Le Infezioni in Medicina, n. 1, 1-9, 2021
REVIEWS
COVID-19-associated coagulopathy: a concise review on pathogenesis and clinical implications
Sahar Memar Montazerin1, Homa Najafi1, Fahimehalsadat Shojaei1, Gerald Chi1, Sogand Goudarzi1, Sadaf Sharfaei2, Farima Kahe1, Shakiba Hassanzadeh3
1Division of Cardiovascular Medicine, Department of Medicine, Beth Israel Deaconess Medical Center,
Harvard Medical School, Boston, MA 02215, USA;
2Baim Institute for Clinical Research, Boston, MA 02215, USA;
3Acquired Immunodeficiency Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
Corresponding author
Shakiba Hassanzadeh
E-mail: shak.hassanzadeh@gmail.com
SummaRY
In this review, we summarize the possible mechanisms of COVID-19-associated coagulopathy and compare its features to other similar conditions. The recent COVID-19 pandemic has caused enormous mortality and morbidity worldwide. It is important to note that COVID-19-associated thrombotic events play a huge role in the morbidity of this disease. Interestingly, it has been observed that this complication may occur despite prophylactic anticoagulant therapy. Recent studies on COVID-19-associated coagulopathy revealed that the COVID-19-associated hypercoagulability is more frequently observed among those with a severe course of the disease. Various mechanisms have been suggested as explanations for this condition and possible underlying etiologies.
Keywords: COVID-19, endothelium, inflammation, SARS-CoV-2, thrombosis.
INTRODUCTION
Since the emergence of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection, coronavirus disease 2019 (COVID-19)-associated coagulopathy has gained significant attention. It is associated with a more severe course of the disease and poor prognosis [1, 2]. The hallmark of COVID-19-associated coagulopathy is the prominent elevation of D-dimer, which is a biomarker of fibrinolysis and a predictor of thrombosis. It has been demonstrated that the incidence of arterial thrombosis is higher among COVID-19 patients as well [3]. The pathologic manifestations of vascular involvement include thrombosis, hemorrhage, edema, inflammation, and endothelial cell death. Both pulmonary and non-pulmonary vessels have been shown to be affected in COVID-19. There is growing evidence indicating that thrombosis in pulmonary vasculature may play a role in the COVID-19-associated Acute Respiratory Distress Syndrome (ARDS) and respiratory failure. For example, in one study, the microscopic pathology of the lung of a patient with COVID-19 infection revealed small vessel stenosis and occlusion [4]. In addition, studies have shown that COVID-19 may affect vessels of different sizes in different organs. This different vascular selectivity may be the result of differential expression of molecular surface antigens required for the infectivity of this organism [5]. There are many evidences that indicate a higher tendency toward thrombotic events in COVID-19-induced ARDS compared to ARDS due to non-SARS-CoV-2 infections. Virchow’s triad is known as the cornerstone of thrombotic events. The three-arms of this triad include endothelial damage, hypercoagulability, and blood stasis. The contribution of each of these arms may vary in different thrombotic events [6]. This article reviews the current understandings of the potential underlying mechanisms of COVID-19-associated coagulopathy.
SARS-CoV-2 pathogenesis
It has been suggested that Angiotensin-Converting-Enzyme-2 (ACE-2) is the primary molecular surface element used by SARS-CoV-2 for entrance to the human cells [5]. Interestingly, the loss or gain of function of this protein (ACE-2) has been shown to affect the endothelial cell-protective barriers in the experimental studies. Other studies have shown that ACE-2 has anti-inflammatory and antioxidant effects [7]. Given that these cell surface antigens are the primary barrier disrupted by the COVID-19 virus, the cells rich in these antigens, such as the pneumocytes and endothelial cells, may be involved in the pathogenesis of this viral infection [8]. Studies have shown that SARS-CoV-2 infection reduces ACE-2 and subsequently increases angiotensin II (AT-II) [9]. In addition, it is known that AT-II is associated with hypertension and recent data have implicated the role of AT-II in the pathogenesis of thrombus formation in the arterioles. In fact, in animal model studies, chronic AT-II infusion has increased platelet-endothelial cell adhesion and enhanced thrombogenesis within the arterial system. Also, increased AT-II has been associated with an increase in tissue factor expression, which is a known factor of coagulation cascade activation [10]. These data provide evidence that the AT-II upregulation may be another piece of the coagulation pathway activation puzzle. A summary of COVID-19-coagulopathy is shown in Figure 1.

