgical multidrug-resistant Acinetobacter baumannii meningitis successfully treated with intrathecal colistin. A new case and a systematic review of the literature. Int J Infect Dis. 2010; 14 (7), e572-9.
[3] Brotis AG, Churi I, Karvouniaris M. Local complications of adjunct intrathecal antibiotics for nosocomial meningitis associated with Gram-negative pathogens: a meta-analysis. Neurosurg Rev. 2019. doi: 10.1007/s10143-019-01226-w.
[4] Li JK, Fu Y, Zhang J, et al. The efficacy of colistin monotherapy versus combination therapy with other antimicrobials against carbapenem-resistant Acinetobacter baumannii ST2 isolates. J Chemother. 2020; 32 (7), 359-67.
[5] Nutman A, Lellouche J, Temkin E, et al. Colistin plus meropenem for carbapenem-resistant Gram-negative infections: in vitro synergism is not associated with better clinical outcomes. Clin Microbiol Infect. 2020; 26 (9), 1185-91.
[6] Gudiol C, Cuervo G, Carratalà J. Optimizing therapy of bloodstream infection due to extended-spectrum β-lactamase-producing Enterobacteriaceae. Curr Opin Crit Care. 2019; 25 (5), 438-48.
[7] Sirijatuphat R, Thamlikitkul V. Preliminary study of colistin versus colistin plus fosfomycin for treatment of carbapenem-resistant Acinetobacter baumannii infections. Antimicrob Agents Chemother. 2014; 58 (9), 5598-601.
[8] Pfausler B, Spiss H, Dittrich P, Zeitlinger M, Schmutzhard E, Joukhadar C. Concentrations of fosfomycin in the cerebrospinal fluid of neurointensive care patients with ventriculostomy-associated ventriculitis. J Antimicrob Chemother. 2004; 53 (5), 848-52.
[9] Srihawan C, Castelblanco RL, Salazar L, et al. Clinical characteristics and predictors of adverse outcome in adult and pediatric patients with healthcare-associated ventriculitis and meningitis. Open Forum Infect. Dis. 2016; 3 (2), ofw077.
[10] Karaiskos I, Galani L, Baziaka F, Giamarellou H. Intraventricular and intrathecal colistin as the last therapeutic resort for the treatment of multidrug-resistant and extensively drug-resistant Acinetobacter baumannii ventriculitis and meningitis: A literature review. Int. J Antimicrob Agents. 2013; 41 (6), 499-508.
[11] Tunkel A, Hasbun, R, Bhimraj A, et al. 2017 Infectious Diseases Society of America’s clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Clin Infect Dis. 2017; 64 (6), e34-e65.
[12] Abdallah M, Alsaleh H. A review of safety and effectiveness of intravenous and intraventricular tigecycline in healthcare-associated Acinetobacter baumannii meningitis and ventriculitis. Curr Treat Options Infect Dis. 2019; doi:10.1007/s40506-019-00192-7.
[13] Remeš F, Tomáš R, Jindrák V, Vaniš V, Setlík M. Intraventricular and lumbar intrathecal administration of antibiotics in postneurosurgical patients with meningitis and/or ventriculitis in a serious clinical state. J Neurosurg. 2013; 119 (6), 1596-602.
[14] Wang JH, Lin PC, Chou CH, et al. Intraventricular antimicrobial therapy in postneurosurgical Gram-negative bacillary meningitis or ventriculitis: a hospital-based retrospective study. J Microbiol Immunol Infect. 2014; 47 (3), 204-10.
[15] Moulin S, Cordonnier C. Prognosis and outcome of intracerebral haemorrhage. Front Neurol Neurosci. 2015; 37, 182-92.