Le Infezioni in Medicina, n. 1, 85-93, 2021
ORIGINAL ARTICLES
A study of group B streptococcus in pregnant women in Lebanon: prevalence, risk factors, vaginal flora and antimicrobial susceptibility
Wadha Alfouzan1,2, Nahed Gaddar3, Rita Dhar1, Ali A. Rabaan4
1Microbiology Unit, Department of Laboratories, Farwania Hospital, Kuwait;
2Department of Microbiology, Faculty of Medicine, Kuwait University, Kuwait;
3Biomedical Department, Lebanese International University, Lebanon;
4Molecular Diagnostic Laboratory, Johns Hopkins Aramco Healthcare, Dhahran, Saudi Arabia
Corresponding authors
Wadha Alfouzan
E-mail: Alfouzan.w@hsc.edu.kw
Ali A. Rabaan
E-mail: arabaan@gmail.com; ali.rabaan@jhah.com
SummaRY
Guidelines recommend universal screening of all pregnant women at 35-37 weeks of gestation for group B streptococcus (GBS) colonization and reserve a risk-factor-based approach for women who have no prenatal cultures. This study determines the prevalence of GBS among pregnant women in Lebanon and assesses the association between risk factors and vaginal flora in this patient population and antibiotic resistance pattern of the GBS isolates. Vaginal samples from women between 35-37 weeks of gestation were obtained and cultured on 5% sheep blood agar (BA), colistin nalidixic acid agar, Strep B Select chromogenic agar and Lim enrichment broth. Also, vaginal flora was evaluated on Gram-stained smears. Colonies on BA suggestive of GBS were identified by Gram staining, catalase test and agglutination in group B antiserum. Antimicrobial susceptibility to different antibiotics was tested on BA. Risk factors were obtained. The prevalence of vaginal GBS colonization was 18.4% (31/168). Evaluation of Gram-stained vaginal smears revealed an inverse relationship between the presence of lactobacilli and GBS colonization (p=0.029). Resistance of GBS to erythromycin and clindamycin was found to be 25.8% and 12.9%, respectively. Demographic and obstetric data did not reveal statistically significant differences in GBS colonization rates between age groups (p=0.498) or level of education (p=0.696) among these women. Prevalence of GBS remains high in this region with no identifiable risk factors for its acquisition. Furthermore, increase in resistance to erythromycin and clindamycin should prompt susceptibility testing of all GBS isolates. The resistance profile of these strains represents an emerging public health concern that needs further surveillance.
Keywords: Group B streptococcus, pregnant women, risk factors, prevalence, antimicrobial susceptibility
INTRODUCTION
Group B Streptococcus (GBS) has been well recognized worldwide as an important cause of maternal and neonatal morbidity and mortality [1-3]. GBS, also known as Streptococcus agalactiae, is part of the normal flora of genital tract and rectum. Even when present at these anatomical sites as a colonizer, it has been associated with higher risk for urinary tract infection and adverse pregnancy outcomes resulting in preterm birth, low birth weight, intrauterine death endometritis and chorioamnioitis [4-6]. Maternal GBS colonization can lead to colonization of 80% of the neonates increasing the risk of development of neonatal sepsis [4, 7].
Although asymptomatic colonization with GBS among pregnant and non-pregnant women is common worldwide, the prevalence varies from 6.5% to 43.6% in pregnant women [8,9] depending on the population studied at different geographical locations with variable characteristics such as age, parity, socio-economic status, sexually transmitted diseases and sexual behavior [10, 11].
GBS is one of the leading causes of perinatal bacterial infections, being commonly responsible for septicemia and meningitis in neonates [12]. A direct correlation between the prevalence of GBS carriage in pregnant women and the rate of occurrence of neonatal GBS infection would be considered rational. Since the burden of perinatal GBS disease varies between countries, preventive measures have been adopted by some and not by others. For example, European countries, which do not have high GBS prevalence like USA, do not recommend screening of all pregnant women for GBS [13].
Based on a large population-based study, the Centers for Disease Control and Prevention (CDC) of the United States currently recommends screening of all pregnant women for GBS between 35-37 weeks of gestation [2]. Intrapartum Antibiotic Prophylaxis (IAP) is recommended during labor for those who test positive for GBS. Since the implementation of this strategy there has been a 79% decline in early-onset neonatal infections, especially in most high-income countries [14].