Figure 1 - Overview of the pathogenesis of COVID-19-associated coagulopathy. Endotheliopathy (as a consequence of direct viral invasion or local/systemic inflammatory response) and increase in angiotensin II have been implicated in orchestrating the coagulopathy in COVID-19. In conjunction with hypercoagulable state, endothelial injury and altered blood flow dynamics constitute the Virchow’s triad and increase the risk of thrombotic complications.
Altered coagulation biomarkers
Studies on patients with severe COVID-19 infection have shown the presence of elevated levels of D-dimer and Fibrin Degradation Product (FDP), and prolonged Prothrombin Time (PT), and activated Partial Thromboplastin Time (aPTT). Also, it has been consistently suggested that elevated levels of D-dimer indicate poor prognosis and higher mortality rates [8]. It is worth mentioning that, D-dimer levels tend to rise as the course of the disease deteriorates [2]. Platelet count is another potential marker that is subject to change in patients affected by COVID-19. In contrast to sepsis-induced coagulopathy, thrombocytopenia is not prevalent among patients with COVID-19. However, low platelet count has been recognized as a marker of disease severity [11]. In some studies, thrombocytosis was similarly associated with a more severe course of the COVID-19 infection, and patients with high platelet counts were reported to have longer hospital stays [12]. In addition, higher serum levels of Von Willebrand Factors (VWF) were also reported in patients with SARS-CoV-2 coagulopathy complications [5]. Another laboratory marker of undetermined significance is the presence of antiphospholipid antibodies in some COVID-19 patients. In a study of 56 COVID-19 patients, about 45% of the participants had lupus anticoagulant antibodies in their serum. Although acute infections may result in the transient appearance of these antibodies, the clinical significance of this association needs to be elucidated [13, 14]. Another interesting finding is that the presence of lupus anticoagulant was associated with aPTT prolongation in these patients. The clinical importance of this finding is that the prolonged aPTT may adversely affect the clinical decision on administrating anticoagulants in these patients and may in turn result in increased thromboembolic conditions [15].
Hemostasis in COVID-19 infection
Considering the change in coagulation biomarkers, patients with COVID-19 infection may be prone to thromboembolic events. It is of particular note that these thromboembolic events may occur while the patients were receiving heparin or enoxaparin for venous thromboembolism (VTE) prophylaxis [16-18]. For example, one study on patients with severe COVID-19 infection showed that about 71% of the cases fulfilled the criteria of the International Society on Thrombosis and Haemostasis (ISTH) criteria for disseminated intravascular coagulation (DIC) [19]. Unlike bacterial-induced DIC, in COVID-19-associated DIC, there is a modest level of thrombocytopenia and high levels of fibrinogen. Bacterial-induced DIC is usually associated with low levels of these markers [2].
Endothelial damage in COVID-19 infection
As mentioned earlier, SARS-CoV-2 infects the cells by disrupting the ACE-2 receptors. Endothelial cells highly express these surface antigens and therefore are highly involved in the COVID-19 infection. This endothelial damage may promote the activation of the inflammatory response which consequently mounts a hypercoagulable state in the body that may be another potential mechanism causing COVID-19-coagulopathy [20]. Additionally, ACE-2 downregulation results in a decreased level of anti-inflammatory agents and endothelial damage, which may also be another potential mechanism in COVID-19-induced coagulopathy [21]. There is evidence demonstrating the presence of platelet-fibrin thrombi within the vessel wall of different organs in COVID-19 infected patients which was consistent among multiple studies analyzing post-mortem histopathology of various organ tissues in patients with COVID-19 infection [22, 23].
