Le Infezioni in Medicina, n. 1, 102-113, 2021
ORIGINAL ARTICLES
Prophylactic letermovir decreases cytomegalovirus reactivation after stem cell transplantation: a single-center real-world evidence study
Bianca Serio1, Valentina Giudice1,2,3, Roberto Guariglia1, Raffaele Fontana1, Luca Pezzullo1, Maria Carmen Martorelli1, Idalucia Ferrara1, Laura Mettivier1, Matteo D’Addona1, Emilia Vaccaro4, Maddalena Langella1,5, Carmine Selleri1,3
1Hematology and Transplant Center, University Hospital “San Giovanni di Dio e Ruggi d’Aragona”, Salerno, Italy;
2Clinical Pharmacology, University Hospital “San Giovanni di Dio e Ruggi d’Aragona”, Salerno, Italy;
3Department of Medicine, Surgery and Dentistry “Scuola Medica Salernitana”, University of Salerno, Baronissi, Salerno, Italy;
4Transfusion Medicine, Molecular Biology Section, University Hospital “San Giovanni di Dio e Ruggi d’Aragona”, Salerno, Italy;
5Transplant Immunology Laboratory, Molecular Biology Section, University Hospital “San Giovanni di Dio
e Ruggi d’Aragona”, Salerno, Italy
Corresponding author
Valentina Giudice
E-mail: vgiudice@unisa.it
SummaRY
Cytomegalovirus (CMV) reactivation is a major cause of morbidity and mortality after organ or hematopoietic stem cell transplantation (HSCT). Letermovir (LTV) is a novel antiviral agent approved for CMV prophylaxis after allogeneic transplantation. In this single-center real-world study, we evidenced efficacy and safety of LTV for CMV prophylaxis in allogeneic HSCT recipients. A total of 133 consecutive patients who underwent autologous or allogeneic HSCT were included in the study, and a subgroup of 13 allogeneic HSCT recipients received CMV prophylaxis with LTV 240 mg/daily from day +7 to +100 (allo-LTV cohort). All patients in the allo-LTV cohort were at moderate or high risk of reactivation based on donor/recipient serology status, and 62% also received haploidentical HSCT and cyclophosphamide which further increased CMV reactivation risk. CMV infection rate was also compared to that observed in allogeneic HSCT patients without CMV prophylaxis and autologous recipients who have the lowest reported CMV infection incidence and were used as a control cohort. In our experience, patients receiving LTV showed a significant decline in CMV reactivation incidence to similar rates described in autologous HSCT recipients (7.7% of allogeneic LTV-treated vs 68% of allogeneic recipients without prophylaxis vs 15% of autologous patients; p<0.0001). The only patient in the allo-LTV cohort with CMV reactivation was a 25-year-old female with a diagnosis of very high-risk acute lymphoblastic leukemia who received a haploidentical HSCT after ex vivo T cell depletion. CMV reactivation occurred beyond LTV course, at +187 days from transplantation. In addition, we confirmed efficacy and safety of valganciclovir 450 mg/daily as pre-emptive therapy or for treatment of CMV disease in allogeneic and autologous HSCT recipients who experienced CMV reactivation even after LTV prophylaxis. However, further clinical trials in larger populations and longer follow-up are required to confirm our preliminary results.
Keywords: Cytomegalovirus, bone marrow transplantation, antiviral agents, letermovir.
INTRODUCTION
Cytomegalovirus (CMV), a human beta-herpesvirus, has an estimated worldwide seroprevalence of 45% to 100% increasing with age [1]. Primary infection usually occurs asymptomatically in immunocompetent subjects, and the virus remains in its latent form in CD34+ Hematopoietic Stem Cells (HSCs) and in CD33+ myeloid progenitors [2, 3]; however, only myeloid dendritic cells and monocytes can productively spread viral particles leading to CMV reactivation [4]. Immunosuppression is one of the major causes of reactivation, and immunocompromised subjects, such as solid-organ and HSC transplanted patients, can experience a more aggressive disease with hepatitis, severe pneumonia, central and peripheral nervous system manifestations, myelosuppression, and graft rejection [5-7]. Indeed, CMV reactivation remains one of the leading causes of morbidity and mortality after HSC transplantation (HSCT) frequently associated with other opportunistic infections and increased incidence of Graft versus Host Disease (GvHD) [8, 9]. In hematological patients receiving HSCT, CMV reactivation frequently occurs in the early post-engraftment phase with a cumulative incidence of 8-35% in the first year after transplantation and a mortality rate up to 70% due to CMV-related pneumonia complications [10-14]. Risk factors of CMV reactivation after HSCT are: pre-transplant CMV donor/recipient (D/R) serostatus, the most important independent factor with the highest risk with D-/R+ or D+/R+ [15]; recipient age; type of donor (matched unrelated, HLA mismatched, or haploidentical); source of HSCs; ex vivo T-cell depletion or administration of Anti-Thymocyte Globulin (ATG) or alemtuzumab; Reduced Intensity Conditioning (RIC) regimens; and development of GvHD treated with high-dose steroids [12, 16].
Since the introduction of specific antiviral agents, such as ganciclovir (GCV), and their rapid administration as early as detection of CMV-DNA copies by Polymerase Chain Reaction (PCR) and/or pp65 antigenemia (pp65), the incidence of CMV disease has dramatically decreased; however, mortality rate is still high especially in D-/R+ or D+/R+ or in those patients receiving T-cell depleted or matched/mismatched allogeneic HSCT [17]. Antivirals can be given in prophylaxis or as pre-emptive therapy when asymptomatic patients show positive CMV antigenemia or viremia [18]. GCV, valganciclovir (VGCV), foscavir, and cidofovir have limited use especially for prophylaxis because of their side effects, such as myelosuppression and nephrotoxicity [19].
