Le Infezioni in Medicina, n. 1, 94-101, 2021
ORIGINAL ARTICLES
Prevalence of respiratory viruses by Multiplex PCR: a four-and-a-half year retrospective study in an Italian general hospital
Christian Leli, Luigi Di Matteo, Franca Gotta, Daria Vay, Andrea Piceghello, Elisa Cornaglia, Valeria Cavallo, Simone Busso, Laura Carrabba, Roberta Mazzeo, Andrea Rocchetti
Microbiology Laboratory, Azienda Ospedaliera SS. Antonio e Biagio e Cesare Arrigo, Alessandria, Italy
Corresponding author
Christian Leli
E-mail: christian.leli@ospedale.al.it
SummaRY
Viruses are frequent causal agents of acute respiratory infections and the most common are influenza virus, respiratory syncytial virus (RSV), human parainfluenza virus (HPIV), human metapneumovirus (HMPV), rhinovirus (RV), adenovirus (AdV) and the four endemic human coronaviruses (HCoV) -229E, -NL63, -OC43, -HKU1. Multiplex real-time PCR platforms are becoming increasingly common in laboratories mostly in relation to the increased diagnostic sensitivity and reduced turnaround time. The aim of our study was to determine the prevalence of respiratory viruses in a population of patients within the S.S. Antonio e Biagio e Cesare Arrigo General Hospital catchment area of Alessandria, Italy, from January 2016 to June 2020. Therefore, we retrospectively analyzed the results of multiplex real-time PCR performed on nasopharyngeal swabs collected from consecutive patients with symptoms of respiratory infection. A total of 572 patients were included in the study subdivided as follows: pediatric 197/572 (34.4%), adults 200/572 (35%) and elderly 175/572 (30.6%). Among all samples, 235/572 (41.1%) were positive for a respiratory virus, of whom 189/235 (80.4%) were monomicrobial. The prevalence was: 15.5% (89/572) of rhinovirus/enterovirus (RV/EV); 9.4% (54/572) of RSV; 8.9% (51/572) of influenza virus; 5.4% (31/572) of AdV; 3.1% (18/572) of HCoV; 2.8% (16/572) of HPIV; and 2.3% (13/572) of HMPV. RV/EV were the pathogens most frequently involved in coinfections (34.7%, 16/46), followed by AdV (19.6%, 9/46) and influenza virus (19.6%, 9/46). Samples collected from the pediatric group were more frequently positive. The prevalence of positive pediatric samples compared to adults and elderly, respectively was: 28.4% (56/197) for RV/EV vs 10.5% (21/200) vs 6.9% (12/175), p<0.0001; 18.8% (37/197) for RSV vs 2% (4/200) vs 7.4% (13/175), p<0.0001; 13.7% (27/197) for AdV vs 1% (2/200) vs 1.1% (2/175), p<0.0001; and 6.6% (13/197) for HPIV vs 0.5% (1/200) vs 1.1% (2/175), (p<0.0001).
With regard to seasonality, a significantly higher prevalence of influenza virus (p<0.0001) and RSV (p=0.029) was found during winter, with peaks in January-February. AdV peaked during winter 2018-2019 (p=0.004), while HCoV were detected with a significantly higher prevalence during winter 2019-2020 (p=0.037). With regard to HPIV, a significant peak from summer to fall 2018 was observed (p=0.016). Most viral respiratory infections have seasonal patterns and the prevalence of respiratory viruses varies according to the method, geographic area and population considered. Knowledge of local epidemiology is therefore crucial for implementation of prevention and treatment strategies.
Keywords: Respiratory tract infections, microbiology, multiplex real-time PCR, diagnosis, biostatistics.