Inflammatory cytokines and COVID-19 infection
Recent studies investigating the levels of inflammatory cytokines in patients with COVID-19 revealed that severe cases had higher levels of circulatory IL-6, IL-10, TNFα, and IL-2 receptor compared to less severe cases [24, 25]. The rapid increase in circulating levels of these core pro-inflammatory cytokines has been known to cause a clinical syndrome, cytokine release syndrome, that presents with high fevers, headache, low blood pressure, night sweats, and multi-organ dysfunction and is associated with poor prognosis. However, it is notable that this syndrome is not unique to COVID-19 infection [25]. The role of IL-6 in COVID-19-associated complications has been investigated in multiple studies. IL-6 plays multiple roles in the inflammatory pathways including synthesis of coagulation factors, platelet production, and vascular permeability [5]. These factors may also contribute to COVID-19-associated coagulopathy. Considering these functions, some studies targeted the receptor of this cytokine as a potential treatment of COVID-19 infection and interestingly their results were promising [26, 27]. In line with IL-6, COVID-19 infection has been associated with increased pro-inflammatory cytokines and chemokines such as Tumor Necrosis Factor (TNF)-α, IL-1β, and Monocyte Chemoattractant Protein (MCP)-1 [24]. These elements recruit more immune cells to the infected organs and provide an environment for the expression of other factors including the tissue factor that is associated with coagulation cascade initiation [9].
Heparin-induced thrombocytopenia and COVID-19 infection
Heparin-Induced Thrombocytopenia (HIT) has been a well-known complication of anticoagulant therapy with heparin-derivative medications. It is particularly common among those receiving heparin compared to low molecular weight heparin. In the absence of heparin exposure, studies suggest the presence of a syndrome that manifests with a similar clinical picture as HIT [28]. This syndrome, spontaneous HIT, has been reported in COIVD-19 patients and should be considered as a potential cause of COVID-19-associated coagulopathy [29].
COVID-19-associated coagulopathy compared to other causes of coagulopathy
COVID-19-associated coagulopathies should be differentiated from bacterial-induced DIC and other thrombotic microangiopathies. The pathogenesis of bacterial-induced DIC and coagulopathy involves pro-inflammatory cytokines and other host defense mechanisms mentioned earlier for COVID-19. However, a key distinction of sepsis-induced DIC is the lack of increase in D-dimer levels with increasing disease severity when compared with non-sepsis induced DIC [30,31]. In other words, the sepsis-induced DIC is associated with progressive clot formation and suppressed fibrinolysis. This suppressed fibrinolysis, also referred to as fibrinolytic shutdown, is due to an increase in the production of plasminogen activator inhibitor-1 [32]. Additionally, COVID-19 infection is characterized by high circulatory levels of VWF, and may manifest with a clinical vignette similar to Thrombotic Thrombocytopenic Purpura (TTP). TTP is a micro thrombotic condition associated with depleted levels of a metalloproteinase, ADAMS 13, which is responsible for VWF cleavage. The lack of ADAMS 13 activity in TTP results in the release of VWF multimers and microthrombi formation in the small vessels and a constellation of symptoms manifesting with thrombocytopenia, fever, decreased consciousness, and renal failure. COVID-19 infection, in contrast to TTP, has not been associated with a decrease in ADAMS 13 levels. Another unique feature of COVID-19 infection in comparison to TTP is its relationship with venous thromboembolism rather than stroke and arterial thrombosis more commonly seen in TTP [28].
COVID-19-associated coagulopathy occurs despite anticoagulant administration
Pulmonary emboli and arterial thrombotic events have been reported in patients with influenza pneumonia while receiving VTE prophylaxis. Although the exact mechanism of this finding remains to be elucidated, one study suggested that influenza A/H1N1 infection is associated with hypercoagulability and endothelial activation or dysfunction [33]. In line with this finding, thrombotic events have been observed in patients with COVID-19 who were receiving the prophylactic dose of anticoagulant agents. A report from France demonstrated a higher incidence of thromboembolic events in patients with COVID-19-associated Acute Respiratory Distress Syndrome (ARDS) compared to non-COVID-19-associated ARDS despite anticoagulation therapy [34]. Another report from the Netherlands showed an incidence of 31% of thrombotic events in Intensive Care Unit (ICU) patients with COVID-19 who have received at least the standard doses of thromboprophylaxis [35]. Although some authors argued that this phenomenon occurred due to underdosing of anticoagulant agents and the invalidity of data, such events show the necessity of venous thromboembolism risk stratification and consideration of appropriate anticoagulant prophylactic dose while managing patients with this infection [19]. Another point to be considered while managing patients with COVID-19-associated coagulopathy is the laboratory findings and their potential effects on coagulopathy indexes. An abnormally prolonged aPTT was hypothesized to be the reason for insufficient or avoidance of prophylactic or therapeutic dose of anticoagulant therapy in patients with COVID-19 [15].