The aim of this prospective, cross-sectional study was to determine the prevalence of vaginal GBS colonization and to assess the associated risk factors for its acquisition among pregnant women in Lebanon. Furthermore, because of increasing evidence suggesting that the vaginal microbiome is an important determinant of pathogens, such as Escherichia coli and Gardnerella spp. colonization, we evaluated the potential relationship of lactobacilli in vaginal flora to GBS colonization [15,16]. In order to study the impact of optimal strategy of antibiotic utilization, antimicrobial susceptibility pattern of GBS isolates from pregnant women was also determined.
PATIENTS AND METHODS
This study was conducted with approval from Ethics Committee of the participating hospitals (Saint George, Makassed and Clemenceaue Medical Center) in Beirut, Lebanon.
Sample collection
Vaginal specimens (duplicate swabs) from pregnant women at 35-37 weeks of gestation attending antenatal clinic of obstetrics and gynecology department were collected by the attending physician. A predesigned questionnaire (Figure 1) was used for recording socio-demographic and relevant obstetric data from each participant.

Figure 1 - Group B streptococcus Colonization Study - Questionnaire.
Microbiology
One of the two samples received from each patient was used to inoculate Tryptic soy agar with 5% sheep blood (BA), Columbia agar with 5% blood supplemented with nalidixic acid and colistin (CNA) and StrepB Select agar, following which the swab was immersed in Lim broth (Todd Hewitt broth) supplemented with 10 mg nalidixic acid/L and 15 mg/L of colistin whereas the second swab was used to prepare a Gram-stained smear. All the cultured plates and broth were incubated overnight at 35-37oC following which the enrichment broth was sub-cultured on to all the three agar plates as the primary culture. GBS were identified presumptively by colony morphology (hemolytic or non-hemolytic), Gram stain and catalase test. The identification was confirmed by Vitek 2 (bioMérieux, France) and positive reaction in latex agglutination test with group B antiserum in the streptococcus grouping kit (Oxoid, Basingstoke, UK). Susceptibility to antibiotics (penicillin, cefotaxime, erythromycin, clindamycin and vancomycin) was determined by Kirby-Bauer disk diffusion method using Mueller-Hinton agar with 5% sheep blood. The results were interpreted according to CLSI recommendations. GBS strain (ATCC BAA-611) was used as the susceptible control. The Gram-stained direct smear was examined and evaluated for bacterial vaginosis according to Nugent criteria [17] as well as for Candida vaginitis.
Statistical analysis
The prevalence was estimated in terms of frequencies and percentages. Then the factors that influence the prevalence of GBS carriage among Lebanese women were explored. For this, a bivariate analysis was applied, considering presence of GBS as dependent variable and age group, level of education, previous bad outcomes of pregnancy, clinical states, and current treatment as independent variables. All variables involved in the study were handled as categorical variables in order to use Chi square test for comparing their proportions with alpha=0.05. The antibiotic susceptibility profiles (susceptible vs. resistant) for the isolated GBS strains were studied. Percentages of susceptibility were compared for each antibiotic using the Chi-square test for proportions.
RESULTS
Prevalence
Among Lebanese pregnant women who participated in the study the prevalence of GBS was determined to be 18.4% (31/168) based on vaginal swab cultures. There were no data available for rectal swabs as none were obtained.
Associated risk factors
The study identified the correlation between GBS colonization and presence of certain maternal risk factors in this study population. Table 1 summarizes the rate of GBS colonization by socio-demographic characteristics, maternal obstetric history and clinical status. Although GBS were more often isolated from women ≤25 years (22.6%) as compared to those >30 years (14.8%), the difference was not statistically significant (p=0.498).