Letermovir (LTV), a new antiviral agent, selectively disrupts CMV terminase complex preventing viral component assembling and acting differently from GCV that blocks viral DNA synthesis. Therefore, LTV reduces viral spread by interfering with both actively replicating and latent CMV forms [20]. Because of its efficacy and safety, LTV has been approved in 2017 for CMV prophylaxis and disease treatment in seropositive allogeneic HSCT recipients, and initial findings have reported a significant decrease of CMV disease after 24 weeks from transplant [20-23]. In this single-center real-world evidence study, we have investigated efficacy and safety of LTV in a cohort of allogeneic HSCT recipients, and incidence rates, clinical manifestations, type and duration of pre-emptive therapy, and Overall Survival (OS) were compared to those described in allogeneic recipients not receiving CMV prophylaxis and to autologous HSCT recipients.
PATIENTS AND METHODS
Patients and conditioning regimens
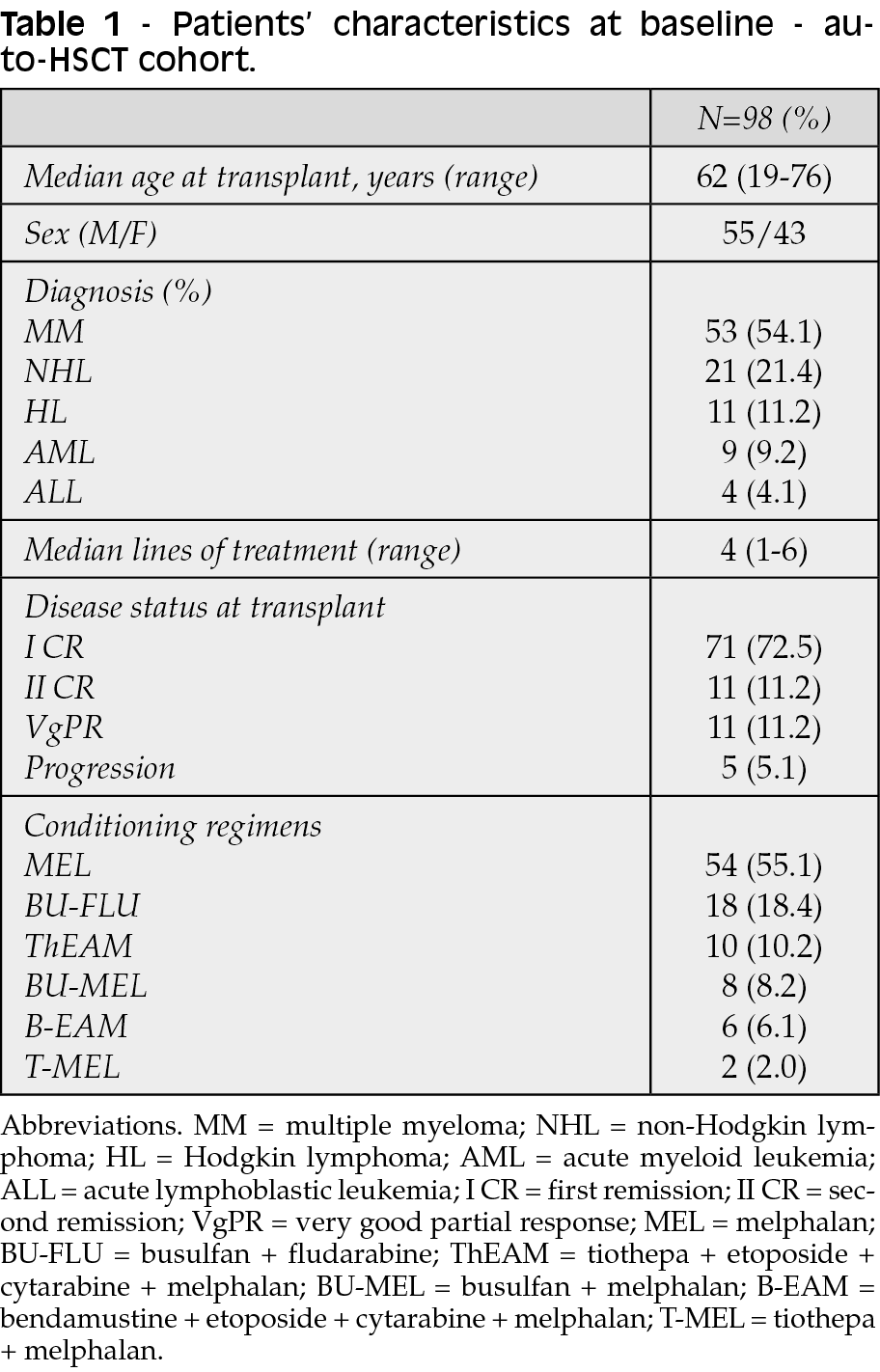
A total of 133 consecutive patients who underwent to HSCT at the Hematology and Transplant Center, University Hospital “San Giovanni di Dio e Ruggi d’Aragona” of Salerno, Italy, from February 2012 to September 2020, was included in this study. Patients were diagnosed with hematological diseases based on current international criteria, and received chemotherapy and HSCT following current international standards of care after informed consent obtained according to the Declaration of Helsinki [24-26]. Subjects were divided in three cohorts: autologous HSCT recipients (N=98; auto-HSCT); allogeneic HSCT recipients who did not receive LTV (N=22; allo-NO-LTV); and allogeneic HSCT recipients who received LTV for CMV prophylaxis (N=13; allo-LTV). Patients characteristics before autologous or allogeneic transplantation are summarized in Tables 1 and 2, respectively.
In the auto-HSCT cohort, patients were diagnosed with: multiple myeloma (MM; N=53); Non-Hodgkin Lymphoma (NHL; N=21); Hodgkin Lymphoma (HL; N=11); Acute Myeloid Leukemia (AML; N=9); and Acute Lymphoblastic Leukemia (ALL; N=4). Conditioning regimens were melphalan (MEL) 140 mg/m2 or 200 mg/m2 at day -1; busulfan 2.5 mg/kg and fludarabine 20 mg/m2 (BU-FLU) from day -5 to -2; thiotepa (T), etoposide, cytarabine (Ara-C), and melphalan (ThEAM); BU 3.2 mg/kg at days -3 to -2 and MEL 140 mg/m2 at day -2 (BU-MEL); bendamustine (300 mg/m2 at day -6), etoposide (200 mg/m2 from day -5 to -2), Ara-C (200 mg/m2 from day -5 to -2) and melphalan (140 mg/m2 at day -2) (B-EAM); or T-MEL (Table 1). Thirteen subjects (13.3%; MM, N=11; HL, N=1; and NHL, N=1) underwent to a previous autologous HSCT with a median time from first to second transplantation of 8 months (range, 3-52 months).