Clinical features of COVID-19-associated coagulopathy
COVID-19-associated thrombotic events have been reported between 16% and 31% in patients with severe SARS-CoV-2 infection [35-37]. Recent data has also shown that venous thromboembolic events are more frequent than arterial events. COVID-19-associated coagulopathy may manifest with venous thromboembolic events, arterial thrombotic events, and microangiopathic events. Arterial thrombotic events, such as stroke are less common among patients with COVID-19. However, in a recent study done in New York, COVID-19 infection was associated with a higher incidence of stroke as compared to influenza infection. This study demonstrated that a total of 31 out of 1916 patients with COVID-19 infection developed acute ischemic stroke [38]. Bleeding or overt DIC has been rarely reported. In half of the cases, the events would be diagnosed within 24 hours of admission [36].
Evaluation of thromboembolic events in COVID-19 infection
The ISTH has released a guidance statement on the evaluation and management of COVID-19-associated coagulopathy. It recommended daily measurement of D-dimer, PT, and platelet count as well as serum fibrinogen level (if feasible) in all hospitalized patients with COVID-19. These laboratory findings have prognostic values and can guide clinicians for future clinical decision making. Worsening of these markers necessitate the consideration of more aggressive critical care support or the administration of experimental therapies and blood product support [39]. On the other hand, if clinical condition and coagulation markers are stabilized or improved, step-down of treatment may be considered.
In hospitalized COVID-19 patients, the Working Party on Hemostasis (Swiss Society of Hematology) recommended regular (daily or 2-3 times/week) monitoring of PT, D-dimer, fibrinogen, platelet count, lactate dehydrogenase (LDH), creatinine, and alanine aminotransferase (ALT) [40]. If there is an indication, such as renal impairment, monitoring of anti-Xa activity should be considered as well. It did not recommend monitoring for antithrombin unless there is DIC, sepsis-induced coagulopathy, or heparin resistance. In addition, in cases with changes in platelet counts or signs of heparin resistance, HIT should be considered [40].
A summary of the recommendations for the evaluation of thromboembolic events in COVID-19 shown in Table 1.

Currently, there is insufficient evidence to recommend routine imaging in evaluating thromboembolic events in COVID-19 patients. Furthermore, there is an overlap of clinical manifestations of COVID-19-associated ARDS or pneumonia with COVID-19-associated pulmonary embolism. However, some studies suggest using Computed Tomography (CT) pulmonary angiography in patients with COVID-19 who present with sudden onset of worsening pulmonary manifestations and high level of D-dimer [41].