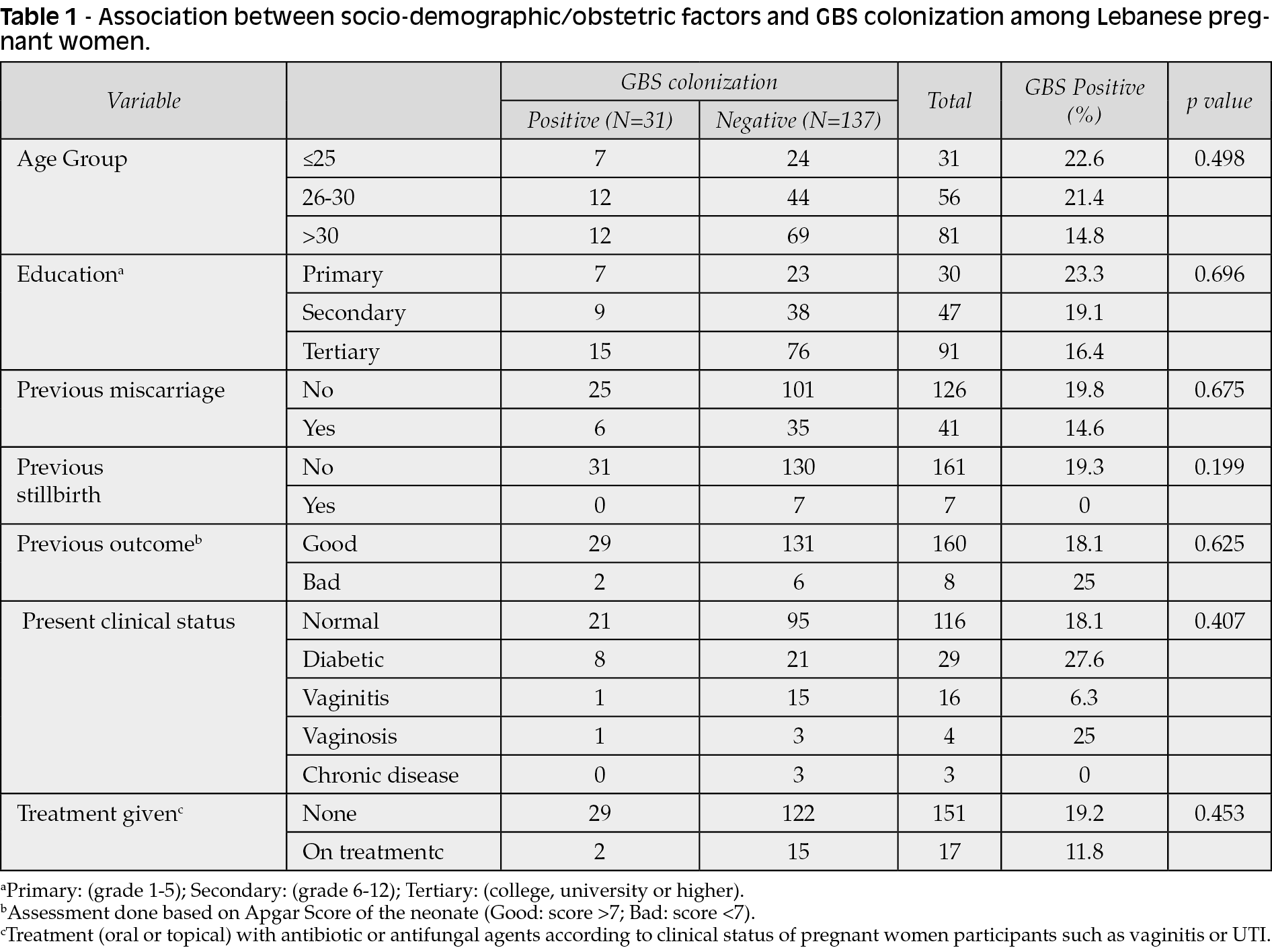
It was observed that GBS carriage rate was inversely proportional to the educational status of the women, being higher (23.3%) in those with primary level education versus 16.5% in those with post-secondary level education. Furthermore, presence of GBS in lower genital tract of these women was not found to be associated with any adverse perinatal outcomes during previous pregnancies. Of 29 pregnant women who were diagnosed with diabetes mellitus during antenatal period, only 8 (27.6%) harbored GBS in the vagina.