In the allo-NO-LTV cohort, patients received a diagnosis of AML (N=12), ALL (N=4), MM (N=3), myelodysplastic syndrome (MDS; N=2), and T-cell NHL (N=1). Nineteen (86.4%) received allogeneic HSCT from a matched sibling donor, while the remaining three subjects (13.6%) from haploidentical donor. Conditioning regimens were BU-FLU (FLU at 30 mg/m2) from day -6 to -3; RIC BU-FLU (BU 0.8 mg/kg, and FLU 30 mg/m2) from day -6 to -3. Two MM patients received FLU 30 mg/m2 from day -5 to -3 and MEL 70 mg/m2 from day -2 to -1; three AML subjects had T-BU-FLU; and one MM patient BU-MEL (BU 130 mg/m2 from day -7 to -4, and MEL 70 mg/m2 from day -2 to -1) (Table 2). Six subjects underwent to a previous autologous HSCT with a median time from first to second transplantation of 23.5 months (range, 19-50 months).
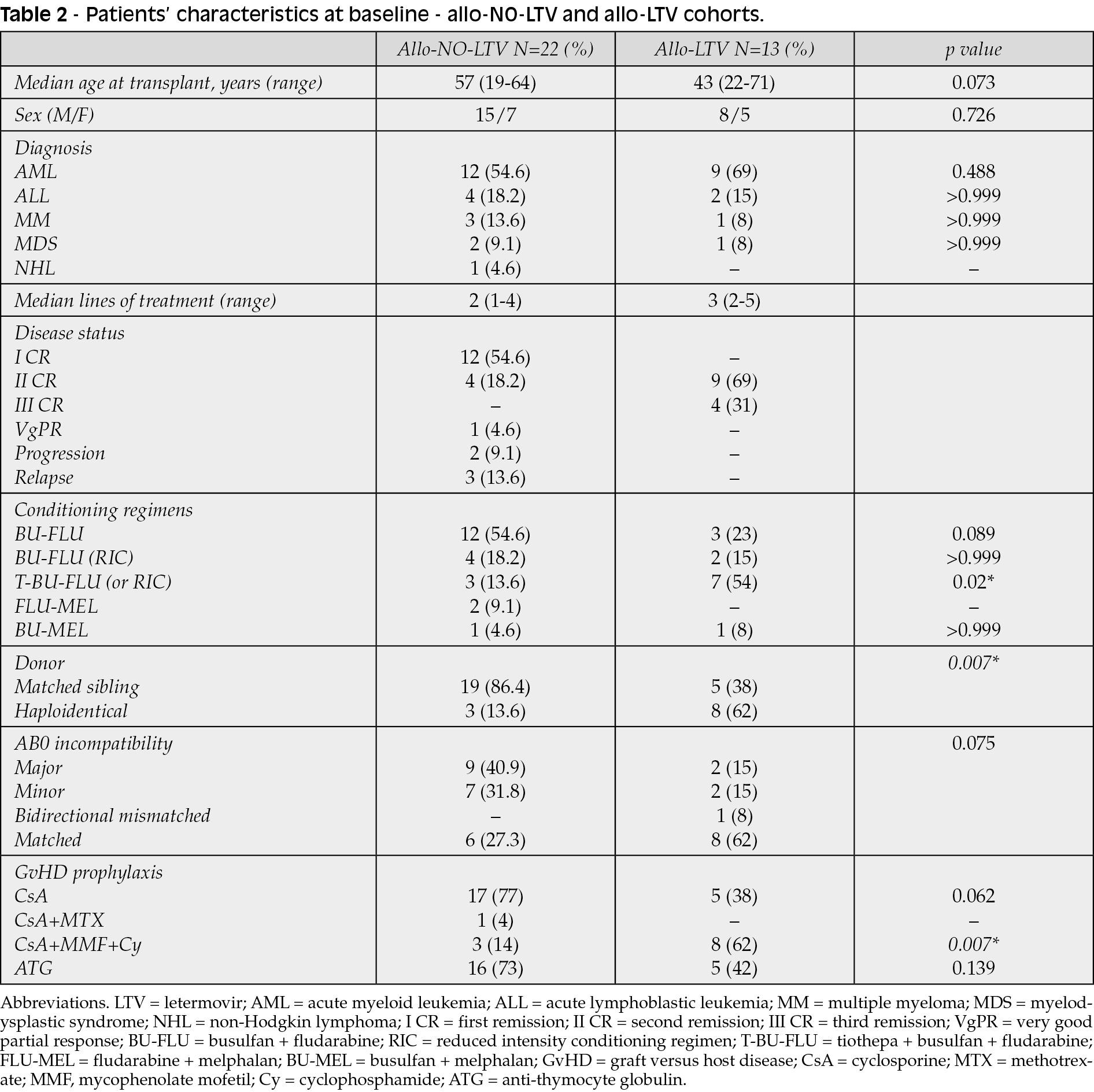
In the allo-LTV cohort, 38% of subjects (N=5) received allogeneic HSCT from a matched sibling donor, while 62% (N=8) from haploidentical donor. Nine patients had a diagnosis of AML, two ALL, one MDS, and one MM. Three AML patients received BU-FLU from day -6 to -3; one MDS and one AML a RIC BU-FLU from day -6 to -3; other five AML and two ALL subjects had T-BU-FLU, and cyclophosphamide post; and one MM patient received BU-MEL from day -2 to -1 (Table 2). A MM patient received two autologous HSCTs, while four AML subjects had a previous allogeneic HSCT from a matched sibling donor.