Management of coagulopathy in COVID-19 infection
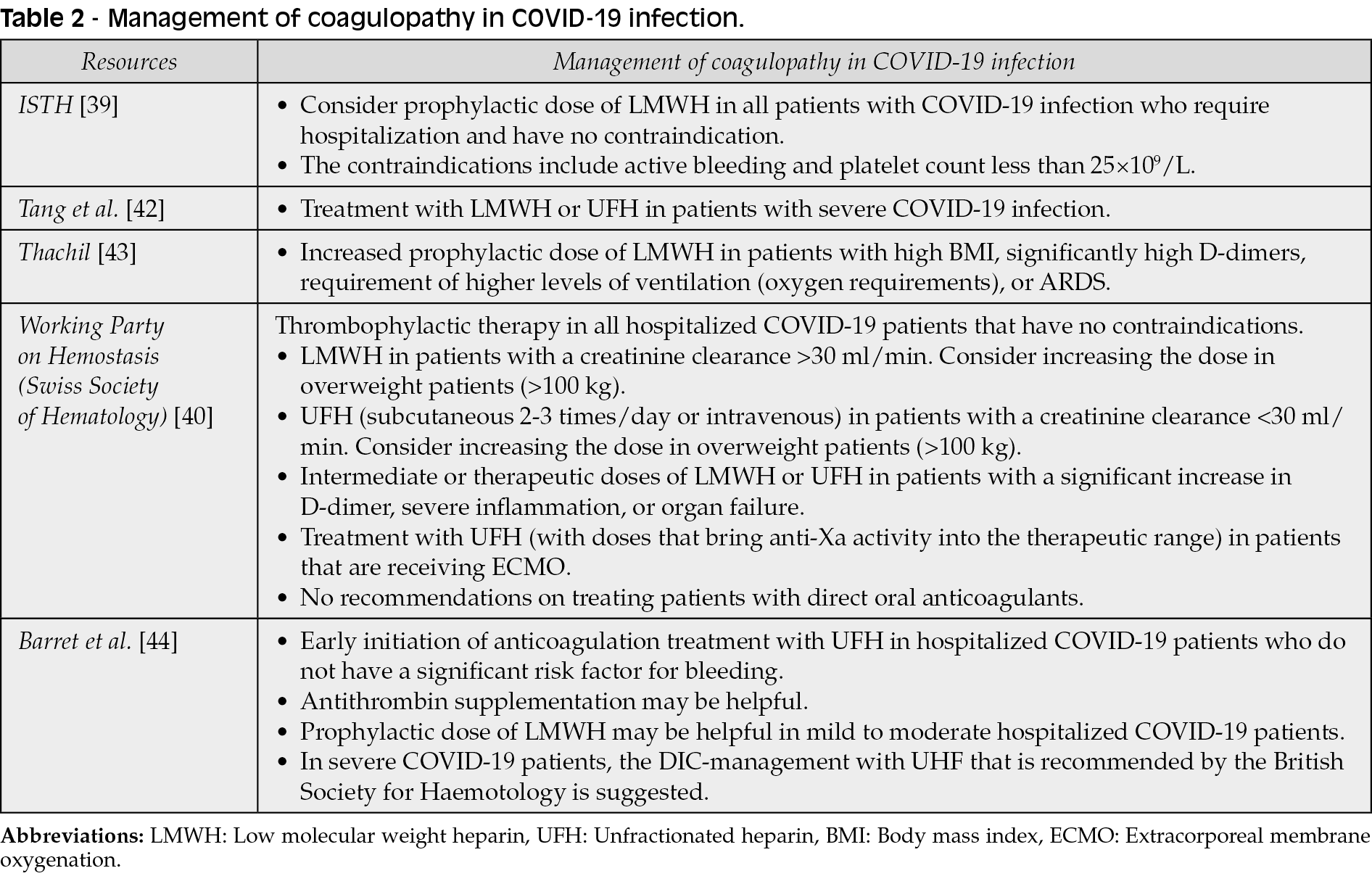
According to ISTH interim guidance statement, prophylactic dose of Low Molecular Weight Heparin (LMWH) should be considered in all patients with COVID-19 infection who require hospitalization and have no contraindication. The contraindications include active bleeding and platelet count less than 25×109/L [39].
Tang et al. have reported that in patients with severe COVID-19 infection, treatment with LMWH or unfractionated heparin (UFH) is associated with a better prognosis, and the mortality of patients who received treatment was lower in those who had sepsis-induced coagulopathy (SIC) score ≥4 or D-dimer >6-fold of upper limit compared to those who did not receive treatment [42].
Thachil suggested that patients with COVID-19 infection may require higher dose of LMWH, such as an increased prophylactic dose of LMWH in patients with high Body Mass Index (BMI), significantly high D-dimers, or requirement of higher levels of ventilation (oxygen requirements), or ARDS [43].
The Working Party on Hemostasis (Swiss Society of Hematology) recommended thrombophylactic therapy in all hospitalized COVID-19 patients that have no contraindications [40]. Patients that have a creatinine clearance >30 ml/min should receive LMWH, but consider increasing the dose in overweight patients (>100 kg). However, those who have a creatinine clearance <30 ml/min should receive UFH (subcutaneous 2-3 times/day or intravenous) but consider increasing the dose in overweight patients (>100 kg) [40]. Additionally, intermediate or therapeutic doses of LMWH or UFH is recommended in patients with a significant increase in D-dimer, severe inflammation, or organ failure. Treatment with UFH (with doses that bring anti-Xa activity into the therapeutic range) should be considered in patients that are receiving extracorporeal membrane oxygenation (ECMO). However, they did not have any recommendations on treating patients with direct oral anticoagulants due to lack of evidence [40].