Associated variables detected by Gram-stained smear examination
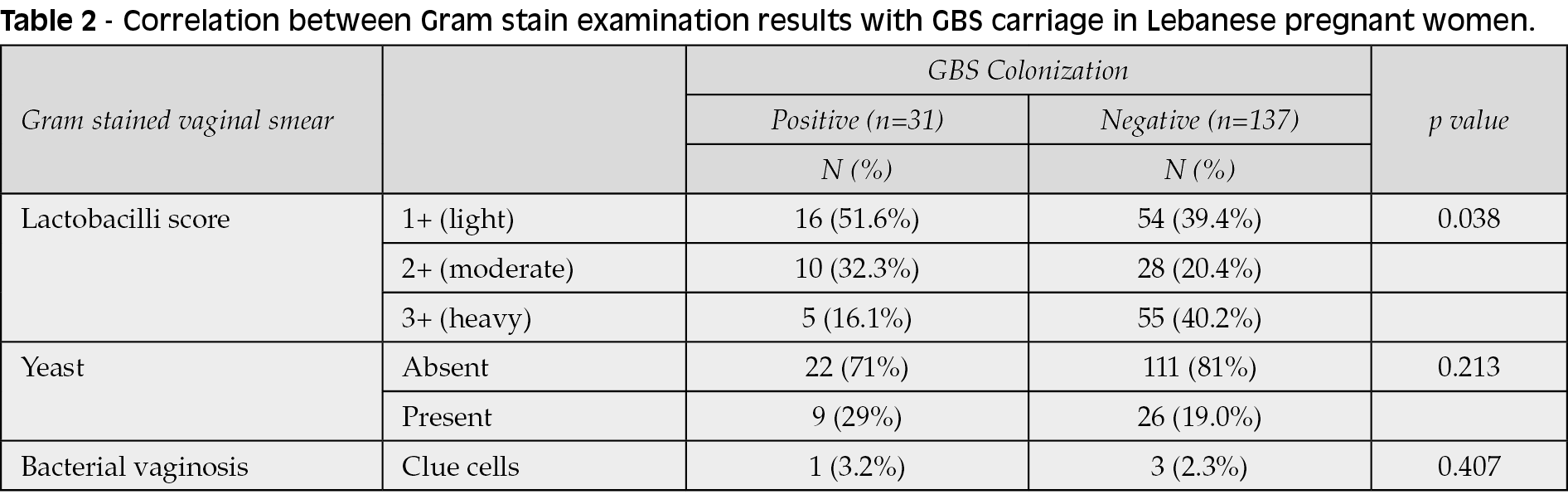
Direct Gram-stained smears of all vaginal samples collected were carefully examined to obtain a Nugent score. Briefly, the smears were evaluated on a scale of 1+ and 4+ for the presence of lactobacilli; presence or absence of ‘clue cells’ and yeast cells. The results obtained were then correlated with the isolation of GBS in these cases (Table 2). Lower score for lactobacilli was found to be inversely associated with GBS carriage (p=0.029). However, vaginal colonization with GBS was not associated with diagnosis of bacterial vaginosis in this obstetric population under study. Also, only 29% of women with GBS-positive vaginal cultures showed concomitant presence of yeast cells in the smear.
Antimicrobial susceptibility profile
Among 31 GBS isolates 100% of them were susceptible to penicillin, cefotaxime and vancomycin. However, resistant rates against erythromycin and clindamycin were found to be 25.8% (8/31) and 12.9% (4/31), respectively (Table 3).

DISCUSSION
Variable rates of vaginal GBS carriers, ranging from 4% to 26.5% among pregnant women have been reported previously from various developed and developing countries [8, 9, 18, 19]. The prevalence of GBS colonization (18.5%) among Lebanese pregnant women was found to be slightly higher than a global prevalence rate of 17.9% as determined in a recent meta-analysis [18-20]. Although studies from different countries have shown that the prevalence of GBS colonization is unstable, it is interesting to note that wide variation can also be found in different regions of the same country. For example, in a study from Greece, the vaginal colonization among women in Athens was found to be 7% as compared to 12% in pregnant women from South-Western Greece [21]. Similarly, the colonization rates reported from different regions of Ethiopia varied from 9% to 19% in previous studies [22]. This may explain a lower rate of GBS carriage (13.4%) among women in a study from Saudi Arabia, which shares a part of its Northern border with Kuwait where the GBS carriage rate was found to be 18.5% [4]. Earlier studies from Kuwait during 1999-2001 and Lebanon during 2006 reported the incidence of GBS colonization as 16.4% and 17.7%, respectively [23, 24]. Differences in prevalence may also be attributed to variation in the culture and non-culture techniques employed and the clinical samples used for GBS culture [25]. In a report from the United States, the prevalence of GBS carriage was determined to be 20.6% by culture and latex agglutination methods in rectal and vaginal specimens from pregnant women [26]. The rates of recto-vaginal and vaginal GBS colonization were found to be similar (11.9% vs 10.9%) in a study from Iran [16]. However, there are several reports indicating higher GBS isolation rates from rectal swabs as compared to genital swabs hypothesizing that gastrointestinal tract is the primary site of GBS carriage, which may lead to vaginal colonization [18, 27-29, 30, 31]. Potentially, therefore, the rate of GBS carriage among Lebanese pregnant women may be higher than observed in our study since only vaginal swabs were studied. Several studies have compared detection of GBS carriage by ‘real-time’ Polymerase Chain Reaction (PCR) with standard microbiological culture and found the latter to be highly accurate with the advantage of rapid turn-around-time of <2 h [32]. However, despite being a useful tool to determine GBS rate in the urgent intrapartum setting a false negative rate of 13.2% was obtained in a study whereas PCR assays performed comparably to culture of intrapartum vaginal samples in another study [33, 34].