INTRODUCTION
Acute respiratory infections represent a significant burden to society, being among the most frequent human diseases worldwide and viruses are frequently involved as etiologic agents [1-4]. Influenza virus, Respiratory Syncytial Virus (RSV), Human Parainfluenza Virus (HPIV), Human Metapneumovirus (HMPV), Rhinovirus (RV), Adenovirus (AdV) and the four endemic Human Coronaviruses (HCoV) -229E, -NL63, -OC43 and -HKU1 are the most common viruses involved in respiratory infections [3-5]. Among them, RSV is described as the leading cause of lower respiratory tract infection in children worldwide, while HMPV as the second most common [3-5]. On the other hand, RV and HCoV are the first and second most frequent causes of common cold, while both HPIV and AdV cause a wide spectrum of diseases, from common cold to pneumonia, mostly in relation to the immune status of the patient [3-5]. Influenza virus can cause mild to severe illness and is characterized mostly by fever, cough, sore throat and headache sometimes complicated by conditions as sinus and ear infections, pneumonia, myocarditis and encephalitis [3]. Antigen detection assays for influenza virus A/B and RSV are widely used. Nevertheless, a recent systematic review and meta-analysis, performed on 134 studies for influenza viruses and 32 for RSV, reported summary sensitivity and specificity for rapid tests of 61.1% and 98.9% for influenza and, 75.3% and 98.7% for RSV, respectively [6]. Molecular methods, such as Multiplex Real-Time PCR platforms are becoming more and more common in laboratories mostly in relation to the increased diagnostic sensitivity and reduced turnaround time [7, 8]. Multiplex Real-Time PCR platforms are also described as useful for epidemiological purposes and the knowledge of the local prevalence of respiratory viruses is of great importance for the development of prevention and treatment strategies [9, 10]. There are few studies that evaluated the prevalence of respiratory viruses in Italy by means of a Multiplex Real-Time PCR [11, 12]. The aim of this study was to assess the prevalence of respiratory viruses detected by Multiplex Real-Time PCR from nasopharyngeal swabs in the catchment area of the General Hospital of Alessandria, Italy.
MATERIALS AND METHODS
Design of the study
This is a retrospective analysis of results of Multiplex Real-Time PCR carried out on nasopharyngeal swabs processed as part of routine clinical care collected from consecutive patients with symptoms of respiratory infection in the catchment area (of about 200,000 people) of the S.S. Antonio e Biagio e Cesare Arrigo General Hospital of Alessandria, Italy, from January 2016 to June 2020. Patients were divided into three groups, according to Ambrosioni et al. [13]: pediatric (<18 years of age), adults (≥18 and <65 years of age), elderly (≥65 years of age).
Detection and identification of the respiratory viruses
The detection and identification of the respiratory viruses was performed by the FilmArray® Respiratory Panel (BioFire Diagnostics, Salt Lake City, Utah), a Multiplex nested PCR assay capable of identifying 17 viral and 3 bacterial targets. Viruses were AdV, HCoV-229E, -NL63, -OC43 and -HKU1, HMPV, RV/EV, influenza A (subtype H1, H1N1 and H3), influenza B, HPIV 1, 2, 3 and 4, and RSV; and bacteria Bordetella pertussis, Chlamydophila pneumoniae and Mycoplasma pneumoniae [14].
Statistical analysis
Values are expressed as median and interquartile range (IQR) or absolute numbers and percentage as appropriate. Differences between categorical variables were assessed using the Chi-square test. SPSS statistical package, release 17.0 (SPSS Inc, Chicago, IL, USA) was used for all statistical analyses. The significance level was set at p≤0.05.
Ethical considerations
The research has complied with all relevant international guidelines and institutional policies. Ethical approval was not needed because this is a retrospective analysis of data from samples collected as part of standard care and those included in the database were de-identified before access. No personal information was stored in the study database. No patient intervention occurred with the obtained results.
RESULTS
A total of 572 samples from as many patients were included in the study and 337/572 (58.9%) were from males. Pediatric patients were 197/572 (34.4%), adults 200/572 (35%) and elderly 175/572 (30.6%). The median age of the whole sample was 50 years (IQR: 6-68) and according to age groups, median values (IQR) were: 3 years (range 1-6) for the pediatric group; 52 years (range 43-57) among the adults and 73 years (range 70-79) in the elderly group.