Barret et al. have commented on the ISTH interim guidance statement by that in some patients, thrombotic events continue to occur despite prophylactic therapy [44]. They suggested early initiation of anticoagulation treatment with UFH in hospitalized COVID-19 patients who do not have a significant risk factor for bleeding. They also suggested that antithrombin supplementation may be helpful [44]. Barret et al. discussed that in mild to moderate hospitalized COVID-19 patients, the prophylactic dose of LMWH may be effective. However, severe COVID-19 patients may progress to hypercoagulability and DIC-related organ failure, and they suggested the DIC-management with UHF that is recommended by the British Society for Haemotology [44]. In addition, COVID-19 patients have been found to have higher levels of fibrinogen and lower levels of antithrombin. Since increased serum levels of fibrinogen reduce the efficacy of prophylactic therapy in preventing thrombosis, prophylactic doses of LMWH and UFH may be less effective in severe COVID-19 patients [44, 45]. Increased levels of fibrinogen causes thrombosis and levels >900 mg/dL increase blood viscosity with low shear, therefore aggressive anticoagulation therapy may prevent multi-organ failure and ARDS [44]. Additionally, since there is a high rate of pulmonary embolism in patients with COVID-19 patients, Barret et al. suggested that UFH may be a better choice because these patients required administration of tissue Plasminogen Activator (tPA), and treating patients with tPA in those who have received LMWH may increase the risk of unstoppable bleeding. Furthermore, renal failure is common in COVID-19 patients which makes UFH a better choice in these patients. [44].
A summary of the recommendations for the management of coagulopathy in COVID-19 patients is shown in Table 2.
A potential combination therapy with heparin and nafamostat has been suggested [46]. Nafamostat is a serine protease inhibitor that inhibits proteolytic enzymes (such as thrombin, plasmin, and trypsin) and has antifibrinolytic actions [47]. It has been used in treating DIC in Japan for over 30 years [46]. Further studies are required to assess the efficacy of nafamostat in treating coagulopathy in COVID-19 patients.
Currently, there are several clinical trials around the world investigating the effects of various drug regimen on COVID-19-associated coagulopathy.
An important consideration while managing thromboembolic events in patients with COVID-19 is potential drug-drug interactions, particularly in patients with inherited bleeding disorders. Another point to remember is considering the potential inherited bleeding disorders while initiating anticoagulant agents for these patients.
As discussed earlier, coagulation biomarkers may be affected according to the severity of the infection. For example, lupus anticoagulant may transiently turn positive in patients with COVID-19 and results in a prolongation of aPTT. Having this in mind, prolonged aPTT should not prevent the administration of appropriate thromboprophylaxis medications in these individuals [48].
The use of extended post-discharge thromboprophylaxis has also been highlighted in patients with comorbidities leading to an increased risk of coagulopathic events [6].
CONCLUSION
Thromboembolism has been proposed as a potential culprit of increased mortality in the COVID-19 era. Although currently speculative, COVID-19-induced coagulopathy may be a distinct entity that involves multiple pathways, including inflammation, activation of endothelial cells, and imbalance of pro- and anti-coagulant proteins. Future research is required to address the appropriate venous thromboembolism prophylaxis in these patients.
Conflict of interest
Authors have no conflict of interest to declare.
Funding
None
REFERENCES
[1] Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020; 18 (4), 844-7.
[2] Al-Ani F, Chehade S, Lazo-Langner A. Thrombosis risk associated with COVID-19 infection. A scoping review. Thromb Res. 2020; 192, 152-60.
[3] Mehra MR, Desai SS, Kuy S, Henry TD, Patel AN. Cardiovascular disease, drug therapy, and mortality in COVID-19. N Engl J Med. 2020; 382 (25): e102.
[4] Luo W, Yu H, Gou J, et al. Histopathologic findings in the explant lungs of a patient with COVID-19 treated with bilateral orthotopic lung transplant, Transplantation. 2020; 104 (11), e329-31.