The heterogeneity in the vaginal GBS carriage rate has been associated with geographic, ethnic and socioeconomic factors [4]. In addition, nutritional status, sexually transmitted diseases, host immunity and sexual behavior have also been implicated [35, 36]. Since 50% of neonates born to colonized women acquire GBS during perinatal period and 1%-2% of these colonized neonates develop invasive disease, it is imperative to determine the risk factors for acquisition and colonization of pregnant women with GBS [22]. There have been many studies which compared different variables with GBS colonization in these subjects. However, no consistent relationship between these factors and GBS colonization has emerged from these studies. Although in our study we demonstrated higher rates of GBS colonization in younger (<25 years) women and in those with primary level education only, the differences were not statistically significant. Our findings are supported by a previous report from Kuwait, which also showed no significant difference in the ages of GBS carriers [23]. Previously, a couple of studies have revealed that women who did not receive any formal education were more likely to be colonized with GBS. The lack of knowledge about personal hygiene has been implicated for this association [10, 37]. Although no significant difference in the results concerning obstetric history such as previous miscarriages or stillbirths related to GBS carriage was observed in our study a higher incidence of previous recurrent spontaneous miscarriages (17.0%) was reported in a study from Kuwait [23]. Other causes of miscarriages have been attributed to silent infections caused by Ureaplasma spp., Mycoplasma spp., and Chlamydia trachomatis, which have a prevalence of 1%-3% [38]. However, some of the previous studies have shown a definite relationship between some of socio-demographic factors (maternal age, marital status, education level, number of sexual partners etc.) and or obstetric factors (gestational age, parity, previous obstetric history, dysuria, vaginal discharge etc.) with GBS colonization [13, 21, 24, 25, 35, 36, 39]. One of the studies from Africa determined the association of HIV infection in pregnant women with GBS carriage but failed to find any correlation [22]. In a multiplexed polymerase chain reaction amplification of 16S ribonucleic acid (rRNA) in vaginal swabs, vaginal microbiome was analyzed in Guatemalan women [18]. This study revealed higher relative abundance of lactobacilli among GBS-colonized women than in GBS-noncolonized women (89.9% vs 51.0%). Although in the present study vaginal smears were analyzed by Gram stain, an inverse correlation of proportion of lactobacilli colonization was observed in GBS-colonized women as compared to those who were not colonized with GBS (Table 3). GBS disease in neonates with mothers who screened negative have also been studied. Maternal age <18 years and black race have been identified as high-risk factors for early-onset GBS disease [40] whereas breast milk has been implicated in late-onset GBS disease [41].
The CDC advocates testing of GBS isolates for susceptibility to clindamycin and erythromycin, as these are considered the drugs of choice for penicillin-allergic women at high risk for anaphylaxis [2]. In our study, while all GBS isolates were determined to be susceptible to penicillin, cefotaxime and vancomycin, 25.8% and 12.9% GBS isolates were found to be resistant to erythromycin and clindamycin, respectively as compared to resistance of 0.7% and 1.7% to erythromycin and clindamycin, respectively in an earlier study from Kuwait [42]. More recently, in 2011, another study from Kuwait showed GBS resistance to erythromycin to be12.6% and 7.0%for clindamycin [43] whereas a study from Lebanon reported the resistance percentages for GBS isolates in 2009 as 11.8% and 15.8% for clindamycin and erythromycin, respectively [44]. Antibiotic susceptibility profile of GBS isolates in studies [4, 21, 22, 37, 42-48] from various geographical locations during the period extending from 2003 to 2018 is presented in Table 3. Although Antimicrobial Susceptibility Testing (AST) is not possible with the PCR strategy, it has been assumed that susceptibility testing is not necessary as all GBS strains are uniformly susceptible to beta-lactam antibiotics [49]. However, resistance to some of the beta-lactam antibiotics, including third-generation cephalosporins have been reported in a few studies [22, 37, 46, 48]. It may therefore become customary to perform AST on all GBS isolates. This gradual increase in antimicrobial resistance has been attributed to overuse or frequent misuse of antibiotics necessitating regular evaluation of GBS antibiotic profile especially in those women who are found to be allergic to penicillin [36].