Among all samples, 235/572 (41.1%) were positive for a respiratory virus and of them 189/235 (80.4%) were monomicrobial. The respiratory organisms detected in the whole sample are described in Figure 1. The prevalence was: 15.5% (89/572) of rhinovirus/enterovirus (RV/EV); 9.4% (54/572) of RSV; 8.9% (51/572) of influenza virus; 5.4% (31/572) of AdV; 3.1% (18/572) of HCoV; 2.8% (16/572) of HPIV; 2.3% (13/572) of HMPV. Rhinovirus/enterovirus were the pathogens most frequently involved in coinfections (34.7%, 16/46), followed by AdV (19.6%,9/46) and influenza virus (19.6%, 9/46).
No significant differences were found in detection rate between males and females. Otherwise, according to age range, samples collected from pediatric group were more frequently positive compared to adults and elderly, respectively.

Figure 1 - Respiratory organisms detected in the whole sample.
The prevalence of positive pediatric samples compared to the other groups was: 28.4% (56/197) for RV/EV vs 10.5% (21/200) vs 6.9% (12/175), p<0.0001; 18.8% (37/197) for RSV vs 2% (4/200) vs 7.4% (13/175), p<0.0001; 13.7% (27/197) for AdV vs 1% (2/200) vs 1.1% (2/175), p<0.0001; 6.6% (13/197) for HPIV vs 0.5% (1/200) vs 1.1% (2/175), p<0.0001. With regards to seasonality, trends for RV/EV, RSV, influenza virus, AdV, HCoV, HPIV and hMPV are described, respectively, in Figures 2 A-G.
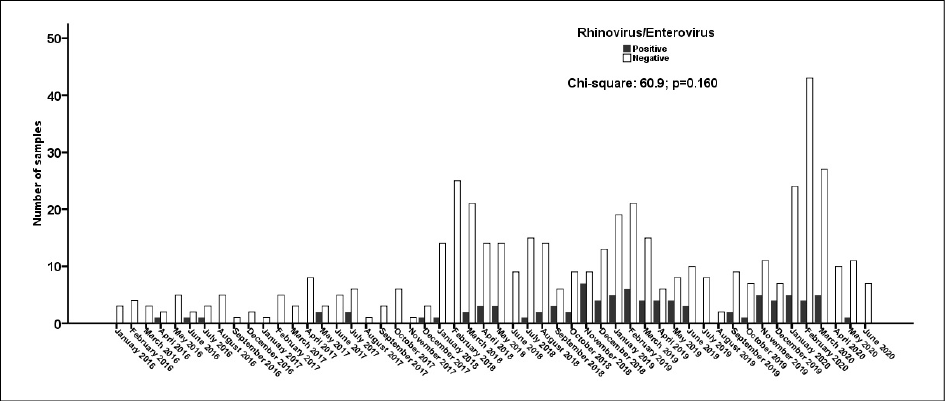
Figure 2A - Seasonal trend for rhinovirus/enterovirus.
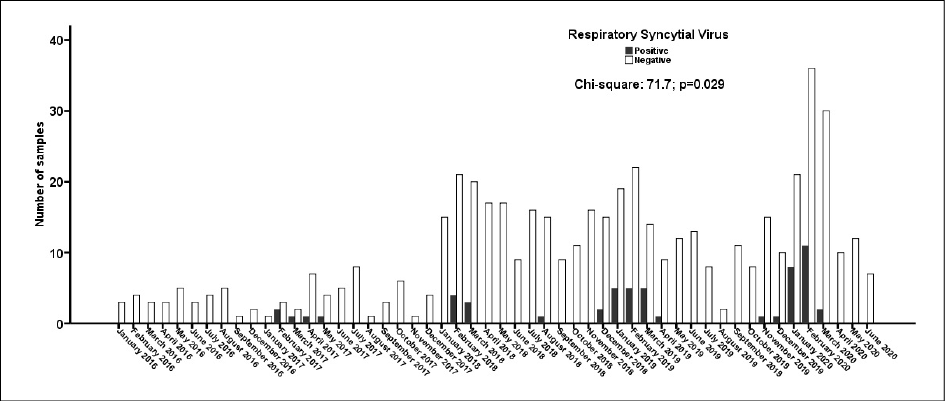
Figure 2B - Seasonal trend for respiratory syncytial virus.

Figure 2C - Seasonal trend for influenza virus A/B.