[5] Labò N, Ohnuki H, Tosato G. Vasculopathy and Coagulopathy Associated with SARS-CoV-2 Infection. Cells. 2020; 9 (7), 1583.
[6] Becker RC. COVID-19 update: Covid-19-associated coagulopathy. J Thromb Thrombolysis. 2020; 50 (1), 54-67.
[7] Zhu L, Carretero OA, Xu J, et al. Activation of angiotensin II type 2 receptor suppresses TNF-α-induced ICAM-1 via NF-κB: possible role of ACE2. Am J Physiol Heart Circ Physiol. 2015; 309 (5), H827-34.
[8] Iba T, Levy JH, Levi M, Thachil J. Coagulopathy in COVID-19. J Thromb Haemost. 2020; 18 (9), 2103-9.
[9] Bautista-Vargas M, Bonilla-Abadía F, Cañas CA. Potential role for tissue factor in the pathogenesis of hypercoagulability associated with in COVID-19. J Thromb Thrombolysis. 2020; 50 (3), 479-83.
[10] Senchenkova EY, Russell J, Esmon CT, Granger DN. Roles of Coagulation and Fibrinolysis in Angiotensin II-Enhanced Microvascular Thrombosis. Microcirculation. 2014; 21 (5), 401-7.
[11] Lippi G, Plebani M, Henry BM. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: a meta-analysis. Clin Chim Acta. 2020; 506, 145-8.
[12] Qu R, Ling Y, Zhang Yhz, et al. Platelet-to-lymphocyte ratio is associated with prognosis in patients with coronavirus disease-19. J Med Virol. 2020; 92 (9), 1533-41.
[13] Harzallah I, Debliquis A, Drénou B. Lupus anticoagulant is frequent in patients with Covid-19. J Thromb Haemost. 2020; 18 (8), 2064-5.
[14] Devreese K, Ortel T, Pengo V, De Laat B, Antibodies SoLAA. Laboratory criteria for antiphospholipid syndrome: communication from the SSC of the ISTH. J Thromb Haemost. 2018; 16 (4), 809-13.
[15] Bowles L, Platton S, Yartey N, et al. Lupus anticoagulant and abnormal coagulation tests in patients with Covid-19. N Engl J Med. 2020; 16, 383 (3), 288-90.
[16] Cui S, Chen S, Li X, Liu S, Wang F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J Thromb Haemost. 2020; 18 (6), 1421-4.
[17] Hanify JM, Dupree LH, Johnson DW, Ferreira JA. Failure of chemical thromboprophylaxis in critically ill medical and surgical patients with sepsis. J Crit Care. 2017; 37, 206-10.
[18] Chi G, Lee JJ, Jamil A, et al. Venous thromboembolism among hospitalized patients with covid-19 undergoing thromboprophylaxis: a systematic review and meta-analysis. J Clin Med. 2020; 9 (8), 2489.
[19] Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020; 75 (23), 2950-73.
[20] O’Sullivan JM, Mc Gonagle D, Ward SE, Preston RJ, O’Donnell JS. Endothelial cells orchestrate COVID-19 coagulopathy. The Lancet Haematol. 2020; 7 (8), e553-5.
[21] Marchandot B, Sattler L, Jesel L, Matsushita K, Schini-Kerth V, Grunebaum L, et al. COVID-19 Related Coagulopathy: a distinct entity? J Clin Med. 2020; 9 (6), 1651.
[22] Carsana L, Sonzogni A, Nasr A, et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: a two-centre descriptive study. Lancet Infect Dis. 2020; 20 (10), 1135-40.
[23] Wichmann D, Sperhake J-P, Lütgehetmann M, et al. Autopsy findings and venous thromboembolism in patients with COVID-19: a prospective cohort study. Ann Intern Med. 2020; 173 (4), 268-77.
[24] Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. 2020; 395 (10223), 497-506.
[25] Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest. 2020; 130 (5), 2620-9.
[26] Moore JB, June CH. Cytokine release syndrome in severe COVID-19. Science. 2020; 368 (6490), 473-4.
[27] Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab treatment in COVID-19: A single center experience. J Med Virol. 2020; 92 (7), 814-8.