GvHD and CMV prophylaxis
In patients receiving allogeneic HSCT, acute GvHD (aGvHD) prophylaxis was performed according to current guidelines with cyclosporine A (CsA) at 1 mg/kg intravenously from day -1 to +21, then 8 mg/kg orally for at least 6 months with or without short-course methotrexate (MTX; 10 mg/kg at days+1, +3 +6 and +11), mycophenolate mofetil (MMF; 15 mg/kg/twice daily from day +1 to +28), or cyclophosphamide. Rabbit antithymocyte globuline (ATG) was administered at 5 mg/kg on days -3 to -1 (Table 2) [27]. Ex vivo T cell depletion was performed in two patients of the allo-LTV cohort.
In the allo-LTV cohort, CMV prophylaxis was performed with LTV at 240 mg/daily started at day +7 (range, from day +3 to +10) for 100 days. Two patients (one MDS and one AML) discontinued LTV because of a grade IV acute liver GvHD or disease relapse, respectively. In the autologous and allo-NO-LTV cohorts, patients did not receive CMV prophylaxis while were monitored for CMV reactivation and VGCV at 900 mg/daily was administered as soon as viral reactivation was diagnosed.
CMV-DNA quantification and serology
Specific anti-CMV Immunoglobulin G (IgG) levels were measured in patients and donors before transplantation. Plasma CMV-DNA copy number was quantified by real-time TaqMan CMV-DNA PCR according to manufacturers’ instructions (Roche) every three weeks in seropositive recipients of the auto-HSCT and allo-NO-LTV cohorts, or every two weeks for seropositive recipients of the allo-LTV cohort. After diagnosis of CMV reactivation, CMV-DNA levels were assessed every week until negativization. Instrument cut-off for positive results was CMV-DNA copy number >137 copies/µL.
Statistical analysis
Data were analyzed using Prism (v.8.3.0; GraphPad software, San Diego, CA). Two group comparison was performed by unpaired t-test, and one-way analysis of variance (ANOVA) for three-group comparison was carried out corrected with Tukey’s test for multiple comparisons. Differences in cumulative incidence of CMV reactivation between groups were assessed by Log-rank (Mantel-Cox) test. A p value <0.05 was considered statistically significant.
RESULTS
CMV reactivation in the auto-HSCT cohort
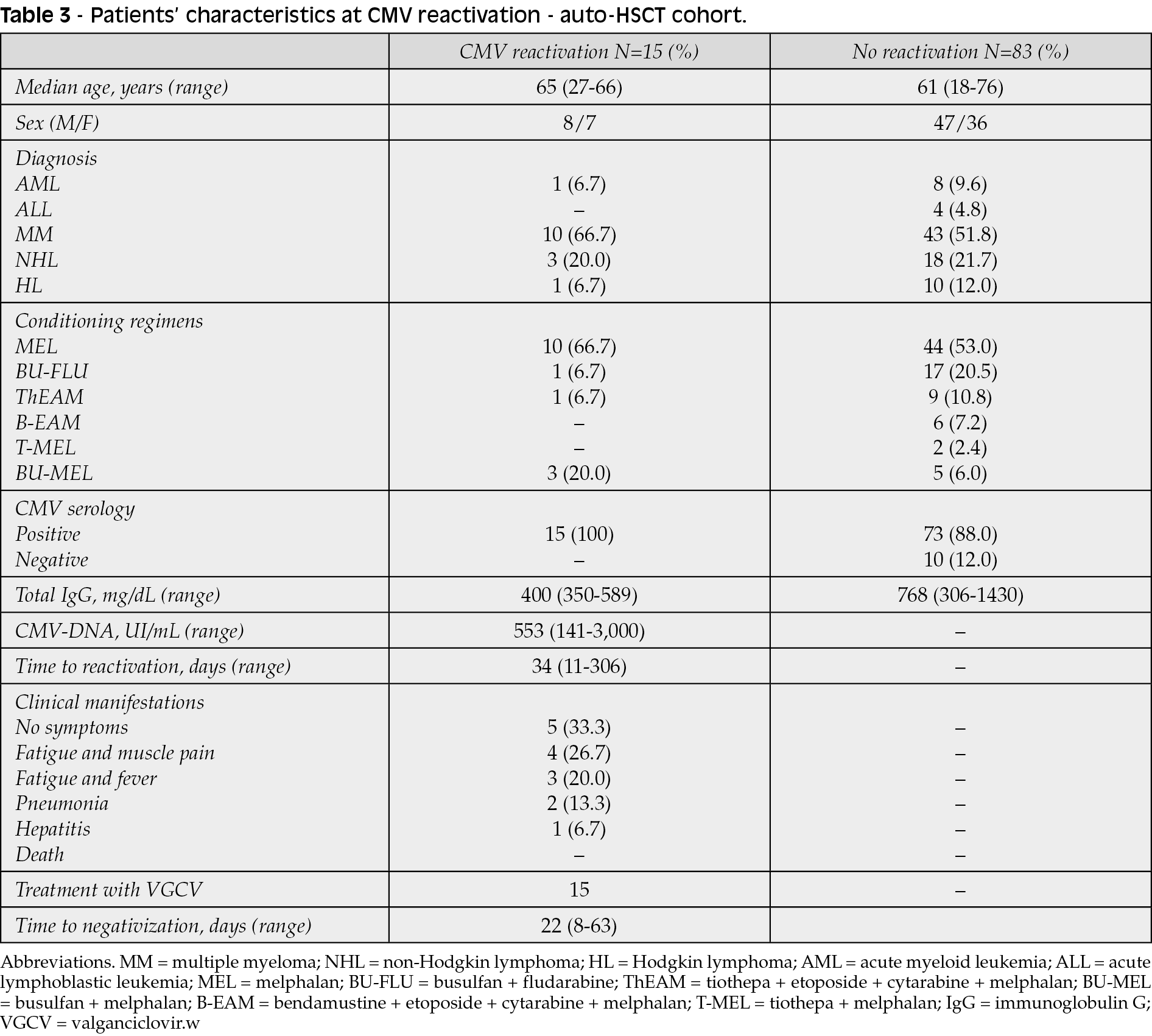
In the auto-HSCT cohort, 88 patients (89.8%) were seropositive for CMV, and reactivation was documented in 17% of them (N=15; MM, N=10; NHL, N=3; HL, N=1; and one AML) with a median age at reactivation of 59 years (range, 27-66 years), and 53% of them were males (Table 3). Median time to reactivation was 34 days (range, 11-306 days) with a median CMV-DNA copy number of 268 UI/mL (range, 141-3,000 UI/mL). At reactivation, five patients (33%) were asymptomatic; four (27%) had fatigue, muscle pain, and thrombocytopenia; three (20%) fever and fatigue; and three (20%) developed CMV disease. All 15 reactivated patients received VGCV 450 mg/twice daily until negativization of circulating CMV-DNA levels with a median length of treatment of 22 days (range, 8-63 days). None of those patients died because of CMV disease.