CONCLUSIONS
Since the association between GBS colonization and underlying risk factors were not found to be of statistical significance it is difficult to identify high-risk women for whom selective screening might be appropriate. Greater understanding of the risk factors for GBS colonization will help in making adjustment for the use of preventive therapies when the culture results are not available.
Conservative use of antibiotics would be recommended for treatment of genital tract infections during pregnancy so as to obviate any possible adverse effects of antibiotics on the vaginal microbiome of the mother and help in preservation of healthy vaginal environment so as to prevent infection due to other potential pathogens and also prevent emergence of drug resistance among bacteria. Furthermore, administration of probiotics has been shown to maintain vaginal microbiome and normal urogenital health to prevent or treat infections [50, 51].
Conflict of interest
None declared.
Funding
No funding sources.
REFERENCES
[1] Edward MS, Nizet V. Group B streptococcal infections. In: Jack S, Remington JS, Klein JO, Wilson CB, Nizet V, Maldonado YA, editors (7th ed.). Infectious diseases of the fetus and newborn infant, Philadelphia: WB Saunders. 2011: 417-67.
[2] Prevention of perinatal group B streptococcal disease: a public health perspective, Centers for Disease Control and Prevention, MMWR Recomm Rep. 1996; 45 (RR-7), 1-24.
[3] Schrag S, Gorwitz R, Fultz-Butts K, Schuchant A. Prevention of perinatal streptococcal disease. Revised guidelines for CDC, MMWR Recomm Rep. 2002; 51 (RR-11), 1-22.
[4] Khan MA, Faiz A, Ashshi AM. Maternal colonization of group B streptococcus: prevalence, associated factors and antimicrobial resistance. Ann Saudi Med. 2015; 35 (6), 423-7.
[5] Winn HN. Group B streptococcus infection in pregnancy. Clin Perinatol. 2007; 34 (3), 387-92.
[6] Tyrrell GJ, Senzilet LD, Spika JS, et al. Invasive disease due to group B streptococcal infection in adults: results from a Canadian, population-based, active laboratory surveillance study-1996. Sentinel Health Unit Surveillance System Site Coordinators. J Infect Dis. 2000; 82 (1), 168-73.
[7] Schuchat A. Group B streptococcal disease in newborns: a global perspective on prevention. Biomed Pharmacother. 1995; 49 (1), 19-25.
[8] Yucesoy G, Caliskan E, Karadenizli A, et al. Maternal colonization with Group B streptococcus and effectiveness of a culture-based protocol to prevent early-onset neonatal sepsis. Int J Clin Pract. 2004; 58 (8), 735-9.
[9] Gavino M, Wang E. A comparison of a new rapid real-time polymerase chain reaction system and traditional culture in determining Group B streptococcus colonization. Am J Obstet Gynecol. 2007; 197 (4), 388.e1-4.
[10] Regan JA, Klebanoff MA, Nugent RP. The epidemiology of Group B streptococcal colonization in pregnancy. Vaginal infections and Prematurity Study Group. Obstet Gynecol. 1991; 77 (4), 604-10.
[11] Foxman B, Gillepsie BW, Manning SD, Marrs CF. Risk factors for Group B streptococcal colonization: potential for different transmission systems by capsular types. Ann Epidemiol. 2007; 17 (11), 854-62.
[12] Edmond KM, Kortsalioudaki C, Scott S, et al. Group B streptococcal disease in infants aged younger than 3 months: systematic review and meta-analysis. Lancet. 2012; 379 (9815), 547-56.
[13] Kim EJ, Oh KY, Kim MY, et al. Risk factors for Group B streptococcus colonization among pregnant women in Korea. Epidemiol Health. 2011; 33, e2011010.
[14] Verani JR, McGee L, Schrag SJ. Prevention of perinatal Group B streptococcal disease-revised guidelines from CDC, 2010. MMWR Recomm Rep. 2010; 59 (RR-10), 1-36.
[15] Dangor Z, Kwatra G, Izu A, at al. Association between maternal Group B Streptococcus surface-protein antibody concentrations and invasive disease in their infants. Expert Rev Vaccines. 2015; 14 (12), 1651-60.