Figure 2D - Seasonal trend for adenovirus.

Figure 2E - Seasonal trend for endemic human coronaviruses -229E, -NL63, -OC43 and -HKU1.

Figure 2F - Seasonal trend for parainfluenza virus.

Figure 2G - Seasonal trend for human metapneumovirus.
DISCUSSION
In this study a greater positivity rate was found in the pediatric group, matching the results of Ambrosioni et al. that reported the highest positivity rate in upper respiratory samples collected from pediatric patients, with a similar overall positivity rate (43.2%) [13]. Similarly, also Jeon et al. found a higher positivity rate in the pediatric group compared to adults and elderly, along with a similar overall positivity rate (37.2%) [15].
Another result of this study was the higher proportion of samples found positive for RV/EV, followed by RSV and influenza virus. Also in the study of Ambrosioni et al. a higher proportion of samples were positive for picornavirus (that comprise RV/EV) in almost every population and both RSV and AdV were more frequently found in pediatric population [13]. In the study by Kim et al., a nation-wide surveillance, a greater prevalence of human RV and influenza virus was found, along with a higher coinfection rate by human RV and AdV, matching the results of the present study [16]. In the study by De Conto et al. the most frequent viruses detected in a pediatric population were RSV and AdV, but in that study RV were not evaluated [11]. Both in Jeon et al. and in Ye et al. influenza virus was the most commonly detected pathogen, nevertheless, in the former study more than half of the population was composed by adults, whereas in the latter only elderly patients (median age 73 years) were included [15, 17]. Finally, Botti et al. in a study performed in hospitalized children, found a greater prevalence of RV, followed by AdV, RSV and HPIV. Nevertheless, in that study the majority of the patients (89.6%) included were younger than 5 years of age [12].
With regard to seasonality, the higher prevalence of influenza virus and RSV during winter with peaks in January-February found in this study has been reported also by Ambrosioni et al. and De Conto et al. and, limited to influenza virus, also by Kim et al. and Ye et al. [11, 13, 16, 17]. RV/EV and AdV were detected throughout the period of the study, with a peak during winter 2018-2019 for AdV, in line with the results of the above mentioned studies [11, 13, 16]. Concerning HCoV and hMPV, the low positivity rates make it difficult to interpret the distribution of the data, nevertheless, for the former, a significantly higher prevalence during winter 2019-2020 was detected, while the latter was observed more frequently around March 2018, 2019 and 2020, although with no significant differences. Similarly, the prevalence of HPIV was low, nevertheless, a significant peak from summer to fall 2018 was observed. All these findings substantially match the results of other Authors [11-13, 16]. The comparison of seasonality patterns for Influenza virus and RSV with those of RV/EV and AdV found in this study confirms the epidemiological evidence described in the review by Moriyama et al., defining the former as winter viruses and the latter as all-year viruses [18].
Because of the ongoing pandemic of coronavirus disease 2019 (COVID-19) caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) the number of tests performed in the first semester of 2020 has grown by more than 30% compared to the same period in 2018 and 2019. Moreover, concerning the possible coinfection between the novel SARS-CoV-2 and the respiratory viruses evaluated in this study, only 50/572 (8.7%) of the samples were processed also for SARS-CoV-2 and no coinfection was noted. Although the number of tests performed does not allow to draw any conclusion, other Authors have found coinfection between SARS-CoV-2 and other respiratory viruses to be rare [19-21].
This study has limitations. First, unfortunately, clinical data were not available. Second, the sample size is small. Third, since this was a single center study, our findings might not be completely applicable to other contexts.
In conclusion, most viral respiratory infections have seasonal patterns and prevalence of respiratory viruses varies according to method, geographic area and population considered. The knowledge of local epidemiology is therefore crucial for implementation of prevention and treatment strategies.
Conflict of interest
All authors have no conflicts of interest to declare.
Funding
None.
REFERENCES
[1] Mulholland K. Global burden of acute respiratory infections in children: implications for interventions. Pediatr Pulmonol. 2003; 36 (6), 469-74.
[2] Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002; 2 (1), 25-32.