CMV reactivation in the allo-NO-LTV cohort
CMV serological status of recipients and donors in the allo-NO-LTV cohort was: D+/R+ in 82% of cases (N=18); D-/R+ in 14% of patients (N=3); and D+/R- in 5% of cases (N=1) (Table 4). Therefore, 87% of patients had low/high-moderate and 14% high risk of CMV reactivation. Fifteen patients (68%) experienced CMV reactivation, and 14 of them (93%) were D+/R+, while one subject was D-/R+. Ten (67%) out of those 15 patients with CMV reactivation had a diagnosis of AML, two (13%) MDS, two (13%) ALL, and one (7%) MM. Two high-risk subjects (13%) received HSCs from a haploidentical donor, and 13 (87%) from a matched sibling donor. Median age at reactivation was 54 years (range, 19-64 years old), and 60% of patients (N=13) were males. Median time to reactivation was 45 days (range, 7-640 days), with a median CMV-DNA copy number of 332 UI/mL (range, 140-50,000 UI/mL). Of the remaining seven subjects without CMV reactivation, two of them were D-/R+, four D+/R+, and one D+/R-; only one high risk subject received HSCs from a haploidentical donor, while the remaining six patients received allogeneic HSCT from a matched related donor. At reactivation, 47% of patients (N=7) were symptomatic mostly with fatigue, and fever (Table 4). All reactivated patients received VGCV 450 mg/twice daily until negativization of CMV viremia with a median length of treatment of 21 days (range, 9-150 days). Ten subjects (45.5%) developed aGvHD involving the skin or gastrointestinal system, and eight out of these 10 patients had CMV reactivation. Twelve subjects experienced chronic GvHD (cGvHD), and eight of them also had aGvHD involving skin, liver, gastrointestinal system, and/or lungs.

CMV reactivation in the allo-LTV cohort
All patients in the allo-LTV cohort were at moderate and high risk of reactivation as 77% of them (N = 10) were D+/R+, and 23% (N=3) D-/R+ (Table 5). Transplanted patients started CMV prophylaxis after a median of seven days (range, 3-10 days). The only patient with CMV reactivation was a 25-year-old female with a diagnosis of VHR ALL, and was D-/R+ receiving HSCs from a haploidentical donor after ex vivo T cell depletion. CsA and MMF were used for GvHD prophylaxis; however, she developed a grade II acute skin and gastrointestinal GvHD treated with CsA for three months, and a chronic limited hepatic GvHD at +163 days treated with budesonide and CsA. At +187 days, she also showed CMV reactivation (CMV-DNA copy number, 3,490 UI/mL) with fever, thrombocytopenia, and increased liver enzymes. No signs of pneumonia were documented by CT scan. Reactivation was treated with VGCV 450 mg/twice daily for 30 days. No other patients experienced viral reactivation. In the allo-LTV cohort, one subject died because of disease relapse at +62 days, one because of GvHD at +104 days, one for sepsis (+399 days), and one for liver failure at +118 days.

Incidence of CMV reactivation and outcomes
Cumulative incidence of post-HSCT CMV reactivation was significantly different among cohorts with the highest incidence in allogeneic HSCT recipients without CMV prophylaxis (p<0.0001) (Figure 1A). Significant differences were also described when considering only allogeneic HSCT recipients with or without CMV prophylaxis (p=0.0045). A total of 15 patients (15%) of the auto-HSCT cohort had CMV reactivation, 15 (68%) of the allo-NO-LTV cohort, and one (7.7%) in the allo-LTV cohort. All CMV-reactivated patients received VGCV 450 mg/twice daily until CMV-DNA negativization, and no differences were found in treatment length among cohorts (mean+SD, 29.5+16.2 days vs 34.1+35.8 days vs 30 days, auto-HSCT vs allo-NO-LTV vs allo-LTV; p=0.9006). In addition, no variations were observed in CMV-DNA copy number at reactivation (mean+SD, 506.7+727.6 UI/mL vs 5,811+13,445 UI/mL vs 187 UI/mL, auto-HSCT vs allo-NO-LTV vs allo-LTV; p=0.3130).
Next, OS were compared between cohorts, and no variations were described (p=0.3056) with median survivals of 46.8 months in the auto-HSCT cohort vs 61.5 months of allo-NO-LTV patients and vs 13.3 months of allo-LTV cohort, and six-month OS of 63.5%, 77.8%, and 85.7% (allo-LTV, allo-NO-LTV, and autologous HSCT cohorts respectively) (Figure 1B). No differences in OS were also observed between allo-NO-LTV and allo-LTV cohorts (p=0.0903). In each cohort, outcomes were also compared between CMV-reactivated and non-reactivated patients. In the auto-HSCT cohort, 3-year OS in reactivated patients was slightly higher than that of non-reactivated subjects (85.7% vs 54.3%), while similar 5-year OS were described (58.8% vs 47.5%). Despite this difference in first years after transplantation, OS between reactivated and non-reactivated patients was similar (p=0.4387), as well as OS of those receiving allogeneic HSCT without CMV prophylaxis (p=0.5930). In particular, in this cohort, 3-year OS was 71.4% in non-reactivated patients and 46.9% in CMV-reactivated subjects. In the allo-LTV cohort, the small number of censored subjects and the short follow-up could not allow to determine differences in 3- or 5-year OS; however, the six-month OS was 100% in patients with CMV reactivation and 58.3% in subjects without CMV reactivation (p=0.4833).