[16] Moghaddam MN. Recto-vaginal colonization of Group B Streptococcus in pregnant women referred to a hospital in Iran and its effect on lactobacillus normal flora. J Biol Sci. 2010; 10 (2), 166-9.
[17] Nugent RP, Kohn MA, Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991; 29 (2), 297-301.
[18] Rick AM, Aguilar A, Cortes R, et al. Group B streptococci colonization in pregnant Guatemalan women: prevalence, risk factors and vaginal microbiome. Open Forum Infect Dis. 2017; 4 (1), ofx020.
[19] Ghaddar N, AlFouzan W, Anastasiadis E, et al. Evaluation of chromogenic medium and direct latex agglutination test for detection of group B streptococcus in vaginal specimens from pregnant women in Lebanon and Kuwait. J Med Microbiol. 2014; 63 (Pt 10), 1395-9.
[20] Kwatra G, Cunnington MC, Merrall E, et al. Prevalence of maternal colonization with group B streptococcus: a systematic review and meta-analysis. Lancet Infect Dis. 2016; 16 (9), 1076-84.
[21] Tsolia M, Psoma M, Gavrili S, et al. Group B streptococcus colonization of Greek pregnant women and neonates: prevalence, risk factors and serotypes. Clin Microbiol Infect. 2003; 9 (8), 832-8.
[22] Mengist A, Kannan H, Abdissa A. Prevalence and antimicrobial susceptibility pattern of anorectal and vaginal. Group B streptococci isolates among pregnant women in Jimma, Ethiopia. BMC Res Notes. 2016; 9, 351-5.
[23] Al Sweih N, Maiyegun S, Diejomaoh M, et al. Streptococcus agalactiae (group B streptococci) carriage in late pregnancy in Kuwait. Med Princ Pract. 2004; 13 (1), 10-4.
[24] Seoud M, Nassar AH, Zalloua P, et al. Prenatal and neonatal Group B streptococcus screening and serotyping in Lebanon: incidence and implications. Acta Obstet Gynecol Scand. 2010; 89 (3), 399-403.
[25] Eren A, Kakercan M, Oguzoglu N, Unal N, Karateka A. The carriage of Group B streptococci in Turkish pregnant women and its transmission rate in newborns and serotype distribution. Turk J Pediatr. 2005; 47 (1), 28-33.
[26] Park CJ, Vandel NM, Ruprai DK, Martin EA, Gates KM, Coker D. Detection of group B streptococcal colonization in pregnant women using direct latex agglutination testing of selective broth. J Clin Microbiol. 2001; 39 (1), 408-9.
[27] Badri MS, Zawaneh S, Cruz AC, et al. Rectal colonization with group B streptococcus: relation to vaginal colonization of pregnant women. J Infect Dis. 1977; 135 (2), 308-12.
[28] Anthony BF, Eisenstadt R, Carter J, Kim KS, Hobel CJ. Genital and intestinal carriage of group B streptococci during pregnancy. J Infect Dis. 1981; 143 (6), 761-6.
[29] Hoogkamp-Korstanje JA, Gerards LJ, Cats BP. Maternal carriage and neonatal acquisition of group B streptococci. J Infect Dis. 1982; 145 (6), 800-3.
[30] Schrag SJ, Zell ER, Lynfield R, et al. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. N Engl J Med. 2002; 347 (4), 233-9.
[31] Valkenburg-van den Berg AW, Sprij AJ, Oostvogel PM, et al. Prevalence of colonisation with group B Streptococci in pregnant women of a multi-ethnic population in The Netherlands. Eur J Obstet Gynecol Reprod Biol. 2006; 124 (2), 178-83.
[32] El Helali N, Nguyen JC, Ly A, Giovangrandi Y, Trinquart L. Diagnostic accuracy of a rapid real-time polymerase chain reaction assay for universal intrapartum group B streptococcus screening. Clin Infect Dis. 2009; 1, 49 (3), 417-23.
[33] Atkins KL, Atkinson RM, Shanks A, Parvin CA, Dunne WM, Gross G. Evaluation of polymerase chain reaction for group B streptococcus detection using an improved culture method. Obstet Gynecol. 2006; 108 (3 Pt 1), 488-91.
[34] Andreasen T, Kjølseth Møller J, Rohi Khalil M. Comparison of BD MAX GBS and GenomEra GBS assays for rapid intrapartum PCR detection of vaginal carriage of group B streptococci. PLoS One. 2019; 14 (4), e0215314.