[3] van Doorn HR, Yu H. Viral Respiratory Infections. Hunter’s Tropical Medicine and Emerging Infectious Diseases. 2020: 284-8.
[4] Nichols WG, Peck Campbell AJ, Boeckh M. Respiratory viruses other than influenza virus: impact and therapeutic advances. Clin Microbiol Rev. 2008; 21 (2), 274-90.
[5] Weston S, Frieman MB. Respiratory Viruses. Encyclopedia of Microbiology. 2019; 85-101.
[6] Bruning AHL, Leeflang MMG, Vos JMBW, et al. Rapid Tests for influenza, respiratory syncytial virus, and other respiratory viruses: a systematic review and meta-analysis. Clin Infect Dis. 2017; 65 (6): 1026-32.
[7] Zhang N, Wang L, Deng X, et al. Recent advances in the detection of respiratory virus infection in humans. J Med Virol. 2020; 92 (4), 408-17.
[8] Hanson KE, Azar MM, Banerjee R, et al. Molecular testing for acute respiratory tract infections: clinical and diagnostic recommendations from the IDSA’s Diagnostics Committee. Clin Infect Dis. 2020; ciaa508.
[9] Esposito S, Mencacci A, Cenci E, Camilloni B, Silvestri E, Principi N. Multiplex Platforms for the Identification of Respiratory Pathogens: Are They Useful in Pediatric Clinical Practice? Front Cell Infect Microbiol. 2019; 9, 196.
[10] Diaz-Decaro JD, Green NM, Godwin HA. Critical evaluation of FDA-approved respiratory multiplex assays for public health surveillance. Expert Rev Mol Diagn. 2018; 18 (7), 631-43.
[11] De Conto F, Conversano F, Medici MC, et al. Epidemiology of human respiratory viruses in children with acute respiratory tract infection in a 3-year hospital-based survey in Northern Italy. Diagn Microbiol Infect Dis. 2019; 94 (3), 260-7.
[12] Botti C, Micillo A, Ricci G, et al. Characterization of respiratory infection viruses in hospitalized children from Naples province in Southern Italy. Exp Ther Med. 2018; 15 (6), 4805-9.
[13] Ambrosioni J, Bridevaux PO, Wagner G, Mamin A, Kaiser L. Epidemiology of viral respiratory infections in a tertiary care centre in the era of molecular diagnosis, Geneva, Switzerland, 2011-2012. Clin Microbiol Infect. 2014; 20 (9): O578-84.
[14] Babady NE. The FilmArray® respiratory panel: an automated, broadly multiplexed molecular test for the rapid and accurate detection of respiratory pathogens. Expert Rev Mol Diagn. 2013; 13 (8), 779-88.
[15] Jeon JH, Han M, Chang HE, et al. Incidence and seasonality of respiratory viruses causing acute respiratory infections in the Northern United Arab Emirates. J Med Virol. 2019; 91 (8), 1378-84.
[16] Kim JM, Jung HD, Cheong HM, et al. Nation-wide surveillance of human acute respiratory virus infections between 2013 and 2015 in Korea. J Med Virol. 2018; 90 (7), 1177-83.
[17] Ye C, Zhu W, Yu J, et al. Viral pathogens among elderly people with acute respiratory infections in Shanghai, China: preliminary results from a laboratory-based surveillance, 2012-2015. J Med Virol. 2017; 89 (10), 1700-6.
[18] Moriyama M, Hugentobler WJ, Iwasaki A. Seasonality of respiratory viral infections. Annu Rev Virol. 2020; 7 (1), 83-101.
[19] Nowak MD, Sordillo EM, Gitman MR, Paniz Mondolfi AE. Coinfection in SARS-CoV-2 infected patients: Where are influenza virus and rhinovirus/enterovirus? J Med Virol. 2020; 92 (10), 1699-1700.
[20] Siordia JA Jr. Epidemiology and clinical features of COVID-19: A review of current literature. J Med Virol. 2020; 127, 104357.
[21] Blasco ML, Buesa J, Colomina J, et al. Co-detection of respiratory pathogens in patients hospitalized with Coronavirus viral disease-2019 pneumonia. J Med Virol. 2020; 92 (10), 1799-1801.