Figure 1 - Cumulative incidence of CMV reactivation and overall survival (OS). Transplanted patients were divided in three cohorts: autologous Hematopoietic Stem Cell Transplantation (HSCT) recipients (auto-HSCT); allogeneic HSCT recipients without CMV prophylaxis (allo-NO-LTV); and allogeneic HSCT recipients receiving letermovir (allo-LTV). (A) CMV reactivation events (1 reactivation/0 no reactivation) and related time to reactivation (days from transplantation) for each patient are represented among cohorts. (B) OS are reported in each cohort. A p < 0.05 was considered statistically significant.
DISCUSSION
To date, HSCT remains the only curative therapeutic strategy for various hematological malignancies or benign disorders, such as congenital bone marrow failure syndromes; however, several transplant-related complications, such as infectious diseases and GvHD, increase morbidity and mortality of transplant recipients. CMV reactivation is the most frequent post-HSCT infectious disease complication in seropositive patients, especially allogeneic HSCT recipients [11, 28]. In this single-center real-world evidence study, incidence of CMV reactivation was studied in autologous and allogeneic HSCT patients, and efficacy and safety of CMV prophylaxis with LTV was investigated.
Incidence of early-onset CMV disease has dramatically decreased after introduction of high-sensitivity PCR methodologies for early detection of circulating CMV-DNA allowing a prompt start of specific antiviral drugs (pre-emptive therapy) [29-32]. Despite these clinical advancements, CMV-related multiorgan disfunction and pneumonia are the major causes of death in transplanted patients especially those with CMV seropositivity [15, 17, 33, 34]. CMV prophylaxis and pre-emptive therapy are essential to reduce morbidity and mortality of post-transplant CMV disease [35]. Acyclovir, GCV, and VGCV have been historically used for CMV prophylaxis; however, these drugs frequently cause myelosuppression and nephrotoxicity and require intravenous administration [19, 36, 37]. Moreover, these drugs only act on active replicating virus, not on latent form, and risk of CMV reactivation after antiviral agent discontinuation is high [38]. LTV, a novel antiviral agent, inhibits the virus in both its replicating and latent status without causing myelosuppression and nephrotoxicity, and can half incidence of CMV reactivation at 14 and 24 weeks from allogeneic transplantation [23, 38]. In this study, no CMV reactivation at 14 weeks was documented in the cohort of transplanted patients receiving LTV as CMV prophylaxis, and only one (7.7%) reactivated after 12 weeks from LTV discontinuation per dose schedule (day +187); therefore, our cohort of allogeneic HSCT recipients receiving LTV displayed a significantly lower CMV reactivation rate than that of allogeneic recipients without CMV prophylaxis. We also compared incidences between allogeneic and autologous recipients used as a control group because autologous HSCT patients have the lowest reported CMV reactivation rate (<30%) [39, 40]. Indeed, our autologous patients had lower incidence of CMV reactivation compared to allogeneic HSCT; however, among allogeneic recipients, subjects who received LTV had CMV reactivation rates similar to that of autologous patients and lower than that of allogeneic subjects who did not receive CMV prophylaxis. CMV infection is particularly frequent in haploidentical recipients and reported to be the highest among allogeneic HSCT even under VGCV prophylaxis [41, 42]. Of note, 62% of our patients receiving LTV underwent to haploidentical transplantation and received cyclophosphamide post thus at very high risk of CMV reactivation; however, only one out of these eight subjects experienced CMV infection after 187 days from transplantation.
LTV can further decrease CMV disease rate and delay time to reactivation suggesting the beneficial of extension of LTV administration in allogeneic HSCT recipients especially in those with GvHD [43, 44]. An ongoing phase 3 randomized, double-blind, placebo-controlled clinical trial is evaluating efficacy and safety of LTV administered for 200 days post-transplant in R+ allogeneic HSCT (ClinicalTrials.gov Identifier, NCT03930615) because of clinical evidence from small case series of LTV efficacy in preventing CMV reactivation also as secondary prophylaxis [44]. In our cohort, the only reactivation was a high-risk patient who developed acute and chronic GvHD and CMV reactivation beyond the 100-day LTV schedule. However, although encouraging, our preliminary results from a small case series require further investigation and extension of number of patients and follow-up.
We have previously reported efficacy and safety of low-dose VGCV for CMV prophylaxis after allogeneic HSCT showing that VGCV is more effective than aciclovir in reducing CMV reactivation; however, administration needs to be started after engraftment because of increased risk of myelosuppresion [19, 22]. Our preliminary results showed that LTV was effective and safe when started seven days after transplant without affecting engraftment as no patient displayed LTV-related anemia, neutropenia, and/or thrombocytopenia. The most common drug-related adverse events were grade I gastrointestinal symptoms with rates similar to those reported [23]. LTV course was completed in 85% of cases and was discontinued in two subjects (15%) because of disease relapse or GvHD, similar to rates previously described [23]. Mori et al. in their multi-center real-world study also show an improvement in six-month OS and lower non-relapse mortality [45]; although six-month OS of our reactivated patients was slightly different between groups, the small number of censored subjects and the short follow-up did not allow to reach statistical significance in our single-center experience.
In conclusion, CMV disease still represents a life-threatening condition in allogeneic HSCT recipients, and effective prophylaxis is required to reduce morbidity and mortality related to CMV reactivation [10]. LTV is a novel antiviral agent approved as prophylactic therapy after allogeneic transplantation [23]. In this single-center real-world evidence study, we added evidence of efficacy and safety of LTV for CMV prophylaxis in allogeneic HSCT recipients, as incidence of CMV reactivation declined to similar rates described in autologous HSCT. However, further clinical trials in larger populations and longer follow-up are required to confirm our preliminary results.
Conflict of interest
The authors declare no conflicts of interest.
Funding
This research was supported by the Intramural Program of the Department of Medicine, Surgery and Dentistry, University of Salerno, Italy.
Acknowledgements
The authors would like to thank Daniela Pellegrino, Bianca Cuffa, and Francesca D’Alto (Hematology and Transplant Center, University Hospital “San Giovanni di Dio e Ruggi d’Aragona”) for technical assistance.