[28] Iba T, Levy JH, Connors JM, Warkentin TE, Thachil J, Levi M. The unique characteristics of COVID-19 coagulopathy. Crit Care. 2020; 24 (1), 1-8.
[29] Liu X, Zhang X, Xiao Y, al. Heparin-induced thrombocytopenia is associated with a high risk of mortality in critical COVID-19 patients receiving heparin-involved treatment. medRxiv. 2020. doi: https://doi.org/10.1101/2020.04.23.20076851
[30] Madoiwa S, Nunomiya S, Ono T, et al. Plasminogen activator inhibitor 1 promotes a poor prognosis in sepsis-induced disseminated intravascular coagulation. Int J Hematol. 2006; 84 (5), 398-405.
[31] Semeraro F, Ammollo CT, Caironi P, Masson S, Latini R, Panigada M, et al. Low D-dimer levels in sepsis: Good or bad? Thrombosis research. 2019; 174, 13-5.
[32] Iba T, Levy JH. Sepsis-induced coagulopathy and disseminated intravascular coagulation. Anesthesiology. 2020; 132 (5), 1238-45.
[33] Bunce PE, High SM, Nadjafi M, Stanley K, Liles WC, Christian MD. Pandemic H1N1 influenza infection and vascular thrombosis. Clin Infect Dis. 2011; 52 (2), e14-7.
[34] Helms J, Tacquard C, Severac F, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020; 46 (6), 1089-98.
[35] Klok F, Kruip M, Van der Meer N, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020; 191, 145-7.
[36] Lodigiani C, Iapichino G, Carenzo L, et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res. 2020; 191, 9-14.
[37] Bilaloglu S, Aphinyanaphongs Y, Jones S, Iturrate E, Hochman J, Berger JS. Thrombosis in hospitalized patients with COVID-19 in a New York City Health System. JAMA. 2020; 324 (8), 799-801.
[38] Merkler AE, Parikh NS, Mir S, et al. Risk of ischemic stroke in patients with coronavirus disease 2019 (COVID-19) vs patients with influenza. JAMA Neurol. 2020; 77 (11), 1366-72.
[39] Thachil J, Tang N, Gando S, Falanga A, Cattaneo M, Levi M, et al. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J Thromb Haemost. 2020; 18 (5), 1023-6.
[40] Casini A, Alberio L, Angelillo-Scherrer A, Fontana P, Gerber B, Graf L, et al. Thromboprophylaxis and laboratory monitoring for in-hospital patients with COVID-19 - a Swiss consensus statement by the Working Party Hemostasis. Swiss Med Wkly. 2020; 150: w20247.
[41] Rotzinger D, Beigelman-Aubry C, von Garnier C, Qanadli S. Pulmonary embolism in patients with COVID-19: time to change the paradigm of computed tomography. Thromb Res. 2020; 190, 58-9.
[42] Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020; 18 (5), 1094-9.
[43] Thachil J. The versatile heparin in COVID-19. J Thromb Haemost. JTH. 2020; 18 (5), 1020-2.
[44] Barrett CD, Moore HB, Yaffe MB, Moore EE. ISTH interim guidance on recognition and management of coagulopathy in COVID-19: A comment. J Thromb Haemost. 2020; 18 (8), 2060-3.
[45] Harr JN, Moore EE, Chin TL, et al. Postinjury hyperfibrinogenemia compromises efficacy of heparin-based venous thromboembolism prophylaxis. Shock (Augusta, Ga). 2014; 41 (1), 33-9.
[46] Asakura H, Ogawa H. Potential of heparin and nafamostat combination therapy for COVID-19. J Thromb Haemost. 2020; 18 (6), 1521-2.
[47] Aoyama T, Ino Y, Ozeki M, Oda M, Sato T, Koshiyama Y, et al. Pharmacological studies of FUT-175, nafamstat mesilate. I. Inhibition of protease activity in in vitro and in vivo experiments. Japan J Pharmacol. 1984; 35 (3), 203-27.
[48] Zhang Y, Xiao M, Zhang S, et al. Coagulopathy and antiphospholipid antibodies in patients with Covid-19. New Engl J Med. 2020; 382 (17), e38.