[35] Jahromi BN, Poorarian S, Poorbarfehee S. The prevalence and adverse effects of Group B streptococcal colonization during pregnancy. Arch Iranian Med. 2008; 11 (6), 654-7.
[36] Davies HD, Adair CE, Partlow ES, Sauve R, Low DE, McGeer A. Two-year survey of Alberta laboratories processing of antenatal Group B streptococcal (GBS) screening specimens: implications for GBS screening programs. Diag Microbiol Infect Dis. 1999; 35 (3), 169-76.
[37] Joachim A, Matee MI, Massawe FA, Lyamuya EF. Maternal and neonatal colonisation of group B streptococcus at Muhimbili National Hospital in Dar es Salaam, Tanzania: prevalence, risk factors and antimicrobial resistance. BMC Public Health. 2009; 9, 437.
[38] Contini C, Rotondo JC, Magagnoli F, et al. Investigation on silent bacterial infections in specimens from pregnant women affected by spontaneous miscarriage. J Cell Physiol. 2018; 234 (1), 100-7.
[39] Rocchetti TT, Marconi C, Rall VL, Borges VT, Carrente JE, do Sliva MG. Group B streptococci colonization in pregnant women: risk factors and evaluation of the vaginal flora. Arch Gynecol Obstet. 2011; 283 (4), 717-21.
[40] Parente V, Clark RH, Ku L. Risk factors for group B streptococcal disease in neonates of mothers with negative antenatal testing. J Perinatol. 2017; 37 (2), 157-61.
[41] Nicolini G, Borellini M, Loizzo V, Creti R, Memo L,
Berardi A. Group B streptococcus late-onset disease, contaminated breast milk and mothers persistently GBS negative: report of 3cases. BMC Pediatr. 2018; 18 (1), 214.
[42] Al-Sweih N, Jamal M, Kurdia M, Abduljabar R, Rotimi V. Antibiotic susceptibility profile of group B streptococcus (Streptococcus agalactiae) at the Maternity Hospital, Kuwait. Med Princ Pract. 2005; 14 (4), 260-3.
[43] Boswihi SS, Udo EE, Al-Sweih N. Serotypes and antibiotic resistance in Group B streptococcus isolated from patients at the Maternity Hospital. J Med Microbiol. 2012; 61 (Pt 1), 126-31.
[44] Hannoun A, Shehab M, Khairallah MT, et al. Correlation between Group B Streptococcal Genotypes, Their Antimicrobial Resistance Profiles, and Virulence Genes among Pregnant Women in Lebanon. Int J Microbiol. 2009; 2009, 796512.
[45] Simoes JA, Aroutcheva AA, Heimler I, Faro S. Antibiotic resistance patterns of group B streptococcal clinical isolates. Infect Dis Obstet Gynecol. 2004; 12 (1), 1-8.
[46] Shabayek SA, Abdalla SM, Abouzeid AM. Vaginal carriage and antibiotic susceptibility profile of group B Streptococcus during late pregnancy in Ismailia, Egypt. J Infect Public Health. 2009; 2 (2), 86-90.
[47] Sharmila V, Joseph NM, Arun Babu T, Chaturvedula L, Sistla S. Genital tract group B streptococcal colonization in pregnant women: a South Indian perspective. J Infect Dev Ctries. 2011; 5 (8), 592-5.
[48] Assefa S, Desta K, Lema T. Group B streptococci vaginal colonization and drug susceptibility pattern among pregnant women attending in selected public antenatal care centers in Addis Ababa, Ethiopia. BMC Pregnancy Childbirth. 2018; 18 (1), 135.
[49] Schuchat A, Zywicki SS, Dinsmoor MJ, et al. Risk factors and opportunities for prevention of early-onset neonatal sepsis: a multicenter case-control study. Pediatrics. 2000; 105 (1 Pt 1), 21-6.
[50] Keski-Nisula L, Kyynarainen HR, Karkkainen U, Karhukorpi J, Heinonen S, Pekkanen J. Maternal intrapartum antibiotics and decreased vertical transmission of Lactobacillus to neonates during birth. Acta Paediatr. 2013; 102 (5), 480-5.
[51] Borges S, Silva J, Teixeira P. The role of lactobacilli and probiotics in maintaining vaginal health. Arch Gynecol Obstet. 2014; 289 (3), 479-89.