Author contributions
All authors have made substantial contributions to this paper. S.B, V.G., and C.S. designed the study. S.B., R.G., R.F, L.P., M.C.M., I.F., L.M., and M.D.A. enrolled patients and were involved in their clinical managements. E.V. and M.L. performed diagnostic tests. V.G., S.B., and R.B. collected clinical data. V.G. analyzed the data. V.G. and C.S. wrote the manuscript. All the authors reviewed the manuscript and agreed with the final version.
REFERENCES
[1] de Melo Silva J, Pinheiro-Silva R, Dhyani A, Pontes GS. Cytomegalovirus and Epstein-Barr Infections: Prevalence and Impact on Patients with Hematological Diseases. Biomed Res Int. 2020; 2020, 1627824.
[2] Reeves MB, MacAry PA, Lehner PJ, Sissons JG, Sinclair JH. Latency, chromatin remodeling, and reactivation of human cytomegalovirus in the dendritic cells of healthy carriers. Proc Natl Acad Sci. USA 2005; 102 (11), 4140-5.
[3] Khaiboullina SF, Maciejewski JP, Crapnell K, et al. Human cytomegalovirus persists in myeloid progenitors and is passed to the myeloid progeny in a latent form. Br J Haematol. 2004; 126 (3), 410-7.
[4] Minton EJ, Tysoe C, Sinclair JH, Sissons JG. Human cytomegalovirus infection of the monocyte/macrophage lineage in bone marrow. J Virol. 1994; 68 (6), 4017-21.
[5] Eid AJ, Bakri SJ, Kijpittayarit S, Razonable RR. Clinical features and outcomes of cytomegalovirus retinitis after transplantation. Transpl Infect Dis. 2008; 10 (1), 13-8.
[6] Ljungman P, Perez-Bercoff L, Jonsson J, et al. Risk factors for the development of cytomegalovirus disease after allogeneic stem cell transplantation. Haematologica. 2006; 91 (1), 78-83.
[7] Boeckh M, Boivin G. Quantitation of cytomegalovirus: methodologic aspects and clinical applications. Clin Microbiol Rev. 1998; 11 (3), 533-54.
[8] Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol. 2010; 20 (4), 202-13.
[9] Emery VC. Investigation of CMV disease in immunocompromised patients. J Clin Pathol. 2001; 54 (2), 84-88.
[10] Stern L, Withers B, Avdic S, et al. Human Cytomegalovirus Latency and Reactivation in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Front Microbiol. 2019; 10, 1186.
[11] Takenaka K, Nishida T, Asano-Mori Y, et al. Cytomegalovirus reactivation after allogeneic hematopoietic stem cell transplantation is associated with a reduced risk of relapse in patients with acute myeloid leukemia who survived to day 100 after transplantation: The Japan Society for Hematopoietic Cell Transplantation Transplantation-related Complication Working Group. Biol Blood Marrow Transplant. 2015; 21 (11), 2008-16.
[12] Slade M, Goldsmith S, Romee R, et al. Epidemiology of infections following haploidentical peripheral blood hematopoietic cell transplantation. Transpl Infect Dis. 2017; 19 (1), e12629.
[13] Boeckh M, Nichols WG, Papanicolaou G, Rubin R, Wingard JR, Zaia J. Cytomegalovirus in hematopoietic stem cell transplant recipients: Current status, known challenges, and future strategies. Biol Blood Marrow Transplant. 2003; 9 (9), 543-58.
[14] Erard V, Guthrie KA, Seo S, et al. Reduced mortality of cytomegalovirus pneumonia after hematopoietic cell transplantation due to antiviral therapy and changes in transplantation practices. Clin Infect Dis. 2015; 61 (1), 31-9.
[15] George B, Pati N, Gilroy N, et al. Pre-transplant cytomegalovirus (CMV) serostatus remains the most important determinant of CMV reactivation after allogeneic hematopoietic stem cell transplantation in the era of surveillance and preemptive therapy. Transpl Infect Dis. 2010; 12 (4), 322-9.
[16] George B, Kerridge IH, Gilroy N, et al. A risk score for early cytomegalovirus reactivation after allogeneic stem cell transplantation identifies low-, intermediate-, and high-risk groups: reactivation risk is increased by graft-versus-host disease only in the intermediate-risk group. Transpl Infect Dis. 2012; 14 (2), 141-8.
[17] Boeckh M, Nichols WG. The impact of cytomegalovirus serostatus of donor and recipient before hematopoietic stem cell transplantation in the era of antiviral prophylaxis and preemptive therapy. Blood. 2004; 103 (6), 2003-8.
[18] Prentice HG, Kho P. Clinical strategies for the management of cytomegalovirus infection and disease in allogeneic bone marrow transplant. Bone Marrow Transplant. 1997; 19 (2), 135-42.
[19] Serio B, Rosamilio R, Giudice V, et al. Low-dose valgancyclovir as cytomegalovirus reactivation prophylaxis in allogeneic haematopoietic stem cell transplantation. Infez Med. 2012; 20 (2), 26-34.
[20] Marschall M, Stamminger T, Urban A, Wildum S, Ruebsamen-Schaeff H, Zimmermann H, Lischka P. In vitro evaluation of the activities of the novel anticytomegalovirus compound AIC246 (letermovir) against herpesviruses and other human pathogenic viruses. Antimicrob Agents Chemother. 2012; 56 (2), 1135-7.
[21] Razonable RR. Role of letermovir for prevention of cytomegalovirus infection after allogeneic haematopoietic stem cell transplantation. Curr Opin Infect Dis. 2018; 31 (4), 286-91.
[22] Chemaly RF, Ullmann AJ, Stoelben S, et al. Letermovir for cytomegalovirus prophylaxis in hematopoietic-cell transplantation. N Engl J Med. 2014; 370 (19), 1781-9.
[23] Marty FM, Ljungman P, Chemaly RF, Maertens J, Dadwal SS, Duarte RF, et al. Letermovir prophylaxis for cytomegalovirus in hematopoietic-cell transplantation. N Engl J Med. 2017; 377 (25), 2433-44.
[24] Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016; 127 (20), 2391-405.
[25] Hsi ED. 2016 WHO Classification update. What’s new in lymphoid neoplasms. Int J Lab Hematol. 2017; 39 (1), 14-22.
[26] Halonen JI, Erhola M, Furman E, et al. The Helsinki Declaration 2020: Europe that protects. Lancet Planet Health. 2020; 4 (11), e503-5.
[27] Penack O, Marchetti M, Ruutu T, et al. Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020; 7 (2), e157-67.
[28] Nichols WG, Corey L, Gooley T, Davis C, Boeckh M. High risk of death due to bacterial and fungal infection among cytomegalovirus (CMV)-seronegative recipients of stem cell transplants from seropositive donors: evidence for indirect effects of primary CMV infection. J Infect Dis. 2002; 185 (3), 273-82.
[29] Madhavan HN, Samson MY, Ishwarya M, Vijayakumar R, Jambulingam M. “pp65 antigenemia and real time polymerase chain reaction (PCR) based-study to determine the prevalence of human cytomegalovirus (HCMV) in kidney donors and recipients with follow-up studies”. Virol J. 2010; 7, 322.
[30] Center for International Blood and Marrow Transplant Research (CIBMTR); National Marrow Donor Program (NMDP); European Blood and Marrow Transplant Group (EBMT); American Society of Blood and Marrow Transplantation (ASBMT); Canadian Blood and Marrow Transplant Group (CBMTG); Infectious Disease Society of America (IDSA); Society for Healthcare Epidemiology of America (SHEA); Association of Medical Microbiology and Infectious Diseases Canada (AMMI); Centers for Disease Control and Prevention (CDC). Guidelines for preventing infectious complications among hematopoietic cell transplant recipients: a global perspective. Bone Marrow Transplant. 2009; 44 (8), 453-558.
[31] Boeckh M, Gooley TA, Myerson D, Cunningham T, Schoch G, Bowden RA. Cytomegalovirus pp65 antigenemia-guided early treatment with ganciclovir versus ganciclovir at engraftment after allogeneic marrow transplantation: a randomized double-blind study. Blood. 1996; 88 (10), 4063-71.
[32] Cho SY, Lee DG, Kim HJ. Cytomegalovirus infections after hematopoietic stem cell transplantation: current status and future immunotherapy. Int J Mol Sci. 2019; 20 (11), 2666.
[33] Mikulska M, Raiola AM, Bruzzi P, et al. CMV infection after transplant from cord blood compared to other alternative donors: the importance of donor-negative CMV serostatus. Biol Blood Marrow Transplant. 2012; 18 (1), 92-9.
[34] Hemmersbach-Miller M, Alexander BD, Pieper CF, Schmader KE. Age matters: older age as a risk factor for CMV reactivation in the CMV serostatus-positive kidney transplant recipient. Eur J Clin Microbiol Infect Dis. 2020; 39 (3), 455-463.
[35] El Helou G, Razonable RR. Letermovir for the prevention of cytomegalovirus infection and disease in transplant recipients: an evidence-based review. Infect Drug Resist 2019; 12, 1481-1491.
[36] Boeckh M, Ljungman P. How we treat cytomegalovirus in hematopoietic cell transplant recipients. Blood. 2009; 113 (23), 5711-9.
[37] Goodrich JM, Bowden RA, Fisher L, Keller C, Schoch G, Meyers JD. Ganciclovir prophylaxis to prevent cytomegalovirus disease after allogeneic marrow transplant. Ann Intern Med. 1993; 118 (3), 173-8.
[38] Zawilinska B, Szostek S, Kopec J, Piatkowska-Jakubas B, Kosz-Vnenchak M. Multiplex real-time PCR to identify a possible reinfection with different strains of human cytomegalovirus in allogeneic hematopoietic stem cell transplant recipients. Acta Biochim Pol. 2016; 63 (1), 161-6.
[37] Crippa F, Corey L, Chuang EL, Sale G, Boeckh M. Virological, clinical, and ophthalmologic features of cytomegalovirus retinitis after hematopoietic stem cell transplantation. Clin Infect Dis. 2001; 32 (2), 214-9.
[38] Eid AJ, Bakri SJ, Kijpittayarit S, Razonable RR. Clinical features and outcomes of cytomegalovirus retinitis after transplantation. Transpl Infect Dis. 2008; 10 (1), 13-8.
[39] Marchesi F, Pimpinelli F, Gumenyuk S, et al. Cytomegalovirus reactivation after autologous stem cell transplantation in myeloma and lymphoma patients: a single-center study. World J Transplant. 2015; 5 (3), 129-36.
[40] Al-Rawi O, Abdel-Rahman F, Al-Najjar R, Abu-Jazar H, Salam M, Saad M. Cytomegalovirus reactivation in adult recipients of autologous stem cell transplantation: a single center experience. Mediterr J Hematol Infect Dis. 2015; 7 (1), e2015049.
[41] Lin CH, Su YJ, Hsu CY, Wang PN, Teng CJ. Haploidentical allogeneic hematopoietic stem cell transplantation increases the risk of cytomegalovirus infection in adult patients with acute leukemia. Transpl Infect Dis. 2019; 21 (4), e13096.
[42] Hammerstrom AE, Lombardi LR, Pingali SR, Rondon G, Chen J, Milton DR, et al. Prevention of cytomegalovirus reactivation in haploidentical stem cell transplantation. Biol Blood Marrow Transplant. 2018; 24 (2), 353-8.
[43] Bansal R, Gordillo CA, Abramova R, et al. Extended letermovir administration, beyond day 100, is effective for CMV prophylaxis in patients with graft versus host disease. Transpl Infect Dis. 2020; e13487.
[44] Shigle TL, Handy VW, Chemaly RF. Letermovir and its role in the prevention of cytomegalovirus infection in seropositive patients receiving an allogeneic hematopoietic cell transplant. Ther Adv Hematol. 2020; 11, 2040620720937150.
[45] Mori Y, Jinnouchi F, Takenaka K, et al. Efficacy of prophylactic letermovir for ytomegalovirus reactivation in hematopoietic cell transplantation: a multicenter real-world data. Bone Marrow Transplant. 2020; doi: 10.1038/s41409-020-01082-z.